
Abstract
SUMMARY: Cerebral amyloid angiopathy (CAA) is an important cause of intracerebral hemorrhage. Its definite diagnosis still requires histopathologic demonstration of vascular amyloid. Thus, further improvement of noninvasive imaging methods would be desirable. Here we present 3 patients with histologically proved CAA, in which superficial cortical hemosiderosis and subarachnoid hemosiderosis were present in T2*-weighted MR images. Thus, we propose that these 2 findings might be valuable as noninvasive diagnostic markers for CAA.
Cerebral amyloid angiopathy (CAA) is defined as the deposition of amyloid in the walls of cortical and leptomeningeal blood vessels. The most important clinical presentation of CAA is intracerebral hemorrhage (ICH),1,2 but identifying CAA as the cause of ICH is challenging. According to the most widely used Boston diagnostic criteria, the definite diagnosis of CAA and the diagnosis of probable CAA with supporting pathologic findings still require the histopathologic demonstration of vascular amyloid as a criterion standard.3,4 Thus, further improvement of the sensitivity and specificity of noninvasive imaging methods would be desirable to increase the value of noninvasive diagnostic measures.
Here we report on 3 consecutive patients with histologically proved CAA who presented to our hospital between June 2002 and June 2006. On the basis of the imaging findings in these patients, we propose superficial cortical hemosiderosis and subarachnoid hemosiderosis as potentially useful new MR imaging criteria to facilitate the noninvasive diagnosis of CAA. In this context, we defined the term subarachnoid hemosiderosis as hemosiderosis in the subarachnoid space. Superficial cortical hemosiderosis is defined as linear residues of blood in the superficial layers of the cerebral cortex as opposed to the punctate subcortical microhemorrhages often described in CAA.5
Case Reports
Patient 1
A 70-year-old woman initially presented with slowly progressive aphasia and apraxia. MR imaging revealed a left parietal leptomeningeal lesion with signal hyperintensity on proton-attenuation (PD)-weighted images, and a linear leptomeningeal contrast enhancement on contrast-enhanced T1-weighted images. T2*-weighted images were not performed at this time. Analysis of the CSF showed no pathologic findings.
One week later, the patient experienced acute global aphasia and severe apraxia. CT revealed an acute left temporal ICH, adjacent to the leptomeningeal lesion. MR imaging also demonstrated the acute left temporal ICH. In addition, T2*-weighted images depicted superficial cortical hemosiderosis in the left parietal lobe (Fig. 1), and subarachnoid hemosiderosis in the left frontal lobe. CT did not show any evidence of acute subarachnoid hemorrhage in the left parietal lobe, but in the left frontal lobe. Digital subtraction angiograms did not show any arteriovenous malformation, dural arteriovenous shunts, or sinus or venous thrombosis.

Patient 1, a 70-year-old woman with global aphasia and severe apraxia. T2*-weighted image demonstrates superficial cortical hemosiderosis in the left parietal cortex (arrows).
Surgical evacuation of the left temporal ICH including open biopsy of the left parietal meninges was performed. The histopathologic examination revealed beta A4-positive CAA with involvement of the meningeal as well as the cerebral vessels and brain parenchyma.
Patient 2
A 69-year-old man presented at an outpatient clinic with a severe headache, visual disturbances, and nausea lasting 3 weeks. Imaging revealed a left frontal ICH. On admission to our hospital, the patient presented with left-sided hemiplegia. MR imaging revealed an acute ICH in the right anterior temporal lobe and a subacute ICH in the left frontal lobe. In addition, T2*-weighted gradient-echo images demonstrated left frontal subarachnoid hemosiderosis, and left parietal superficial cortical hemosiderosis (distant from the acute macrohemorrhages [Fig 2]). Surgical resection of the right temporal ICH via right temporal trepanation and histopathologic evaluation of the resected material revealed CAA.

