
Abstract
BACKGROUND AND PURPOSE: Various endovascular techniques have been applied to treat blister-like aneurysms. We performed a systematic review to evaluate endovascular treatment for ruptured blister-like aneurysms.
MATERIALS AND METHODS: We performed a comprehensive literature search and subgroup analyses to compare deconstructive versus reconstructive techniques and flow diversion versus other reconstructive options.
RESULTS: Thirty-one studies with 265 procedures for ruptured blister-like aneurysms were included. Endovascular treatment was associated with a 72.8% (95% CI, 64.2%–81.5%) mid- to long-term occlusion rate and a 19.3% (95% CI, 13.6%–25.1%) retreatment rate. Mid- to long-term neurologic outcome was good in 76.2% (95% CI, 68.9%–8.4%) of patients. Two hundred forty procedures (90.6%) were reconstructive techniques (coiling, stent-assisted coiling, overlapped stent placement, flow diversion) and 25 treatments (9.4%) were deconstructive. Deconstructive techniques had higher rates of initial complete occlusion than reconstructive techniques (77.3% versus 33.0%, P = .0003) but a higher risk for perioperative stroke (29.1% versus 5.0%, P = .04). There was no difference in good mid- to long-term neurologic outcome between groups, with 76.2% for the reconstructive group versus 79.9% for the deconstructive group (P = .30). Of 240 reconstructive procedures, 62 (25.8%) involved flow-diverter stents, with higher rates of mid- to long-term complete occlusion than other reconstructive techniques (90.8% versus 67.9%, P = .03) and a lower rate of retreatment (6.6% versus 30.7%, P < .0001).
CONCLUSIONS: Endovascular treatment of ruptured blister-like aneurysms is associated with high rates of complete occlusion and good mid- to long-term neurologic outcomes in most patients. Deconstructive techniques are associated with higher occlusion rates but a higher risk of perioperative ischemic stroke. In the reconstructive group, flow diversion carries a higher level of complete occlusion and similar clinical outcomes.
ABBREVIATION:
- BLA
- blister-like aneurysm
Blister-like aneurysms (BLAs) are intracranial arterial lesions originating at nonbranching sites of the dorsal supraclinoid internal carotid artery and basilar artery. BLAs account for 0.3%–1% of intracranial aneurysms and 0.9%–6.5% of ruptured aneurysms.1⇓⇓⇓⇓–6 They are attributed to subadventitial dissections resulting in a focal wall defect with absence of internal elastic lamina and media, leading, in most cases, to acute subarachnoid hemorrhage. The arterial gap is only covered with adventitia and thin fibrinous tissue.4,7⇓⇓–10
Ruptured BLAs have a high mortality rate. Furthermore, treatment of these lesions is technically difficult because they often lack a defined neck and the aneurysm sac has a very thin wall.4,11⇓–13 Thus, ruptured BLAs are associated with high rates of spontaneous or treatment-induced rebleed and death, regardless of treatment type.2,4,13,14
Many surgical techniques such as wrapping or trapping with bypass have been described for the treatment of these lesions. However, such techniques are often associated with high perioperative morbidity and mortality rates.8,10,11,13,15⇓⇓⇓⇓–20 Because of these results, endovascular techniques, both reconstructive and deconstructive, have emerged as the treatment of choice due to perceived lower rates of treatment-related morbidity and higher efficacy.2⇓–4,12,21⇓⇓⇓–25 However, because of the rarity of these lesions, most series on endovascular treatment of BLAs are small retrospective single-center case series. Thus, the efficacy and safety of endovascular treatment of these lesions have not been well-established.4 In addition, little is known regarding whether reconstructive techniques with parent artery preservation are associated with similar rates of angiographic occlusion and improved clinical outcomes compared with deconstructive parent artery sacrifice.13 Therefore, we performed a systematic review of the literature examining the overall efficacy of endovascular treatments for ruptured BLAs and comparing outcomes of reconstructive techniques such as stent placement, flow diversion, and stent-assisted coiling with deconstructive techniques such as parent artery occlusion and trapping. We also performed a subgroup analysis comparing the safety and efficacy of flow-diverter treatment with other reconstructive techniques.
