
Abstract
BACKGROUND AND PURPOSE: We conducted a retrospective evaluation of the results of endovascular treatment (EVT) of middle cerebral artery aneurysms (MCAAs) in a center where embolization is the first treatment option considered.
MATERIALS AND METHODS: Ninety-two MCAAs were diagnosed in 87 patients between September 2001 and January 2006. The strategy of treatment (endovascular versus surgical), the clinical and angiographic results of embolization, and the ensuing complications are described.
RESULTS: Initially, 59 aneurysms (64.1%) in 55 patients were embolized, 18 (19.6%) were clipped, and 15 (16.3%) were not treated. Four endovascular procedures failed (7.3%), and 55 aneurysms in 51 patients were finally treated by embolization. During the procedure, complications occurred in 13 patients (25.5%) comprising 3 ruptures and 10 thromboembolisms. In the follow-up, 4 patients having a preoperative complication had a modified Rankin scale more than 2 (3 patients [5.9%]) or died (1 patient [2.0%]). Of the 55 embolized aneurysms, according to the Raymond scale, 23 (41.8%) were completely occluded, 24 (43.6%) retained a residual neck, and 8 (14.6%) were residual at the end of the first procedure. No bleeding was detected during the follow-up period in the embolized patients.
CONCLUSION: EVT of MCAA is effective for preventing rebleeding episodes within the first year of treatment judging by historical controls. The real question is whether clipping or coiling of MCAAs is better in terms of reducing rebleeding rates and complications rates in the long term, and such a determination would require a far larger number of patients over a much longer observation period.
The International Subarachnoid Aneurysm Trial (ISAT) did much to prove the efficacy and safety of the endovascular treatment (EVT) of ruptured cerebral aneurysms.1 However, for middle cerebral artery aneurysms (MCAAs), surgery remains often the first-line treatment. This is mainly because of the anatomic characteristics of these aneurysms, which often have wide necks and branches arising from the neck, and also because of their proximity to the cerebral surface, which facilitates surgical access.2–5 The aim of this study was, therefore, to analyze retrospectively the feasibility and efficacy of ruptured and unruptured MCAA embolization in a center where this option is the first one considered.
Patients and Methods
Between September 2001 and January 2006, we conducted a search for all of the MCAAs angiographically confirmed by the neuroradiology department in a hospital responsible for a population of approximately 250,000 people. Ninety-two MCAAs were found in 87 patients. Women constituted 63% of the population studied. Patients were aged between 24 and 76 years (mean, 49 years). Clinical presentation, symptoms, the size and shape of the aneurysmal sac, and the patient age were evaluated by the referring neurosurgeon and the neurointerventionist. Decision of treatment (clipping versus coiling) was made by a multidisciplinary team involving neuroanesthesiologists, neurosurgeons, and neuroradiologists after completion of the initial angiogram (multiple projections and 3D angiogram). Surgical treatment was the first option in case of compressive hematomas or aneurysms with large neck and branches arising from them. In the other cases, priority was given to EVT. All of the patients were classified according to the Hunt and Hess grading scale (HHGS) to determine the clinical severity of the subarachnoid hemorrhage (SAH) and also according to the modified Rankin scale (mRS) to assess the clinical results recorded at the patient's last follow-up consultation (Table 1).
Patient characteristics, clinical data, aneurysm size, and outcome of 55 patients with middle central artery aneurysms treated by endovascular coiling
Treatment was performed within 3 days of SAH. General anesthesia was administered to all of the patients, and a femoral approach with a 6F sheath was used in all of the cases. The approach was bifemoral when the balloon-remodeling technique was performed. On the basis of the images generated by 3D rotational acquisition, 1 or 2 working projections that gave the best achievable view of the aneurysmal neck were defined. After placement of the sheath, 5000 IU of heparin were administered as an intravenous bolus injection and then continuously infused at a rate of 2500–3000 IU per hour throughout the procedure. In addition, 500 mg of aspirin were administered intravenously when aneurysms were not ruptured. In most cases, heparin was discontinued after embolization.
All of the adverse events were registered and reported in the present article even if no clinical consequence was observed.
Patients were clinically evaluated postoperatively, 1 month, 3 months, and 1 year after the treatment by the neurosurgeon. The neuroradiologists performed anatomic follow-up, including immediate postoperative angiography, 3-month MR angiography (MRA), and 12-month MRA and digital subtraction angiography (DSA). Subsequent follow-up was performed by MR imaging and MRA. The angiographic results were interpreted independently by one of us by chart review, using Raymond classification (Figure 1).6

Raymond classification for aneurysmal occlusions. (Reproduced with permission from Roy D, Milot G, Raymond J. Endovascular treatment of unruptured aneurysms. Stroke 2001;32:1998–2004.)