Patient 2, a 69-year-old man with severe headache, visual disturbances, and nausea. A,B, T2*-weighted images depict left frontal subarachnoid hemosiderosis (dotted arrows) and left parietal superficial cortical hemosiderosis (arrows).
Patient 3
A 72-year-old woman with a history of breast cancer presented with an acute left-sided, brachiofacial hemiparesis, somnolence (Glasgow Coma Scale of 12), and a gaze deviation to the right side. According to her husband, the patient had experienced a right frontal ICH 3 years previously and had had some deficits in short-term memory since then.
Unenhanced cranial CT demonstrated an acute right frontal ICH. MR imaging revealed a hyperacute, right frontal lobar hemorrhage with signal isointensity on T1-weighted images. In addition to the hyperacute ICH, T2*-weighted gradient-echo images showed subarachnoid hemosiderosis and superficial cortical hemosiderosis in the right frontal and parietal lobe, as well as in the left frontal lobe (Fig 3). As the PD-weighted MR images did not show any hyperintensity in the subarachnoid space in the respective regions, the hypointensity in the T2*-weighted images was not caused by an acute subarachnoid hemorrhage. Instead, it corresponds to chronic subarachnoid hemosiderosis. The right frontal lesion did not show any abnormal contrast enhancement, and contrast-enhanced T1-weighted images did not reveal additional contrast-enhancing intracerebral lesions. Thus, there was no evidence of intracerebral metastasis of the breast cancer. Evacuation of the right frontal ICH via a right parietal trepanation and subsequent histopathologic examination revealed CAA as the underlying cause of the ICH.

Patient 3, a 72-year-old woman with histopathologically proved CAA and a large hyperacute right frontal intracerebral macrohemorrhage (thick arrows). A,B, T2*-weighted images demonstrate the hyperacute lobar hemorrhage (thick arrows), subarachnoid hemosiderosis (dotted lines), and superficial cortical hemosiderosis (thin arrows).
Discussion
Here we present the imaging findings of 3 patients with histologically proved CAA in which we observed superficial cortical hemosiderosis and subarachnoid hemosiderosis on T2*-weighted images.
Secondary acute subarachnoid hemorrhage has been described in CAA in cases in which an ICH reaches the cortical surface.6 It has been speculated that CAA can cause primary subarachnoid hemorrhage as well, but data supporting this hypothesis are still sparse.6,7 We found chronic subarachnoid hemosiderosis at sites distant from the localization of acute ICH in 2 of our 3 patients. These observations indicate that these patients had clinically occult subarachnoid hemorrhages and that subarachnoid hemorrhage in CAA cannot only occur as an epiphenomenon if a lobar ICH reaches the cortical surface,6 but also as a primary hemorrhagic manifestation of CAA. This has also been suggested in cases of familial leptomeningeal amyloidosis.8,9 A neuropathologic study by Takeda et al10 further supports this hypothesis, as it shows that in some cases of CAA the primary hemorrhage occurs in the subarachnoid space.
Besides subarachnoid hemosiderosis, we observed linear superficial cortical hemosiderosis, defined as linear blood residues in the superficial cortical layers of the brain on the T2*-weighted images in our patients. In accordance with our findings, Kumar et al11 identified 1 patient in their study on superficial siderosis of the CNS who had a history of supratentorial intraparenchymal hemorrhages caused by CAA, in whom superficial deposits of hemosiderin were present over the cerebral convexities, but not in the posterior fossa, which is the typical localization of the hemosiderosis observed in superficial siderosis of the central nervous system.12
The superficial cortical hemosiderosis observed in our patients could have been caused by a primary bleeding in the superficial cortical layers, but it has been shown in animal models with experimental siderosis that repeated bleeding in the subarachnoid space leads to deposition of hemosiderin in the subpial layer of the brain.13 Thus, we propose the same mechanism as the underlying pathogenesis of the linear superficial cortical hemosiderosis that we observed in our patients. The schematic drawing in Fig 4 illustrates the development and imaging appearance of subarachnoid hemosiderosis and superficial cortical hemosiderosis.