Materials and Methods
Literature Search
We identified all studies published between 1980 and November 2014 that reported patients treated with endovascular therapy for ruptured BLAs. A comprehensive literature search of the databases PubMed, Ovid MEDLINE, and Ovid EMBASE was designed and conducted by an experienced librarian with input from the authors. The key words “blister,” “aneurysm,” “endovascular,” “coil,” “clip,” “stent,” “intravascular,” and “flow diverter” were used in both “AND” and “OR” combinations. Studies were selected by using the following criteria: 1) ruptured BLAs treated by an endovascular approach; 2) involving subjects 18 years of age or older; 3) with available data on clinical and/or angiographic outcomes; 4) retrospective or prospective with at least 3 patients; and 5) published in English.
Two authors jointly searched the data base and selected potentially relevant articles on the basis of the title and abstract and obtained the full text for detailed review. We also searched the reference lists of retrieved articles and published review articles for additional studies. We also screened duplicate publications that drew on the same datasets (ie, data overlapped that in other included studies); only the publication with the most complete data was included. The included studies reported their own definition of blister aneurysms with homogeneity in the classification as small lesions without a defined neck located at nonbranching sites. The included series are homogeneous according to the definition of blister aneurysms as small lesions without definite neck located at nonbranching sites and with a dome/neck ratio of <1. Some included cohorts reported larger aneurysms, which are mainly a recurrence after a first treatment. All of the included series stated that the aneurysms were all blister aneurysms according to their “Materials and Methods” section.
Data were extracted independently by 2 authors by using a standardized form, and any disagreement was resolved by consensus. We did not contact the authors of the studies to request incomplete or unpublished data. For each study, we extracted the following data: patient demographics, initial clinical status (Hunt and Hess scale grade), treatment technique (coiling, stent-assisted coiling, stent placement alone, flow-diverter stent, endovascular parent artery occlusion), immediate angiographic occlusion, mid- to long-term angiographic occlusion, perioperative morbidity (resulting from procedural complications), perioperative mortality (all causes), rebleeding (for ruptured only), recurrence, retreatment, and mid- to long-term good neurologic outcome (>3 months of follow-up). Good neurologic outcome was defined as a modified Rankin Scale score of ≤2. In cases in which a modified Rankin Scale score was not available, good neurologic outcome was determined if the study used terms such as “no morbidity” or “good recovery.”
Outcomes were obtained for the overall population of patients receiving endovascular treatment of ruptured BLAs. Separate analyses were also performed comparing outcomes between patients receiving reconstructive techniques with preservation of the parent artery, including coiling, stent placement, stent-assisted coiling, or flow-diverter stent versus those undergoing deconstructive techniques such as endovascular trapping or parent artery occlusion. Patients undergoing parent artery occlusion with surgical bypass were excluded. In addition, we compared outcomes between patients treated with a flow-diverter stent versus other reconstructive endovascular treatments.
Statistical Analysis
All included studies were noncomparative. From each cohort, we estimated the cumulative incidence (event rate) and 95% confidence interval for each outcome. Event rates for each intervention were pooled in a meta-analysis across studies by using the random effects model.26 Anticipating heterogeneity among studies, we chose this model a priori because it incorporates within-study variance and between-study variance. For all outcomes, we quantified between-study heterogeneity by using a homogeneity test based on the Cochran Q statistics and by calculating the I2 statistics.27
Results
Literature Review
The initial literature search yielded 157 articles. On initial abstract and title review, we excluded 72 studies: 20 studies because they dealt with surgical treatment, 20 because they did not report detailed outcomes for blister aneurysms, and 32, because they were either case reports or had fewer than 3 patients. Eighty-five studies were reviewed in additional detail. Of them, 20 were excluded because they reported only surgical treatments; 24, because they did not report detailed clinical outcomes; and 10, because they were review articles. The identified non-English publications excluded from the analysis were all case reports with fewer than 3 patients.
In total, 31 studies with 258 patients with ruptured BLAs were included. Seventy-three percent of patients were women, their mean age was 47.6 years (range, 19–84 years), 19.3% (44/228) of patients had a grade 4 or 5 Hunt and Hess scale hemorrhage, and the mean dome size of the blister aneurysms was 2.4 mm (range, 1–12 mm). This wide range in the aneurysm sizes, up to 12 mm, is because blister aneurysms are characterized by early frequent recurrence and some of the studies from our analysis included regrowth of blister aneurysms. Overall, 265 procedures were included; of them, 25 treatments (9.4%) were deconstructive techniques and 240 procedures (90.6%) were reconstructive techniques. Of the 240 reconstructive procedures, 62 (25.8%) involved flow-diverter stents and 178 were non-flow-diverter reconstructive techniques with stent-assisted coiling in 106, coiling with or without balloon remodeling in 15, stent placement (1 or several overlapped stents) in 45, Onyx (Covidien, Irvine, California) with stent in 3, and merged reconstructive techniques in 9. Mean follow-up was 14.2 months (range, 1–54) with at least 6 months for 23 of the 31 studies. A summary of the included studies is provided in the On-line Table.
Overall Outcomes of Endovascular Treatment of Ruptured BLAs
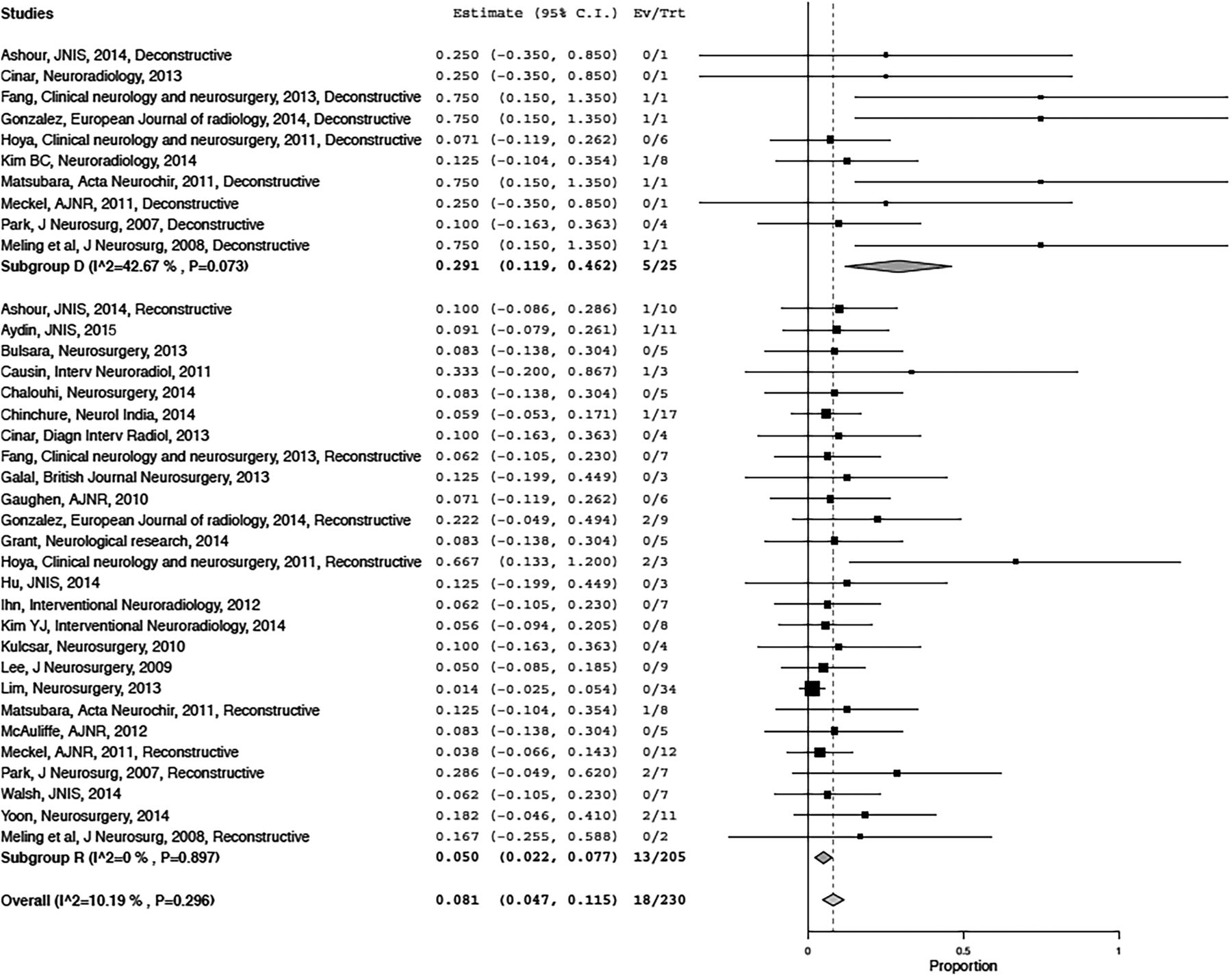
When we considered all patients treated with either reconstructive or deconstructive techniques, immediate occlusion rate was 40.6% (62/172; 95% CI, 28.5%–52.7%) and mid- to long-term occlusion rate was 72.8% (197/266; 95% CI, 64.2%–81.5%). The retreatment rate was 19.3% (52/265; 95% CI, 13.6%–25.1%). Perioperative intracranial hemorrhage occurred in 7.0% (18/245; 95% CI, 4.1%–9.9%) of procedures and rebleeding of the BLA occurred in 8.3% (17/242; 95% CI, 5.0%–11.5%) of cases. The overall perioperative complication incidence rate was 12.6% (37/251; 95% CI, 8.3%–16.8%). The perioperative morbidity rate was 13.4% (34/225; 95% CI, 8.9%–17.9%), and the perioperative stroke rate was 8.1% (18/230; 95% CI, 4.7%–11.5%). All-cause perioperative mortality was 7.3% (16/265; 95% CI, 4.4%–10.1%). Mid- to long-term neurologic outcome was good in 76.2% (207/265; 95% CI, 68.9%–8.4%) of patients. These data are summarized in Table 1.
Outcomes of the overall population
Deconstructive versus Reconstructive Techniques
Patients treated with deconstructive techniques had higher rates of complete occlusion on immediate posttreatment angiography than those treated with reconstructive techniques (77.3% versus 33.0%, P = .0003, Fig 1) but had a higher risk for perioperative stroke (29.1% versus 5.0%, P = .04, Fig 2). No other statistically significant difference was noted between deconstructive and reconstructive techniques for the treatment of ruptured BLAs. Specifically, mid- to long-term good clinical outcome rates were similar between the reconstructive (76.2%; 95% CI, 67.5%–84.8%) and deconstructive groups (79.9%; 95% CI, 64.7%–95.0%) (P = .30). These data are summarized in Table 2.

Meta-analysis. Comparison of initial occlusion rates between deconstructive and reconstructive techniques.

Meta-analysis. Comparison of the perioperative stroke rate between deconstructive and reconstructive techniques.
Meta-analysis—comparison of outcomes with deconstructive versus reconstructive techniques
Flow-Diverter Arterial Reconstruction versus Other Non-Flow-Diverter Reconstructive Techniques
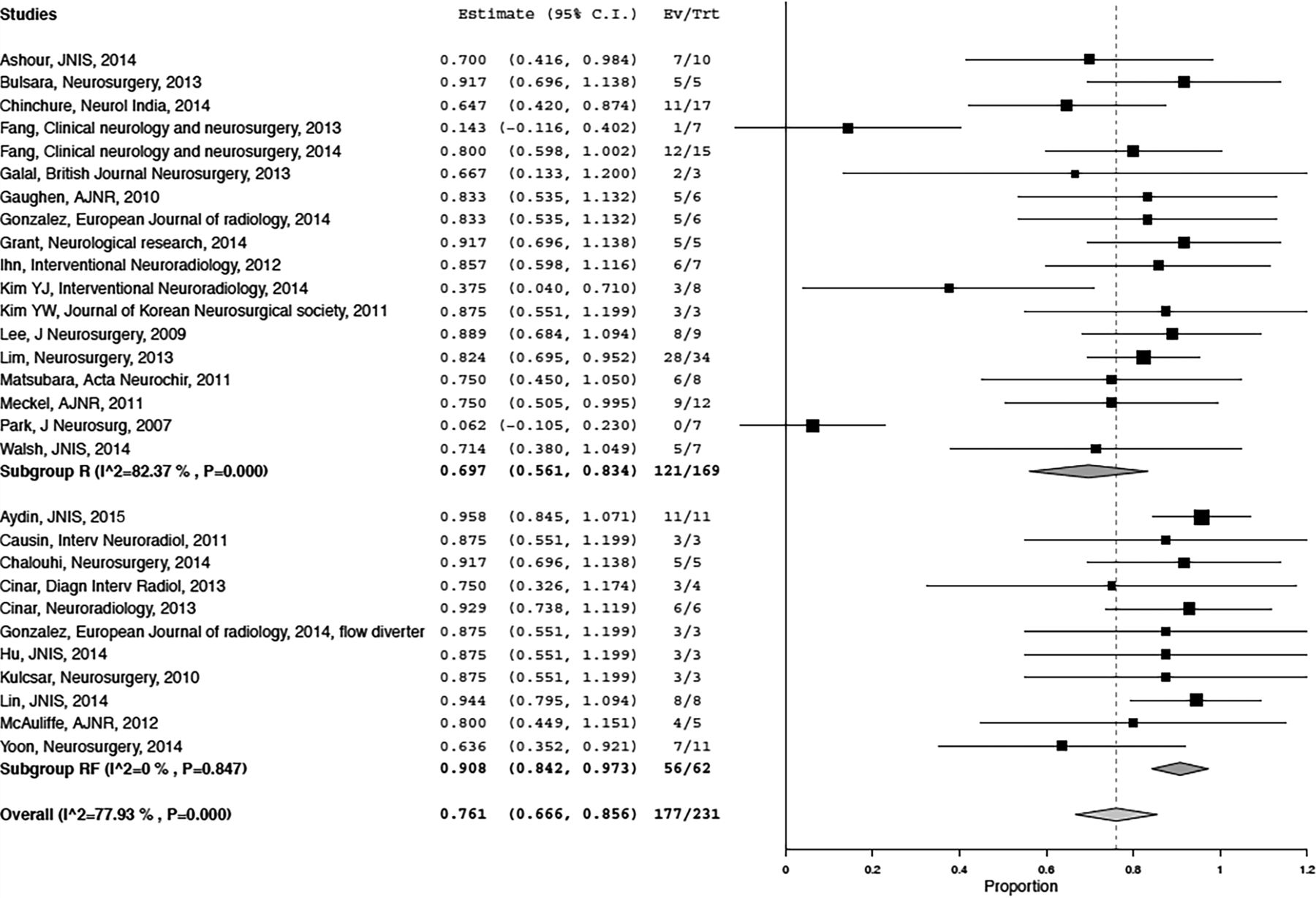
Patients treated with flow-diverter stents had higher rates of mid- to long-term complete occlusion than those treated with other reconstructive techniques (90.8% versus 69.7%, P = .005, Fig 3) and a lower rate of retreatment (6.6% versus 27.1%, P = .0002, Fig 4). Perioperative morbidity rates were similar in the flow-diverter group compared with the non-flow-diverter reconstructive group (12.6% versus 13.2%, P = .64). Perioperative mortality was 8.7% (95% CI, 2.1%–15.2%) in the flow-diverter group versus 7.2% (95% CI, 3.5%–15.9%) in the non-flow-diverter reconstructive group (P = .46). Mid- to long-term good clinical outcome rates were statistically similar between the flow-diverter group (86.0%; 95% CI, 77.8%–94.2%) and non-flow-diverter reconstructive group (75.0%; 95% CI, 63.7%–86.2%) (P = .23). Perioperative intracranial hemorrhage rates were similar between the flow-diverter (7.6%; 95% CI, 0.8%–14.9%) and non-flow-diverter reconstructive group (6.3%; 95% CI, 2.6%–9.7%) techniques (P = .21). These data are summarized in Table 3.

Meta-analysis. