
Abstract
BACKGROUND AND PURPOSE: Collections of extraluminal paratracheal gas may be present on CT images of the neck and cervical spine and the radiologist may question whether this is related to a pathologic process. This study is designed to demonstrate the appearance, clinical presentation, and prevalence of paratracheal air cysts, which, on CT examinations of the neck, can mimic abnormal extraluminal air.
MATERIALS AND METHODS: From January 1, 2005, through May 22, 2005, a total of 702 CT examinations of the cervical spine or soft tissue of the neck were reviewed. All examinations were at 2- to 5-mm thickness. Sagittal and coronal reconstructions were available for review, if necessary. Paratracheal air cysts were evaluated for size; the presence of visible communication with the trachea; association with pneumothorax, pneumomediastinum, or subcutaneous emphysema; and association with findings of emphysematous changes in the lung apices. Patient demographics of age, sex, and whether the patient had sustained a traumatic injury were also collected.
RESULTS: Of the 702 patients evaluated, 26 (3.7%) had paratracheal air cysts, all of which were found on the right, at the level of the thoracic inlet. Ages of the patients ranged from 15 to 74 years. In 9 (34.6%) of the patients, a direct communication with the trachea was seen. Sizes of the paratracheal air cysts ranged from 1 × 2 mm to 10 × 15 mm. No association was found with CT findings of emphysema in the lung apices, abnormal soft tissue air, or trauma.
CONCLUSION: Right paratracheal air cysts are a common CT finding that occur in a predictable location. In the setting of trauma, these characteristic structures can mimic pneumomediastinum and are seen in approximately 3% to 4% of the US population. The cause is unclear but may be either congenital or an acquired phenomenon, given that they are often seen in both children and adults. We found no association with either trauma or the presence of emphysematous changes in the lung apices.
A frequently occurring finding on CT examination of the neck is an air cyst or collection of air cysts to the right of the trachea at the level of the thoracic inlet (Fig 1). Paratracheal air cysts have been infrequently described in the radiologic literature. Previous reports suggested an association with obstructive lung disease and emphysema from weaknesses in the right posterior lateral wall of the trachea at the level of the thoracic inlet because of increased expiratory pressures in these patients.1 However, several case reports have described congenital right-sided tracheal diverticula in children with recurrent respiratory tract infections or with other congenital respiratory tract abnormalities such as bronchomalacia of the right upper lobe bronchus2 or with cystic adenomatoid malformation.3 It has also been reported that tracheal diverticula can be a rare cause of chronic cough.4,5 Other complications that have been reported include right-sided recurrent laryngeal nerve paralysis6 and difficult intubation.7

Right-sided paratracheal air cyst (arrow) at the thoracic inlet. T indicates trachea; E, esophagus; cc, common carotid; SCA, subclavian artery; IJ, internal jugular vein; Thy, inferior portion of the right lobe of the thyroid gland.
Right-sided paratrachial air cysts at the thoracic inlet can be confused with other causes of extraluminal air collections in the same area such as in patients with apical hernia of the lung, which has been previously described.8 In the patient who has sustained traumatic injuries, right-sided paratracheal air cysts could misinterpreted as mediastinal air, which can also occupy the same location.
The purpose of our study was to determine the prevalence and other demographic associations of right-sided paratracheal air cysts in the general population by evaluating for the presence of this entity on CT examinations of the neck in patients with traumatic injuries and in patients undergoing a study for other indications. We also sought to determine if there is increased prevalence in the trauma population, which might indicate that the entity is related to increased tracheal pressures sustained during traumatic injury. In addition, because this entity has previously been reported to be related to, and possibly caused by, obstructive lung disease, we sought to corroborate this finding by evaluating our studies for evidence of emphysema in the lung apices.
Materials and Methods
From January 1, 2005, through May 22, 2005, a total of 702 consecutive patients had technically adequate CT examinations of the cervical spine or soft tissue of the neck at 2- to 5-mm intervals. These examinations were performed at the University of Arizona Health Sciences Center in Tucson, Arizona, and were reviewed. Additional or follow-up examinations were excluded. Indications for the examinations were for either emergent reasons such as a traumatic injury, with instructions from the emergency department, or for nonemergent reasons such as soft tissue neck studies. Indications for examination of a traumatic injury included pain, blunt trauma, flexion or extension injuries, or penetrating injuries. Sagittal and coronal CT reconstructions were available for review, if necessary. Paratracheal air cysts were evaluated for size; the presence of visible communication with the trachea; association with pneumothorax, pneumomediastinum, or subcutaneous emphysema; and association with findings of emphysematous changes in the lung apices. Patient demographics of age, sex, and whether the patient had sustained a traumatic incident were also collected.