Results
Initial Treatment Technique
Between September 2001 and January 2006, 92 MCAAs were diagnosed; 49 of them were ruptured, and 43 were unruptured. For 59 MCAAs (64.1%), EVT was considered feasible and was, therefore, tried first. For 18 aneurysms (19.6%), this treatment was not considered a good indication, and they were assigned to surgery. Fifteen of the 92 MCAAs diagnosed (16.3%) were not treated (Fig 2). Seventy seven were, therefore, treated, 59 (76.6%) by endovascular coiling, and 18 (23.4%) by surgical clipping. The reasons for assigning 18 MCAAs to surgery were as follows: 10 had wide neck with incorporation of an MCA branch (4 of them unruptured), 4 were ruptured microaneurysms (diameter, 2–3 mm), 3 exhibited a voluminous hematoma, and 1 of the patients (with 1 aneurysm) had chronic renal insufficiency. Twelve of the 15 untreated patients had unruptured aneurysms. They were composed of 1 patient with MCA branches arising from the sac, 8 patients with microaneurysms (2- to 3-mm wide with large necks), 1 patient with a calcified aneurysm, 1 with a thrombosed aneurysm, and 1 with chronic renal insufficiency. The remaining 3 untreated patients were grade V on the HHGS (Table 2). Remodelling technique was used in 4 cases (6.8%).
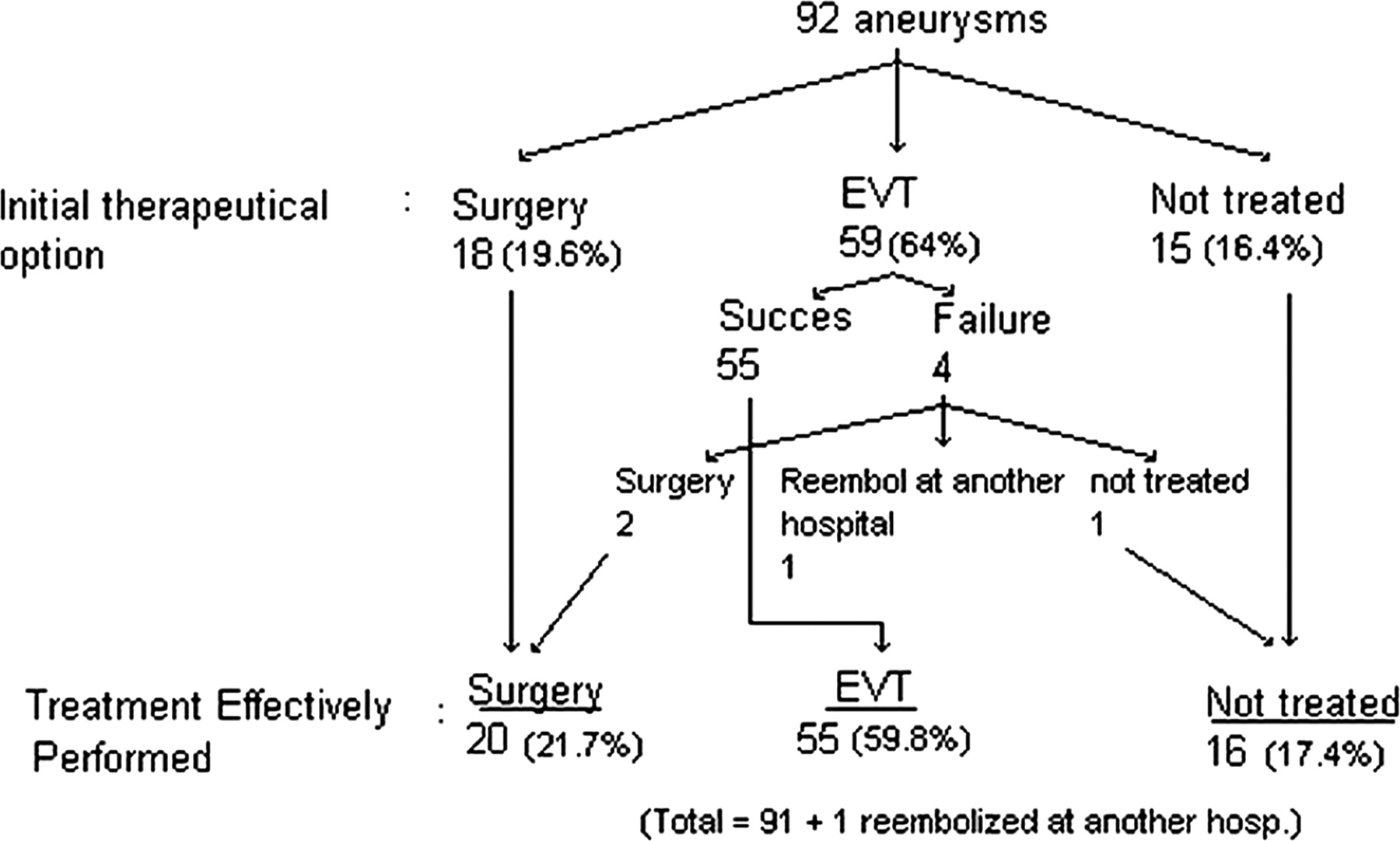
Flow chart of options for treatment of MCAAs.
