
Abstract
BACKGROUND AND PURPOSE: Diagnostic performance by MR imaging or by SPECT alone in discriminating DLB patients from AD patients has been estimated previously. However, the performance of a combination of MR imaging and SPECT has not yet been evaluated. Our aim was to evaluate the usefulness of combining MR imaging and SPECT to discriminate mild DLB from AD.
MATERIALS AND METHODS: Nineteen patients with mild DLB and 19 age- and cognitive decline−matched patients with mild AD underwent both SPECT and MR imaging. Hippocampal, occipital, and striatal volume and SPECT count ratios were compared. Linear discriminant and ROC analyses were performed by using the parameters of striatal volume and the occipital SPECT ratio.
RESULTS: The striatal volume ratio in the DLB group was significantly lower than that in the AD group. The occipital SPECT ratio in the DLB group was lower than that in the AD group. The mean area under the ROC curve from combined MR imaging and SPECT (AUC = 0.898) was higher than that from MR imaging (AUC = 0.679) or SPECT (AUC = 0.798) alone.
CONCLUSIONS: By combining MR imaging and SPECT, we were able to distinguish patients with mild DLB from those with AD with a high level of accuracy. Our findings suggest that combining MR imaging and SPECT modalities is a useful and practical approach for diagnostically differentiating DLB from AD.
Abbreviations
- AD
- Alzheimer disease
- AUC
- area under the curve
- AVSIS
- automated volumetry of segmented image system
- DLB
- dementia with Lewy bodies
- 123I-FP-CIT
- iodine 123-N-omega-fluoropropyl-2β-carbomethoxy-3 β-(4-iodophenyl)-nortropane
- GM
- gray matter
- 123I
- iodine 123
- MMSE
- Mini-Mental State Examination
- PD
- Parkinson disease
- PET
- positron-emission tomography
- ROC
- receiver operating characteristic
- SBD
- Simulated Brain Data Base
- SPECT
- single-photon emission CT
- SPM
- statistical parametric mapping
- TIV
- total intracranial volume
- VOI
- volume of interest
- WM
- white matter
The number of patients diagnosed with neurodegenerative dementia has increased in societies in which the average age of the population has risen. DLB is the second most prevalent form of neurodegenerative dementia following AD, and its clinical diagnosis is based on revised consensus criteria.1 An essential neuropathologic feature of DLB is the presence of Lewy bodies in cortical and brain stem structures, such as the substantia nigra and locus coeruleus.2–5 The central diagnostic criterion for DLB is dementia, defined as a progressive cognitive decline of sufficient magnitude to interfere with normal social or occupational functions. The core diagnostic features of DLB are the following: 1) fluctuating cognition with pronounced variations in attention and alertness, 2) recurrent visual hallucinations that are typically well-formed and detailed, and 3) spontaneous features of parkinsonism. The presence of 2 of 3 core features is sufficient for a diagnosis of probable DLB.1
Clinically distinguishing patients with DLB from those with AD, however, is difficult because of overlapping clinical and pathologic features.3–5 This is especially so during the early stages of illness. For example, because psychosis is usually defined as delusions and/or hallucinations, accurate differentiation of psychosis may be difficult at early stages of both diseases.6,7 The accurate identification and differentiation of patients with DLB and AD are particularly important because of the development of interventions and specific pharmacologic treatments and outcome evaluations.
Occipital abnormalities in glucose metabolism and cerebral perfusion are also a characteristic neuropathologic feature of DLB. This has been demonstrated by using SPECT and PET.8–10 Recent studies have reported dopamine transporter loss in the striatal, caudate, and posterior putamen in patients with DLB.11,12
Many studies investigating AD have found volume decreases in medial temporal structures and cerebral blood flow reductions in temporoparietal areas.13 Few studies, however, have reported the usefulness of cerebral regional volume measurement with MR imaging for discriminating AD from DLB.14
The aim of the present study was to discriminate DLB and AD by means of regional cerebral volume and perfusion measures by combining MR imaging and SPECT techniques.
Materials and Methods
Nineteen patients with mild DLB (8 men and 11 women) and 19 patients with mild AD (8 men and 11 women), matched for age, sex, and MMSE score, were retrospectively selected from patients admitted to the infirmary of our institution for the evaluation of dementia from April 2004 to March 2006. The institutional ethics board approved the study. The requirement for a participant's informed consent was waived due to the retrospective nature of the study and because it was solely observational.