We differentiated paratracheal air cysts from those conditions mimicking air cysts on the basis of several factors: a typical location in the right posterior paratracheal region at the thoracic inlet but located away from the lung pleura, communication with the trachea, and rounded margins that differentiate cysts from emphysematous changes with angular margins as they track along fascial planes.
Results
A total of 26 (3.7%) examinations demonstrated the presence of paratracheal air cysts that ranged in size from 1 × 2 mm to 10 × 15 mm. Ages of patients who had paratracheal air cysts were 15 to 74 years (average age, 34.6 years). Of these patients, 14 (53.9%) were male and 12 (46.1%) were female. Many of the larger air cysts were multiloculated (Fig. 2), and some cysts demonstrated multiple communicating necks with the trachea. Overall, 9 (34.6%) patients had 1 or more communications with the trachea (Fig 3). In the patients who had sustained a traumatic injury, 17 (65.4%) air cysts were found, and 9 were found in patients examined for nontraumatic indications. There were 2 (7.7%) patients who also had pneumothorax, but only 1 (3.9%), of these patients had subcutaneous emphysema (Fig 4). None of these patients had pneumomediastinum extending into the neck, and none had evidence of emphysematous changes in the lung apices.

An 18-year-old woman with typical multiloculated paratracheal air cyst seen in the axial plane (image A superior to B) and in the coronal (C) and sagittal (D) planes. Cyst is labeled with white arrows.
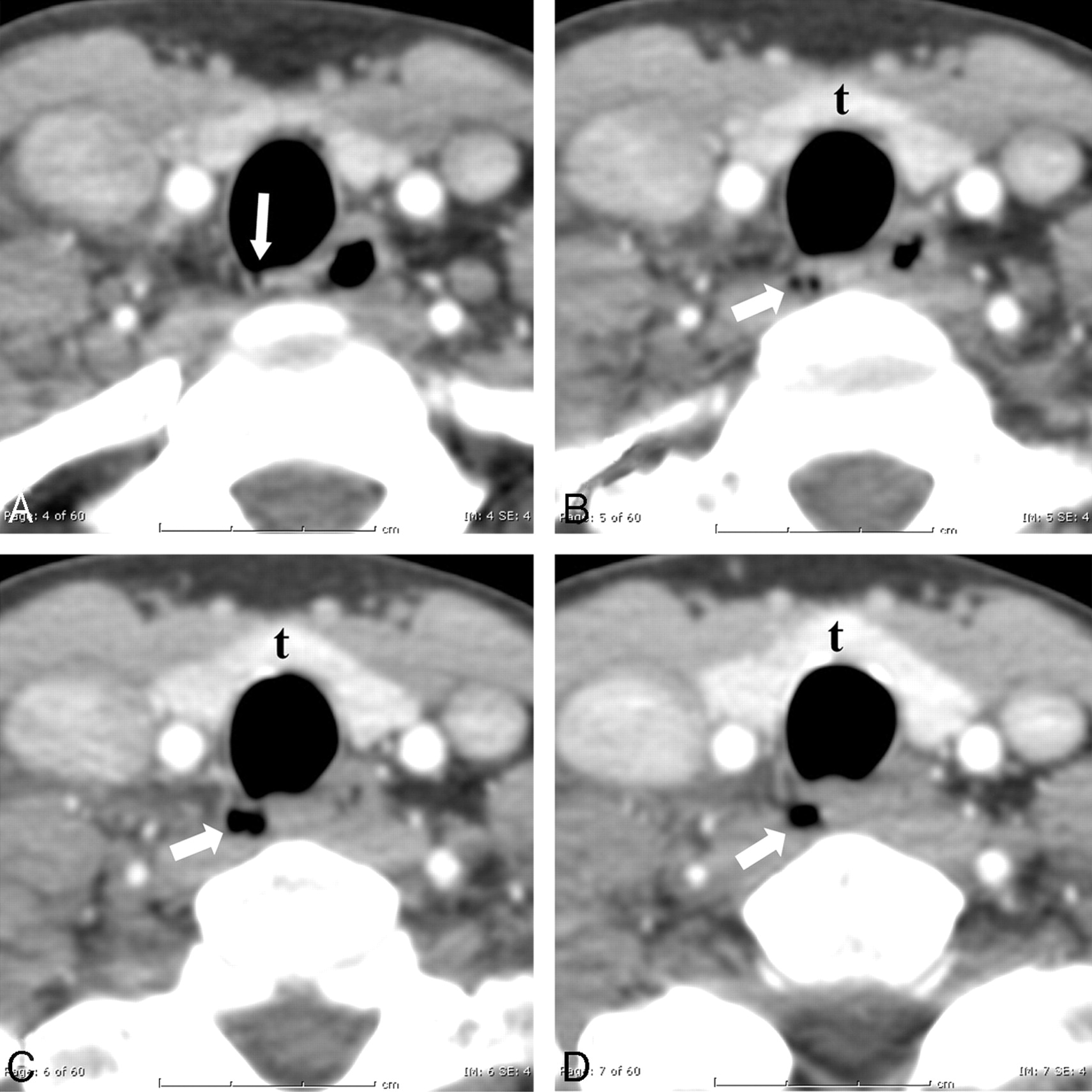
Sequential images through a right-sided paratracheal air cyst. Communication with the trachea via a narrow stalk (arrow) is seen on image A. The air cyst, which is at the level of the thyroid (t) gland, extends inferiorly.