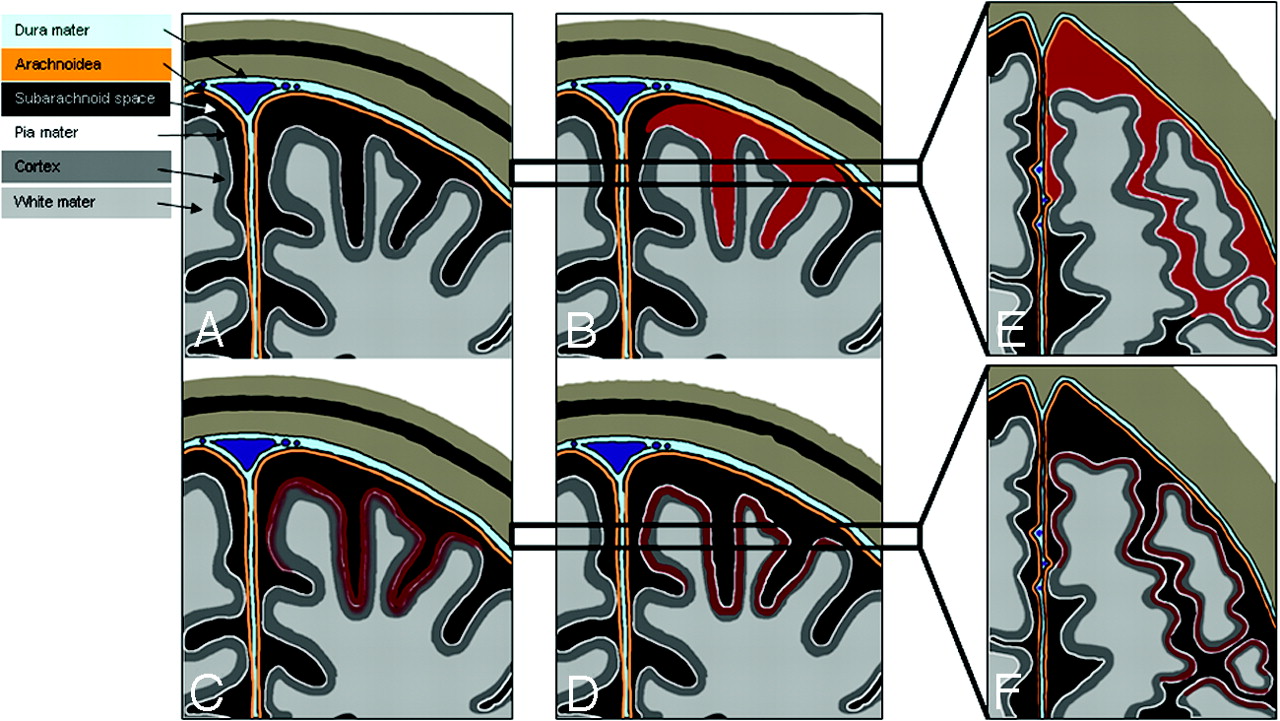
A–F, Schematic drawings illustrating subarachnoid hemosiderosis and superficial cortical hemosiderosis. A–D, Coronal schematic drawings, illustrating the time-dependent development of subarachnoid hemosiderosis and superficial cortical hemosiderosis (black, subarachnoid space; white line, pia mater; orange line, arachnoid layer; light blue, dura mater). E,F, Horizontal schematic drawings corresponding to the areas marked with black bars in B and C, demonstrating the visual appearance of subarachnoid hemosiderosis and superficial cortical hemosiderosis on axial sections. A, Normal appearance of the subarachnoid space. B,E, Subarachnoid hemorrhage (red) presenting as a linear signal intensity in the subarachnoid space (E). C, Residues of blood penetrating the pia mater and deposit in the superficial layers of the cerebral cortex. D,F, Superficial cortical hemosiderosis, defined as linear residues of blood in the superficial layers of the cerebral cortex (dark red). Superficial cortical hemosiderosis typically has a bilinear “tracklike” appearance on axial sections, caused by the signal intensity of the normal-appearing subarachnoid space in the middle, which is bordered bilaterally by linear deposits of hemosiderin in the superficial layers of the adjacent cortex (F).
In patient 1, we observed a leptomeningeal contrast enhancement in a cortical region that was affected by CAA. Although this finding has been described previously in patients with familial amyloidosis,14 its detailed pathologic cause remains unclear.
On the basis of the imaging findings in the patients presented here, we propose superficial cortical hemosiderosis and subarachnoid hemosiderosis as potentially useful MR imaging criteria to facilitate the noninvasive diagnosis of CAA. Prospective studies with a larger number of cases are necessary to systematically assess the value of these MR signs in diagnostic settings.
Acknowledgments
We thank Ms. J. Benson for copyediting the manuscript.
References
- Received April 20, 2007.
- Accepted after revision June 29, 2007.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Cerebral amyloid angiopathy: an underdiagnosed cause of recurrent neurological symptoms
- Spontaneous Intracranial Hypotension: Atypical Radiologic Appearances, Imaging Mimickers, and Clinical Look-Alikes
- Cortical superficial siderosis and bleeding risk in cerebral amyloid angiopathy: A meta-analysis
- Cortical superficial siderosis: A prospective observational cohort study
- Innovative Magnetic Resonance Imaging Markers of Hereditary Cerebral Amyloid Angiopathy at 7 Tesla
- Atrophy patterns in cerebral amyloid angiopathy with and without cortical superficial siderosis
- Acute convexity subarachnoid haemorrhage and cortical superficial siderosis in probable cerebral amyloid angiopathy without lobar haemorrhage
- Prevalence and Natural History of Superficial Siderosis: A Population-Based Study
- Florbetapir imaging in cerebral amyloid angiopathy-related hemorrhages
- Republished: Aneurysmal wall imaging in a case of cortical superficial siderosis and multiple unruptured aneurysms
- Cortical superficial siderosis and first-ever cerebral hemorrhage in cerebral amyloid angiopathy
- Early Magnetic Resonance Imaging and Cognitive Markers of Hereditary Cerebral Amyloid Angiopathy
- Aneurysmal wall imaging in a case of cortical superficial siderosis and multiple unruptured aneurysms
- Cortical superficial siderosis predicts early recurrent lobar hemorrhage
- Cerebral Amyloid Angiopathy as an Etiology for Cortical Superficial Siderosis: An Unproven Hypothesis
- Diagnostic Significance of Cortical Superficial Siderosis for Alzheimer Disease in Patients with Cognitive Impairment
- Cerebral amyloid angiopathy with and without hemorrhage: Evidence for different disease phenotypes
- Cortical superficial siderosis: A marker of vascular amyloid in patients with cognitive impairment
- White Matter Perivascular Spaces Are Related to Cortical Superficial Siderosis in Cerebral Amyloid Angiopathy
- Prevalence of cortical superficial siderosis in a memory clinic population
- Cortical superficial siderosis and intracerebral hemorrhage risk in cerebral amyloid angiopathy
- Prevalence and mechanisms of cortical superficial siderosis in cerebral amyloid angiopathy
- Sporadic cerebral amyloid angiopathy revisited: recent insights into pathophysiology and clinical spectrum
- In vivo amyloid imaging in cortical superficial siderosis
- Prevalence of Superficial Siderosis in Patients with Cerebral Amyloid Angiopathy
- Isolated Acute Nontraumatic Cortical Subarachnoid Hemorrhage
- Prevalence of superficial siderosis in patients with cerebral amyloid angiopathy
- Superficial Siderosis in Cerebral Amyloid Angiopathy
- Neuroimaging in Superficial Siderosis: An In-Depth Look
- Descriptive Analysis of the Boston Criteria Applied to a Dutch-Type Cerebral Amyloid Angiopathy Population
- Superficial siderosis in the general population