All patients underwent a neurologic and psychiatric examination by 2 neurologists and/or psychiatrists followed by an MR imaging brain scan and a standard neuropsychological examination. Because all the subjects were initial patients, none of them were given any drugs at the examinations. The criteria for diagnosing and managing DLB were revised in 2005.1 This study dealt directly with morphologic and functional findings of DLB. To avoid sample-selection bias, we used DLB inclusion criteria based on the diagnostic criteria from 1996.15 These criteria do not refer to MR imaging and SPECT techniques, while the new criteria include morphologic and functional examinations.
The DLB inclusion criteria used in this study were the following: 1) a diagnosis of probable DLB by using the criteria of the Consortium on DLB International Workshop published in 199616, 2) absence of evidence of focal brain lesions on MR images, and 3) an MMSE score of >20. These criteria include 3 core features (fluctuating cognitive functions, recurrent visual hallucinations, and spontaneous parkinsonism), any 2 of which are necessary for a diagnosis of probable DLB. All patients were examined comprehensively by both neurologists and psychiatrists; and standard neuropsychological examinations, routine laboratory tests, electroencephalography, and cranial MR imaging examinations were performed. Staff physicians closely monitored fluctuation of cognitive functions over a 1-month admission in terms of MMSE performance, activities of daily living, and episodic confusion. Psychiatric and behavioral symptoms were assessed with a structured interview of a caregiver and the Neuropsychiatric Inventory,17 and they were monitored during the patient's hospital stay by staff physicians. Parkinsonism was rated as positive when ≥1 of the following features were present: resting tremor, cogwheel or lead-pipe rigidity detectable without reinforcement, bradykinesia, and loss of postural reflexes.
The inclusion criteria for AD were the following: 1) a diagnosis of probable AD by using the National Institute of Neurologic and Communicative Disorders and Stroke/Alzheimer Disease and Related Disorders Association criteria,16 2) absence of evidence of focal brain lesions on MR images, and 3) an MMSE score of >20. We excluded patients with complications from other neurologic diseases or those in poor overall physical condition and patients with severe language, attentional, or behavioral disorders that might cause difficulties with the MR imaging and SPECT procedures. Subjects in each group were matched for age and sex on a one-to-one basis. Patients with DLB and AD were also matched for MMSE score. None of the patients with AD reported visual hallucinations, fluctuating cognition, or parkinsonism.
The mean ages of the DLB and AD groups were 76.0 ± 7.1 years and 75.6 ± 6.0 years, respectively, and the mean MMSE scores of the DLB and AD groups were 22.7 ± 2.0 and 22.4 ± 1.6, respectively. Thirteen of the 19 patients with DLB had parkinsonism, 16 had visual hallucinations, and 17 had fluctuating cognitive functions.
The MR imaging scanner was a 1.5T Horizon (GE Healthcare, Milwaukee, Wisconsin). For T1-weighted images; 3D spoiled gradient-echo imaging (TR, 14 ms; TE, 3 ms; flip angle, 20°; thickness, 1.5 mm; 124 sections) was performed. Axial T2-weighted images and fluid-attenuated inversion recovery images were also obtained. MR images were obtained 0–28 days before the SPECT examinations.
The SPECT scanning was initiated with the patient in a resting state in a supine position with the eyes closed, 15 minutes after the injection of 111 MBq (3 mCi) of iodine 123 N-isopropyl-p iodoamphetamine. All SPECT studies were performed by using a rotating dual-headed gamma camera (GAMMA View SPECT 2000 H; Hitachi, Tokyo, Japan) with a low-energy general-purpose collimator. The effective FOV was a 220 mm (axial) by 170 mm (longitudinal) volume for imaging of the whole brain, including the cerebellum. The energy window was 160 keV with 20% width. Projection data were obtained at 15 seconds/step × 64 views (2 rotations, 360°). A Ramachandran filter was used for SPECT image reconstruction. Attenuation correction was performed by using Chang's method. Reconstructed images were 4 mm in pixel size and 8 mm in section thickness with 15–17 sections, and reconstructed spatial resolution was 13.4 mm at the center and 8.9-mm tangential at 80 mm. The delay time between performance of the MR imaging and the SPECT studies was 0–2 weeks.