Patient characteristics, clinical data, and outcome at discharge for patients with middle cerebral artery aneurysms not treated by coiling as first option
Features of the Embolized Aneurysms
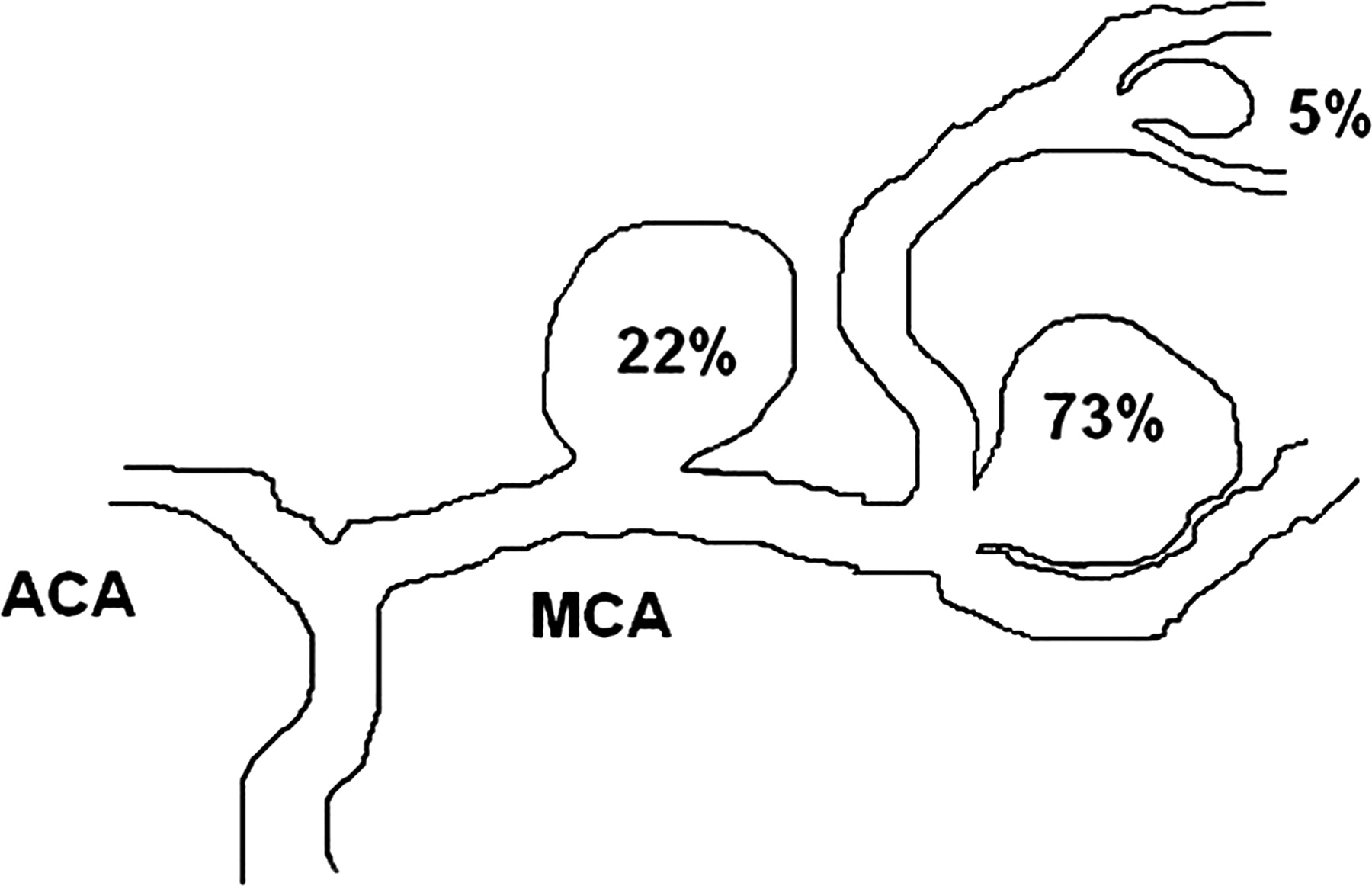
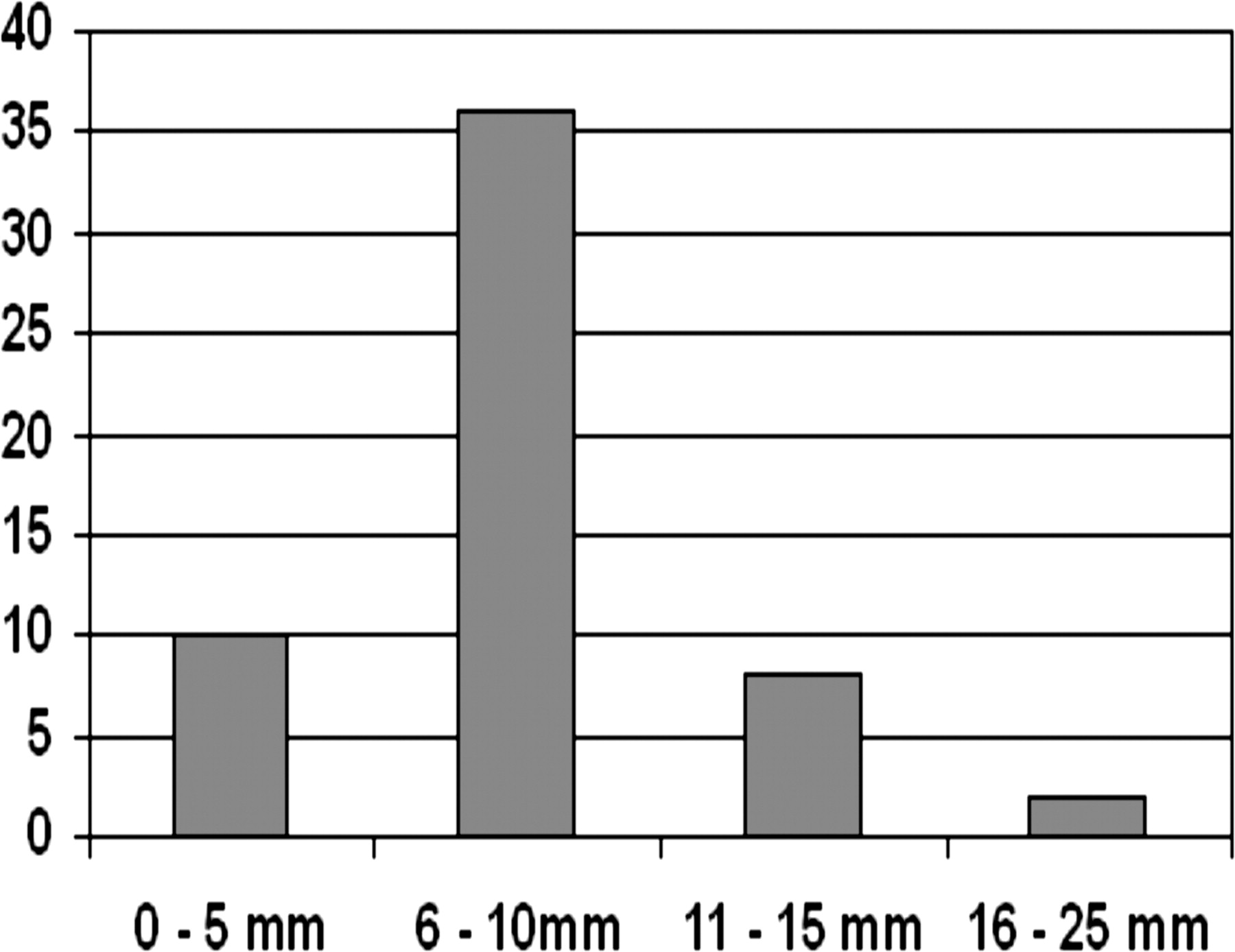
Of the 59 embolized aneurysms, 33 (55.9%) were ruptured, and 26 (44.1%) were unruptured. Thirty four were located in the right hemisphere and 25 in the left hemisphere. Thirteen (22.0%) were located in the main trunk of the artery (M1 segment), 43 (72.9%) at the first major bifurcation, and only 3 (5.1%) beyond that point (Fig 3). Aneurysm diameters ranged from 3 to 20 mm (mean, 6 mm; Fig 4) and aneurysm neck widths from 2 to 5 mm (mean, 2.8 mm). At admission, 21 of the 59 embolized aneurysms were grade 0 on the HHGS (5 of the patients concerned had a ruptured aneurysm in another location), 19 were grade I or II, 12 were grade III or IV, and 3 were grade V.

Distribution of 59 MCAAs initially proposed for EVT. ACA indicates anterior cerebral artery.

Diameter of 59 MCAAs initially proposed for EVT.
Procedure Failures
The embolization procedure failed in 4 patients (7.3%). The failures were due to coil instability inside the sac in 3 cases and technical problem involving the coil in 1 case. The coil instability was because of the anatomic features of the aneurysms, which rendered them unsuitable for embolization but had not been identified preoperatively, even by 3D rotational imaging.
Three of these 4 patients were assigned to surgical clipping, but 1 could not undergo surgery because of his poor neurologic condition and advanced age. The remaining patient was retreated by occlusion of the parent artery in another hospital.
Initial Angiographic Results
Of the 55 of 92 aneurysms that underwent embolization, 23 (41.8%) were completely occluded, 24 (43.6%) still had a residual neck, and 8 (14.6%) exhibited a residual aneurysm.
Complications During the Procedure
During the procedure, complications occurred in 13 patients (25.5%): in 3 (5.9%), complications were ruptures, and in 10 (19.6%), complications were thromboembolism. Only 1 of the 3 patients whose aneurysm ruptured during embolization experienced aggravation of her clinical condition because of the mass effect of a hematoma, which had to be surgically removed. In 8 of 10 patients with thromboembolic complications, a thrombolytic agent was administered. Good results were obtained in 4 cases (ie, no change in clinical condition after embolization). Of the 10 patients with periprocedural embolic complications, 5 had unruptured aneurysms, and just after the procedure, 3 of them exhibited neurologic deficits despite the administration of thrombolytic agents. After the follow-up period, they were grades 1, 2, and 4 on the mRS, respectively. Of the 5 patients with SAH, 1 was grade IV on the HHGS and died after a severe vasospasm. Of the 4 others, only 2 exhibited additional neurologic deficits, but after the follow-up period, they were grade 1 or 2 on the mRS.
Globally, 6 patients (11.8%) were aggravated, and 1 patient (2.0%) died postoperatively related to a preoperative rupture or a thromboembolic complication. The patient who died was initially grade 4 and presented a severe vasospasm. Because he also had a thromboembolic complication, this death was attributed to the treatment.
Globally, in the follow-up period, 4 of 55 patients were aggravated (mRS >2) because of the EVT (1 death and 3 neurologic deteriorations). In 1 case of rupture occurring in a HHGS IV patient, no clinical modification was observed immediately after the treatment, but in the follow-up, mRS was 3. The rerupture probably partially explains the outcome of this patient. Then, the permanent morbidity and mortality of the treatment were 5.9% and 2.0%, respectively. One patient for whom we used a thrombolytic agent exhibited an aneurysm of the femoral artery at the puncture site and was treated by vascular surgery without adverse consequences.
Recanalized Aneurysms
After a mean follow-up of 13.1 months, we identified 8 aneurysms (14.5%) of which the occlusion rate had regressed, but additional coiling was only considered necessary for 3 of them. One of the patients concerned had a completely occluded aneurysm after re-embolization, 1 decided to undergo surgery, and the other has not yet agreed to a treatment.
Final Angiographic Results
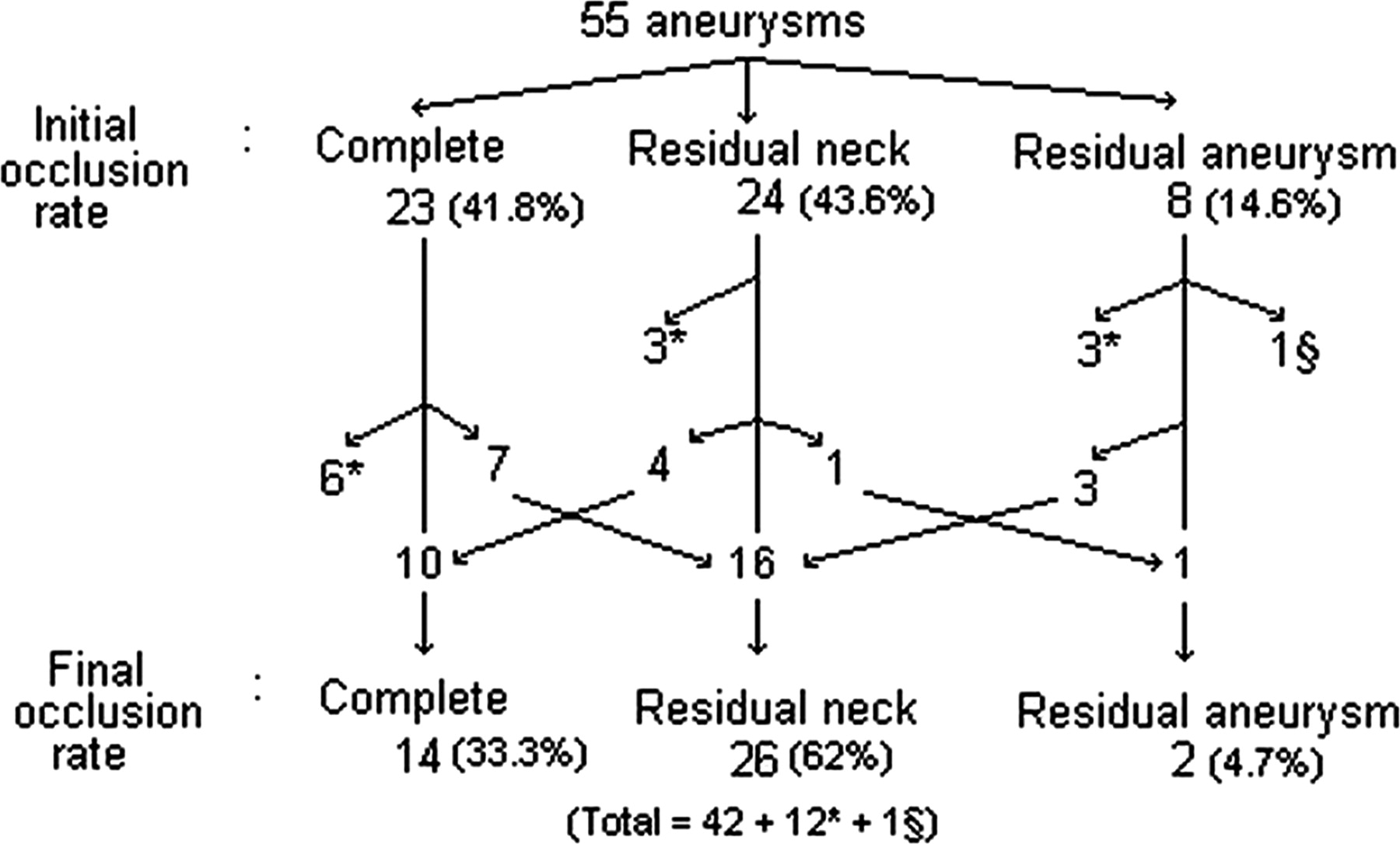
Finally, 55 aneurysms (59.8%) were embolized, 20 (21.7%) were surgically clipped, 16 (17.4%) were not treated, and 1 patient was re-embolized at another hospital. In the embolized group, 7 patients died of complications because of SAH, 5 were lost to follow-up, and 1 patient with residual aneurysm had a complementary treatment by surgery. The angiographic results were as follows: 17 of the 23 aneurysms that were initially completely occluded had midterm anatomic follow-up, 10 remained completely occluded, and 7 retained a residual neck. Of the 24 aneurysms with initially residual necks, 21 had midterm anatomic follow-up: 16 retained a residual neck, 4 evolved to complete occlusion, and 1 became a residual aneurysm. Of the 8 initially residual aneurysms, 4 had midterm anatomic follow-up: 3 evolved into a residual neck and 1 remained with a residual aneurysm (retreatment is programmed). Finally, 14 aneurysms (33.3%) were completely occluded, 26 (61.9%) retained a residual neck, and 2 (4.8%) retained residual aneurysms (Fig 5).

Flow chart of occlusion rates for 55 aneurysms treated by endovascular coiling. * indicates patients who died or were lost to follow-up; §, surgically treated patients.
Final Clinical Grades of the 51 Embolized Patients
In the final clinical grading, 30 patients (58.8%) were grade 0 or 1 on the mRS, 6 (11.2%) were grade 2, 5 (11.8%) were grade 3, 2 (3.9%) were grade 4, 1 (2.0%) was grade 5, and 7 (13.7%) were grade 6. In the group of patients who died, 1 patient was grade V on the HHGS at admission, 4 patients were grade III or IV, and 2 were grade II. There were no episodes of rebleeding during the follow-up period.
Discussion
Ausman7 was the first neurosurgeon to advocate endovascular coiling of cerebral aneurysms as a first option treatment in 1997. In his experience, 50% of aneurysms were suitable for EVT. In the series reported by Raftopoulos et al,4 the proportion of aneurysms proposed for coil embolization was similar, but embolization of the MCAA was responsible for 41.7% of the total failures of this technique of treatment. In 1999, Regli et al2,3 reported 85% of failures for the EVT of unruptured MCAAs. In addition, the authors of a recent series found that, on the basis of 3D imaging, only 16.1% of all MCAAs were suitable for EVT, and they obtained a complete occlusion rate of 86.8%.8 The authors of the above studies attributed their results to the anatomic characteristics of the MCAAs. In the ISAT, EVT was more effective than clipping for all aneurysms, whatever their location, but MCAAs only accounted for 14% of the aneurysms included in the study.1 Advances in coil technology will probably increase the proportion of aneurysms that is treatable by endovascular techniques: for instance, the introduction of coils with complex shapes and 3D structures and ultrasoft coils, as well as the development of techniques using balloons and intravascular stents to support coil occlusion, are improvements that have already broadened the appropriate indications for coil embolization. The skills of the practitioner performing this technique and the facilities available in the institution concerned are also important, because the outcome of endovascular coil embolization improves as practitioners acquire more experience.9 In 2005, the Rothschild Foundation published a series of 149 embolized MCAAs, for which the feasibility rate was 99% and the morbidity-mortality rate was very low.10 However, this series was very specific, because most of the patients were referred from other centers to be treated endovascularly as a first option. The same institution published a series of unruptured MCAAs treated by embolization and observed that only 9% were assigned to surgery after discussions based on 3D images or embolization failure, and only 2.2% of the patients in the series had a neurologic deficit related to the embolization.11 Finally, the feasibility of EVT of MCAAs is difficult to evaluate because of the great heterogeneity of the series dealing with this topic. To have a more precise evaluation of this feasibility, an analysis of our practice was conducted knowing that, in our center, endovascular approach is the first when it is clinically relevant and technically possible.
Appropriate patient selection is of great importance. Careful evaluation of the angioarchitecture by using multiple projections and rotational 3D angiography, available on most new generation neurointerventional angiosuites, may be helpful for precise visualization of the aneurysmal neck, shape, and size, thus favoring appropriate patient selection and further treatment planning by a multidisciplinary team.
In the present study, 59 (77.6%) of the 77 aneurysms treated were initially proposed for EVT, but only 55 (71.5%) actually underwent this treatment. Then, the feasibility of EVT of MCAAs is greater than expected before.2–3,8 However, a precise analysis of complications and anatomic results is needed to define the place of the EVT in the management of MCAAs. Overall, treatment-related adverse events with or without clinical modification were encountered in 13 patients (25.5%). The comparison of treatment-related adverse events from one series to another is difficult, because some totally silent events were not reported, like small clots close to the neck or partial deployment of 1 coil outside the limit of the aneurysms, which were, respectively, described as thromboembolic events and ruptures in our series. However, in the review performed by Brilstra et al9 in 1999, the rate of complications for all of the aneurysm locations was 12% and 15.4% in high-quality studies. In the largest single-center series reporting results of EVT of intracranial aneurysms,12 complications were reported in 17.45% of cases. In a recent multicentric series dealing with EVT of intracranial aneurysms with Matrix coils,13 treatment-related adverse events were reported in 18.2%. In our series, the rate of aneurysm perforation during treatment was 5.9%, and thromboembolic events were observed in 19.6% of cases. These percentages are slightly higher than in other series dealing with all aneurysm locations. In the most recent and largest series, the rate of aneurysm perforation during EVT was 2.4%–4.5%,9 2.3%,14 3.6% including aneurysm perforation and coil malposition or thrombosis,12 and 3.6%.15 The rate of thromboembolic complications was 11%,16 8.5%,9 9.5%,12 and 12.7%.13 The global rate of perioperative rupture and thromboembolism seems high in our series because of the fact that all of the adverse events, even with no clinical modifications, were reported. In most endovascular and surgical series, only clinically relevant complications were reported. In our series, the global rate of clinically relevant complications is 13.7% (perforation, 2.0%; thromboembolism, 11.7%) and compares favorably with most endovascular series dealing with various locations.
In the follow-up, procedure-related permanent morbidity and mortality were, in our series, 5.9% and 2.0%, respectively, and compare favorably with other series dealing with aneurysms in various locations. In the largest series, permanent morbidity was, respectively, 4%,16 4.8%,17 5.1%,12 6%,14 and 8.9%.15 Mortality was, respectively, 1.3%,12 1.4%,15 2%,16 3.4%,14 and 4.8%.17
Despite the good feasibility rate in our series, the angiographic results seem poorer than those reported in the literature9,18,19 for 4 reasons. First, assessment of these results is limited by Raymond classification, which is not easy to apply. For example, the difference between a residual neck and a residual aneurysm may be hard to detect. Second, in our study, the occlusion rate was evaluated by an independent observer. As demonstrated previously, the operator's evaluation and that of an independent observer often differ.13 Third, the relatively high percentage of neck remnants in our series was probably because of the treatment strategy that we used. Thus, to reduce the rate of thromboembolic complications as much as possible, we deliberately left the aneurysmal neck in place in certain cases, when there was a risk of occlusion by protrusion of the coils or a risk of clotting of a branch of the MCAA bifurcation. Lastly, remodeling with balloon was only used in 4 cases (6.7%) in our series. We know from recent publications that this technique will improve the feasibility and occlusion rates without increasing the rate of complications.11,20
An aneurysm may grow or recanalize after initial coil embolization, even when it has been completely occluded.9,18,19 Further embolization is possible and may be required to prevent growth and possible SAH.18,21 Follow-up imaging provides an opportunity to identify inadequately treated aneurysms before SAH or other symptoms occur. An unpredictable number of aneurysms will require additional treatment after initial coil embolization. When a second embolization is not possible, surgery may be indicated.22 Our follow-up protocol of embolized aneurysms include MRA at 3 months and MRA and DSA at 1 year. Subsequent follow-up imaging is based on the results of 1-year imaging, depending on the appearance of the aneurysm. During the follow-up period, only 13 months, we observed a global recurrence rate of 14.5%, but retreatment was only considered necessary in 3 cases of major recurrence, which shows that, for MCAA, the coiling treatment gives lasting results. Moreover, no bleeding or rebleeding was observed during the period of follow-up, even for partial occlusions. We also observed improvement of the occlusion rate for 7 patients. One of the limits of this study regarding anatomical results is the small size of the population and the short period of follow-up.
In this study we did not analyze our surgical results in detail, because the number of patients in this group was too small to draw valid conclusions. Moreover, it was a selected population that was not comparable with an endovascular group. A comparison with the neurosurgical literature is difficult because there have been few reports dealing with the outcome of surgical management of MCAAs, and it is not really logical to compare the results of the EVT of a global series dealing with various locations. Moreover, in series evaluating clinical results after surgical treatment of ruptured intracranial aneurysms, it is not always possible to delineate precisely the morbidity and mortality related to the surgical treatment itself. Then a true comparison between the results of endovascular and surgical treatment of MCA aneurysms is actually difficult. In the report on surgical results by the International Cooperative Study, the mortality rates after surgery for MCAAs (4%–18% depending on the patient's evolution before surgery) were better than those seen after surgery for anterior cerebral/anterior communicating artery aneurysms and aneurysms in the posterior circulation.23 In another series, consisting of 413 patients with MCAA, 94% of good or excellent results were reported 6 months after surgery, but half of these patients underwent surgery after 2 weeks or had unruptured aneurysms and HHGS grades of 0 or I.24 In contrast, in a large series of 561 patients with MCAA, Rinne et al25 reported surprisingly poor management outcomes after 1 year for 32% of ruptured MCA aneurysms compared with 25% for other anterior circulation aneurysms. According to the review presented by Horowitz et al,26 the morbidity and mortality for patients with a HHGS grade of 0 or 1 undergoing surgical clipping of an MCA aneurysm is between 3% and 16% compared with 7.9% in our series. Our series cannot be directly compared with surgical series dealing with unruptured aneurysms, because ruptured and unruptured aneurysms were included. In our series, the overall morbidity was 15.7%, and the overall mortality was 13.7%, which compare well with the rates reported for the surgical series referred to above.
Conclusion
In our nonselected series, EVT of MCAAs is feasible in a high percentage of cases (71.5%) and can favorably change their natural history in midterm (no bleeding or rebleeding in our series). According to our analysis and to the literature, the safety of the EVT of MCAAs seems to be somewhat similar to other aneurysmal locations. On the other hand, our results are difficult to compare with surgical data. Larger series are probably necessary to have a more precise evaluation of the results of the EVT of MCAAs and to precisely analyze the respective indications of surgical and EVT in the management of MCAAs. According to our experience and other aneurysmal locations, multidisciplinary decisions are certainly indicated in the management of MCAAs. Improvements in embolization techniques, materials used, and image technology will certainly greatly increase the feasibility and safety of MCAA embolization in the future, widening its indications.
References
- Received October 26, 2006.
- Accepted after revision February 5, 2007.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Endovascular Treatment of 300 Consecutive Middle Cerebral Artery Aneurysms: Clinical and Radiologic Outcomes
- Stent-Assisted Coiling of Complex Middle Cerebral Artery Aneurysms: Initial and Midterm Results
- Endovascular Treatment of Wide-Neck Middle Cerebral Artery Aneurysms with Stents: A Review of 16 Cases
- Long-Term Follow-Up of 1036 Cerebral Aneurysms Treated by Bare Coils: A Multicentric Cohort Treated between 1998 and 2003