
Abstract
SUMMARY: We present a case with recurrent orbital myositis sequentially affecting both lateral rectus muscles separately. In the first episode, the absence of the required symptoms for the diagnosis of orbital myositis led to the erroneous diagnosis of sixth nerve palsy. Eventually, the correct diagnosis was established with cerebral MR imaging. Orbital myositis should be included in the differential diagnosis of what appears clinically to be abducens palsy, and MR imaging with a focus on the orbita is mandatory in such patients.
Orbital myositis implies orbital inflammation confined to ≥1 extraocular muscle and usually begins acutely with unilateral periorbital pain, particularly with eye movement, and diplopia due to restriction of extraocular muscle movement. In addition, eyelid swelling and conjunctival injection usually are present.1 These may be related to specific inflammatory processes associated with systemic disease or restricted to the orbit.2 Typically, inflammation is unilateral and can be recurrent. Recurrences can involve different muscles and, occasionally, the other eye.2 Diagnosis can usually be made clinically due to the characteristic pain and signs of inflammation. Here, we report a young patient with 2 asynchronous bilateral orbital myositis episodes, separated by 18 months, presenting without any clinical signs of inflammation. This case emphasizes the notion that orbital myositis should be considered in the differential diagnosis of clinically apparent abducens nerve palsy.
Case Reports
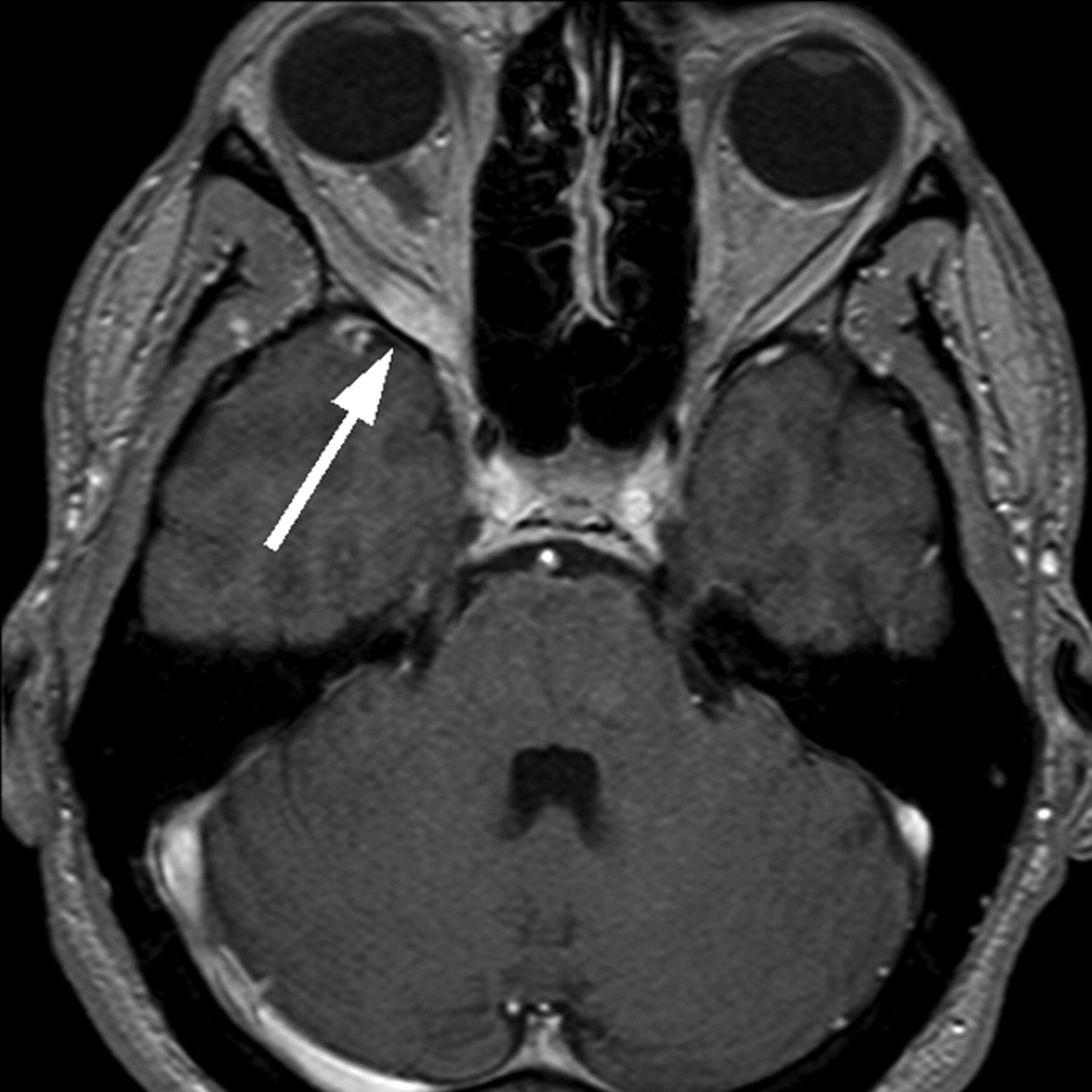
A 30-year-old man presented after acute onset of diplopia on gazing to the right. He reported pain around the right eye for 3 days, especially when looking to the right. Neurologic examination revealed a discrete deficit in abduction movement of the right eye that progressed during the following days. There was no conjunctival injection, chemosis, or bulb pain present; and visual acuity, visual fields, pupillary reactions, funduscopy findings, and eyelids were normal as were the findings on the remainder of the neurologic examination. Results of thyroid function tests were normal. MR imaging of the brain showed swelling and signal-intensity hyperintensity in the right lateral rectus muscle on T2-weighted images (Fig 1) and contrast-enhancement on T1-weighted images (Fig 2), establishing the diagnosis of myositis. Symptomatic causes were excluded; steroid treatment with intravenous prednisolone, followed by oral prednisolone in a decreasing dosage, led to complete remission.

Cerebral MR image shows swelling of the right lateral rectus muscle (arrow) on a T2-weighted image. Note the position of the bulbi indicating right-sided weakness for abduction.

Cerebral MR image shows swelling of the right lateral rectus muscle (arrow) on a T1-weighted image with contrast enhancement. Note the position of the bulbi, indicating right-sided weakness for abduction.
During the stay, he reported having had similar symptoms at the contralateral (left) eye 18 months previously, with diplopia on looking to the left. According to the patient and the medical records, pain and other signs of inflammation had been absent. At that time, abducens nerve palsy had been diagnosed. Brain MR imaging and intracranial MR angiography, CSF, visual-evoked potentials, and acoustic-evoked potentials had been unremarkable on first impression. Reassessment of the MR imaging scans revealed signal-intensity hyperintensity and slight thickening of the left lateral rectus muscle on T2-weighted images (Fig 3), which had not been noticed 18 months earlier. Therefore, the diagnosis of recurrent ocular myositis was established. There had been no family history of orbital myositis.

Eighteen months previously, similar swelling was present in the left lateral rectus muscle (arrow) on a T2-weighted image. Note the position of the bulbi, indicating left-sided weakness for abduction.
Discussion
In patients 50 years of age or older, sixth nerve palsy is usually attributed to extra-axial microvascular injury associated with arteriosclerosis, hypertension, or diabetes.3 In younger patients, nerve compression by aneurysms or tumors, multiple sclerosis, and vascular brain stem lesions must be considered, yet in many cases, the cause remains elusive.4,5
Typically, orbital myositis can be differentiated from neurogenic lesions because of the characteristic clinical triad of periorbital pain, diplopia, and signs of inflammation, such as conjunctival injections or swelling. Concurrent pain is present in >95% of all cases.2,6 Nevertheless, the diagnosis in the painless cases could be established due to other signs of inflammation. Unilateral single-muscle involvement is the most common presentation; multiple or bilateral involvement can also be seen. Superior, lateral, and medial rectus muscles are involved equally frequently, and recurrences occur in ≤56% of cases.7 Multiple muscle involvement, male sex, eyelid retraction, lack of protoptosis, and lack of response to systemic corticosteroids are associated with recurrent orbital myositis.8 Thyroid function must be assessed in recurrent orbital myositis, and a familial incidence is possible. Myositis can be detected on MR images or CT scans through thickening of the affected muscle and uptake of contrast medium, and on MR imaging through signal-intensity hyperintensity in T2-weighted images. Localized inflammation can be evaluated best on fat-suppressed T2-weighted images.9 There is usually a rapid response to systemic steroid therapy. To our knowledge, isolated orbital myositis of the lateral rectus muscle mimicking abducens nerve palsy has not been reported, and recurrence of the condition affecting the contralateral eye in a second episode is unprecedented in the literature.
In approximately 5% of orbital myositis cases, pain is absent, and our case shows that other clinical signs of inflammation can also be missing. Isolated alterations in an individual rectus muscle can occur. This leads to our speculation that some patients presenting clinically with abducens palsy may in fact have inflammation of the lateral rectus muscle, which may be overlooked unless specifically assessed. Although cerebral MR imaging or CT is mandatory in the diagnostic work-up of abducens palsy in younger patients,4 our case illustrates that thickening of the lateral rectus muscle may be missed when the focus is centered on other structures. Orbital myositis should be considered in the differential diagnosis of abducens palsy, especially in younger individuals. MR images with thin sections through the orbits should be included, and special attention should be paid to the lateral rectus muscle of the affected eye. Therapy with steroids leads characteristically to a good and rapid response.7
References
- Received April 5, 2009.
- Accepted after revision May 17, 2009.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.