All MR images and SPECT data were transferred to a personal computer. Volumetry and the measurement of SPECT accumulation were performed with our AVSIS.14 In brief, the AVSIS process in this study was the following: VOI intracranial, hippocampal, striatal, and occipital lobe templates were prepared before this analysis. We produced each regional VOI template on a digital phantom (SBD; http://www.bic.mni.mcgill.ca/brainweb) in standard Montreal Neurologic Institute space, delineating the contours of each structure manually. The occipital lobe VOI template included Brodmann Areas 17, 18, and 19.
The process of modified AVSIS was as follows: first, each individual MR image and SPECT image were coregistered. Each subject's MR image was then segmented into GM, WM, and CSF with the SPM5 segmentation program (Wellcome Trust Centre for Neuroimaging, London, UK). The GM template image derived from the SBD was then spatially transformed into the individual subject's GM image, and a normalization parameter was produced. This normalization parameter functions in the same way as a reversed parameter produced in the anatomic normalization of an individual brain to a standard brain. Using this parameter, we transformed the intracranial, hippocampal, striatal, and occipital VOI templates to the individual subject's space. The TIV was adjusted by using an image derived from the segmented GM, WM, and CSF images.
The segmented images were derived as follows: WM and GM areas were calculated with the voxels in the TIV VOI template. GM volumes in the hippocampi and striata were calculated by using the transformed hippocampal and striatal VOI templates. Volumes of GM and WM in the occipital lobes were calculated by using the transformed occipital VOI template for each subject. Each regional relative volume was calculated by normalization relative to the TIV. Next, hippocampal, striatal, and occipital SPECT uptake counts were calculated by determining the regions of coregistered SPECT images on each extracted area by using the aforementioned volumetric procedure (Fig 1). We calculated the regional ratio of DLB and AD: Hippocampal, striatal, and occipital volume/intracranial volumes were used for MR imaging. For SPECT, hippocampal and occipital counts/striatal counts were used.
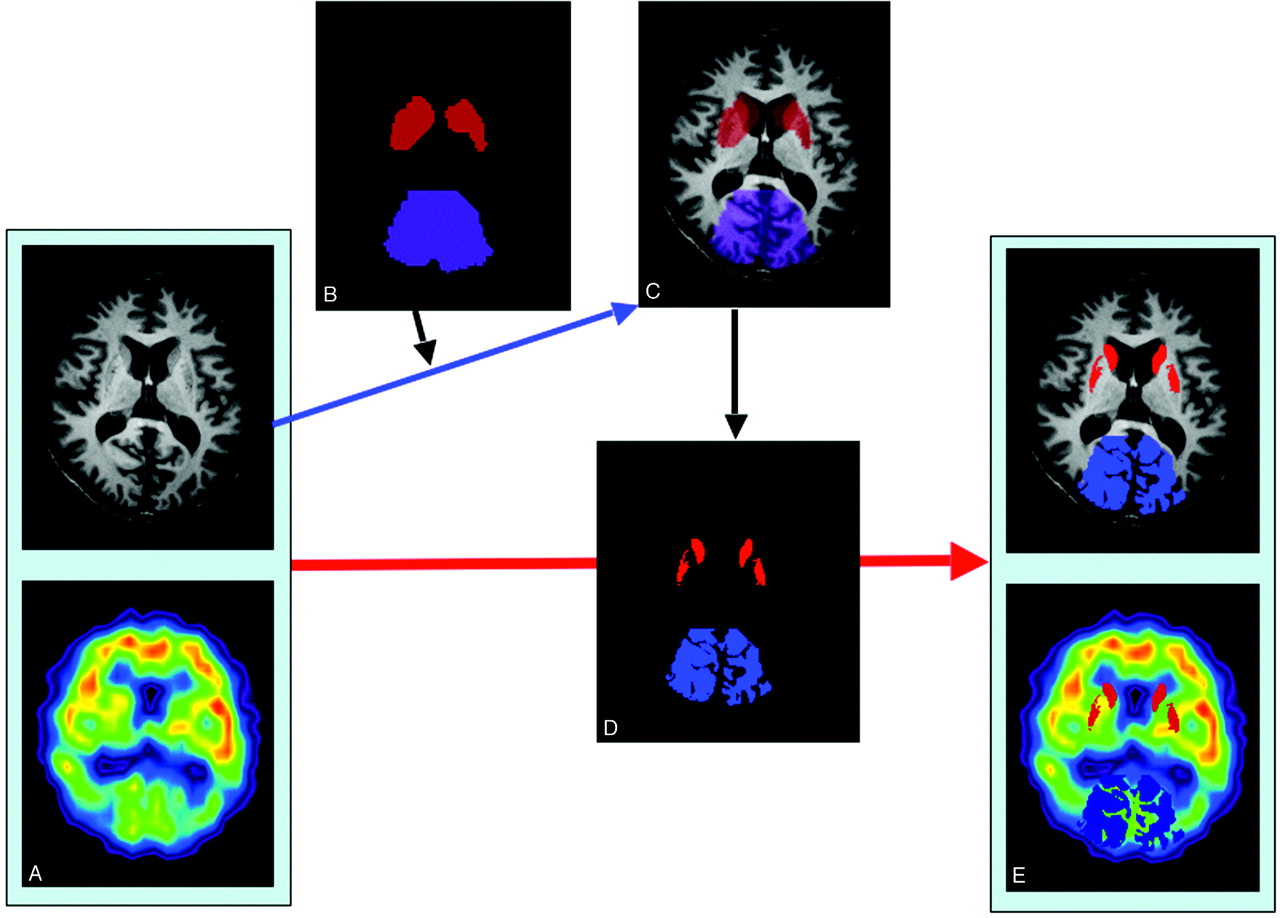
Schema for calculating regional structural volume and SPECT counts. An example of calculating striatal and occipital volume and SPECT counts is shown. A, The original MR imaging and SPECT images are coregistered. B−D, We transformed the striatal and occipital VOI templates to the individual brain (B); and by using these VOI templates on the individual MR image (C), we extracted individual regional segmented VOI templates (D) and calculated their volumes. E, Then, by using the extracted striatum and occipital lobe as VOIs for the individual coregistered SPECT image, we determined striatal and occipital lobe counts.
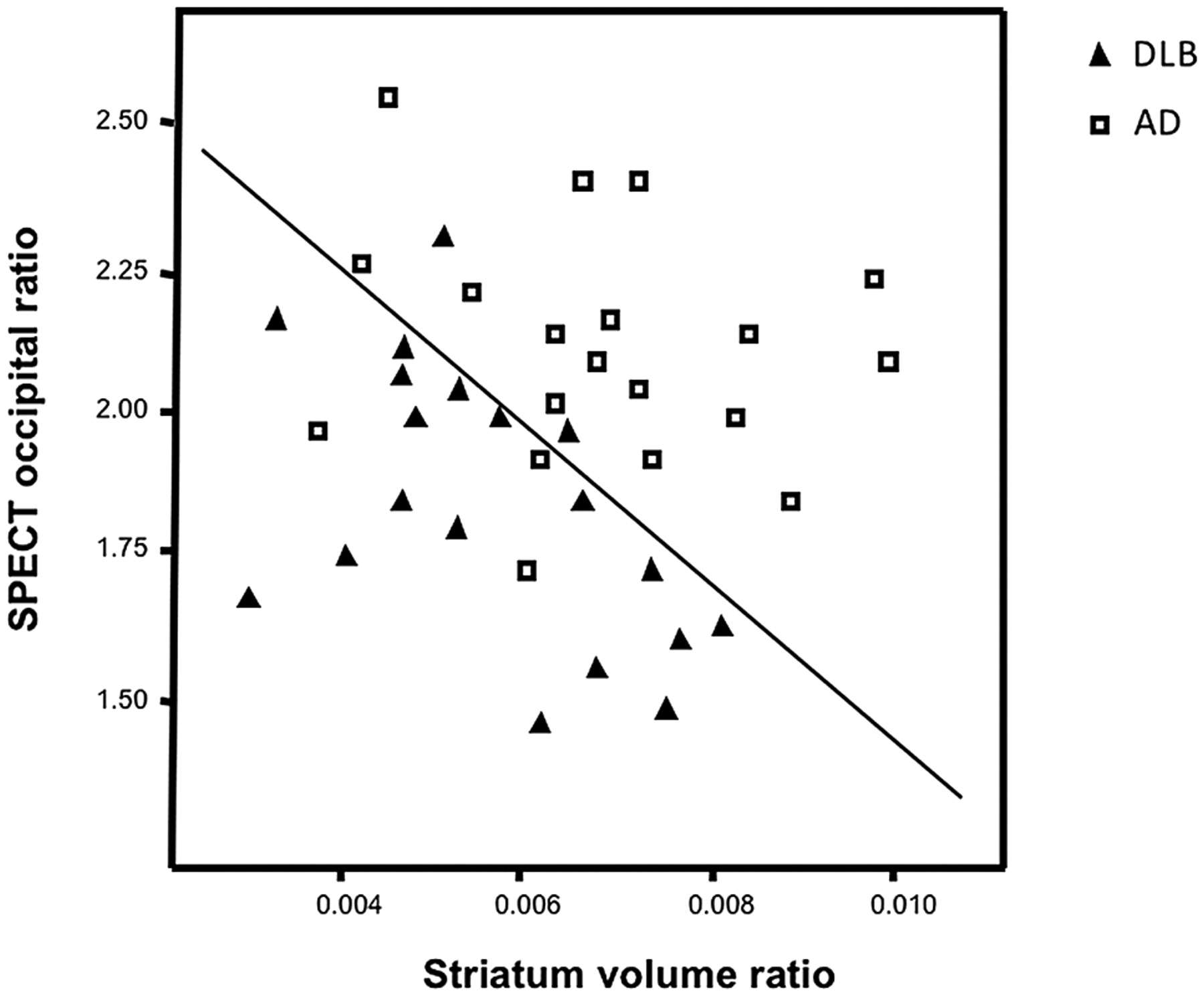
Distribution of SPECT occipital ratio and the striatal volume ratio of patients with DLB and AD. The square indicates AD; the triangle, DLB.
Linear discriminant analysis was performed on the regional ratio of volume and SPECT counts. Statistical tests were made at the 0.05 level. All statistical analyses were performed with the SPSS 17 (SPSS, Chicago, Illinois; and the JMP 8. (http://tech.its.iastate.edu/macosx/howtos/jmp8.shtml).
Results
The Table shows the mean volume and SPECT count ratios of the DLB and AD groups. Patients with DLB showed a significantly lower GM volume in the striatum compared with those with AD (P < .05). Patients with DLB showed significant cerebral blood flow reductions in the occipital lobe (P < .05). Figure 2 shows the distribution of the striatal volume ratio and the SPECT occipital ratio of both groups. We obtained the following linear discriminant analysis formula: S = (SPECT occipital ratio) × 4.934 + (striatal volume ratio) × 474.136 − 13.803, with S < 0 diagnosed as DLB, and S > 0 diagnosed as AD. DLB was correctly diagnosed in 17 of the 19 patients by using this approach. Similarly, AD was correctly diagnosed in 16 of 19 patients. Therefore, the sensitivity and specificity for discriminating DLB from AD were 89% and 84%, respectively.
Mean volume ratio and SPECT counts ratio of the DLB and AD groups
Figure 3 shows the AUCs in the ROC analysis. For the combined striatal volume and occipital SPECT ratio, the AUC was 0.898; for the striatal volume ratio, the AUC was 0.679; and for the occipital SPECT ratio, the AUC was 0.798.

ROC curves to discriminate between DLB and AD. The measurement of the z-score in the combined striatal volume and occipital SPECT ratio yielded higher sensitivity and specificity (AUC = 0.898) (a) compared with the independent striatal volume ratio (AUC = 0.679) (b) or the independent occipital SPECT ratio (AUC = 0.798) (c).
Discussion
Several previous studies have reported that detecting occipital and parietotemporal hypoperfusion can be useful in distinguishing DLB from AD.18–21 However, hypoperfusion in the parietotemporal lobe has been observed in the brains of patients with both DLB and frontotemporal dementia,22–24 and brain perfusion SPECT in these 2 disorders can be similar to that seen in AD. A large degree of overlap also exists between AD and DLB in regional uptake patterns.25 Kemp et al26 reported that the appearance of the occipital perfusion decrease is of little use for differentiating DLB from other diseases. Overall, the contribution of occipital hypoperfusion to diagnostic accuracy remains unclear.27 It was, however, recently demonstrated that 123FP-CIT, a ligand that binds to the dopamine transporter, is useful for differentiating AD and DLB.28–32 O'Brien et al33 demonstrated the accuracy of 123I-FP-CIT SPECT in diagnosing patients with possible DLB. A presynaptic dopamine transporter imaging is useful for diagnosing patients with DLB, though it is used as an additional examination after perfusion SPECT study.
A recent systematic review of the use of hexamethylpropyleneamine oxime SPECT to distinguish AD from other dementias reported a sensitivity of approximately 70%.34 The authors of this article suggested that perfusion SPECT is unable to draw a clear line between AD and other dementias. Nevertheless, because all SPECT studies included in the study used perfusion SPECT alone, SPECT may still be helpful in the clinical diagnosis of DLB if used in conjunction with other neuroimaging techniques. PET has a higher sensitivity and a higher spatial resolution than SPECT, so it may be more suitable for distinguishing DLB and AD.35
Combining measures of metaiodobenzylguanidine cardiac uptake reduction and MMSE score-change patterns with SPECT reduction patterns has been found to increase the accuracy of differentiating DLB from AD.36,37 Moreover, MR imaging is widely available in general hospitals. We found that with a combination of MR imaging and SPECT, we were able to discriminate DLB and AD with high sensitivity and specificity. As shown in the ROC analysis, the AUC resulting from combined MR imaging and SPECT was higher than the AUC resulting from either technique alone. This finding shows that discriminative power can be increased by using MR imaging and SPECT in conjunction. Kitayama et al38 previously suggested the usefulness of a combined analysis of hippocampal perfusion and GM volume by using SPECT in conjunction with MR imaging for the early diagnosis of AD. The present study is the first showing a clear differentiation of DLB and AD by using combined MR imaging and SPECT. Our method needs SPECT and MR imaging studies, but dopamine-transporter SPECT alone does not give any cerebral perfusion state and a dopamine transporter study must be performed as an additional study after perfusion and MR imaging studies.
Several previous studies have produced results regarding striatal volume in the DLB-affected brain that conflict with the present findings.39–41 A voxel-based morphometry study with a large sample number of 72 patients with DLB and 72 patients with AD (28 confirmed by autopsy) did not report greater atrophy of the striatum in DLB than in AD.42 In a previous article, however, we demonstrated that striatal volume reduction was able to differentiate AD from DLB.14 Another study showed that patients with DLB exhibited a significantly smaller putaminal volume ratio than controls and patients with AD.43 Some pathophysiologic studies have reported morphologic changes associated with DLB. The lack of postmortem evidence of wallerian degeneration in the DLB brain44 and the presence of widespread spongiform changes and gliosis affecting long projection fibers are a part of DLB pathophysiology.45
Zaja-Milatovic et al46,47 reported evidence of spinodendritic degeneration of gamma-aminobutyric acidsergic medium spiny neurons in specific regions of the caudate nucleus. This may be a structural correlate of the impairments in executive function in patients with DLB, and such pathologic changes may explain the reduction of striatal volume in these patients. These previous findings are in accord with the present result of a significantly lower striatal volume in patients with DLB compared with those with AD. Additionally, patients with PD had significantly smaller subcortical nuclei than age- and sex-matched controls.48–50 The 68% of patients with DLB in our study had parkinsonism, and the striatal volume loss may depend on the parkinsonism related to Lewy body disease.
Several previous perfusion studies demonstrated that hippocampal volume and perfusion in patients with AD were significantly lower than those in patients with DLB.11,14,51,52 In the present study, no significant differences in hippocampal volume were found between patients with DLB and those with AD. However, this may be explained by the restriction of this study to patients with only mild DLB and AD. Furthermore, the lack of a hippocampal volume difference in the present study is in accord with the report of Barber et al53 that the presence of hippocampal atrophy is useful in detecting AD but less useful in differentiating dementias. Also, most of the patients with DLB in this study were elderly (mean age, 76.0 years), probably including those with the common type of DLB, and were affected in the hippocampus.
The limitation of this study is the small number of patients included, and validation of the discriminative model used in a different and larger cohort of patients is needed.
Conclusions
We demonstrated that a combined morphologic and functional approach by using MR imaging and SPECT may be a suitable approach for distinguishing DLB from AD with high specificity and sensitivity.
References
- Received June 14, 2009.
- Accepted after revision August 18, 2009.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.