A 63-year-old man involved in an automobile accident. There is a small right-sided paratracheal air cyst (arrow) in the typical location as well as abnormal soft tissue air in the right supraclavicular region (curved arrows). The paratracheal air cyst can be differentiated from the abnormal soft tissue gas in that it communicates with the trachea and is within the wall of the trachea and not adjacent to it.
Of the 702 patients, 429 (61.1%) were male and 273 (38.9%) were female. Of the 542 (77.2%) patients who had sustained a traumatic injury, 25 (3.6%) had pneumothorax, 18 (2.6%) had either subcutaneous emphysema or pneumomediastinum extending into the neck, and 8 (1.1%) had both pneumothorax and soft tissue air. No patients were found to have CT evidence of emphysematous changes in the lung apices. The age range in the population was younger than 1 year to 103 years (average age, 39.6 years).
There were 676 patients without paratracheal air cysts. Of these, 415 (61.4%) were male and 261 (38.6%) were female. A total of 525 (77.7%) patients sustained a traumatic injury; of these, 23 (3.4%) had pneumothorax, 17 (2.5%) had either subcutaneous emphysema or pneumomediastinum extending into the neck, and 7 (1.0%) had both pneumothorax and soft tissue air. The age range in this population was younger than 1 year to 103 years (average age, 39.7 years).
Discussion
In this study, a right-sided paratracheal air cyst in the region of the thoracic outlet is relatively common, being present in approximately 3.7% of the population. Because of its predictable location and appearance, it should not be confused with pneumomediastinum or other causes of cystic lesions in the same region such as apical lung herniation on the right.
Right-sided paratracheal air cysts may be unilocular or multilocular and often can be seen to have communication with the trachea. In fact, some of these cysts have multiple narrow connections with the trachea. In our study, we found a communication with the trachea 35% of the time compared with the previously reported finding of a connection in 8%,1 probably because of the increased resolution in CT scanning that has occurred since the previous study. We believe that at least most, if not all, of these lesions are, in fact, tracheal diverticula. This conjecture is supported by a pathology series published, which demonstrated that these lesions were diverticula protruding through a weakened wall of the trachea in a characteristic location.9 It is interesting to note that although many of the patients with traumatic injuries were intubated, none of these lesions were seen in that population. This finding suggests that when there is compression of a cyst by an endotracheal balloon, the gas may be forced out of the cyst.
There does not seem to be an association between trauma and the prevalence of right-sided paratracheal air cysts. Of the total studied population, 77% were patients with traumatic injuries, but of the patients with right-sided paratracheal air cysts, only 64% had sustained traumatic injuries. There was also no association with the finding of soft tissue air or pneumothorax, as 5% of the total population had either 1 or the other, or both, compared with 8% who had a cyst. The difference was not statistically significant. Before our study, we had theorized that increased intratracheal pressures developed during trauma could lead to the development of tracheal diverticula. This does not seem to be the case.
Goo et al1 concluded in their study published in 1999 that there is an association between paratracheal air cysts and obstructive lung disease. We did not find any relationship in our study. None of the patients in our study had findings of emphysema in the lung apices. In addition, the average age of the patients with cysts was 37 years, which suggests that air cysts are unrelated to chronic obstructive pulmonary disease. Additionally given that five of the lesions were found in teenagers, this would also support that these could be congenital or developmental lesions rather than acquired through a disease process such as obstructive lung disease.
We observed a prevalence of air cysts of 3.7%, whereas Goo et al1 reported a prevalence of 2%. They also reported a size range of 5 to 20 mm compared with a range of 2 to 15 mm in our study. The differences are likely because of the increased ability to detect smaller cysts with the advent of thinner cuts and higher spatial resolution.
In summary, right-sided paratracheal air cysts at the level of the thoracic inlet are common and should not be confused with pneumomediastinum on CT of the cervical spine in the patient who has sustained a traumatic injury.
References
- Received October 16, 2007.
- Accepted after revision January 27, 2008.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}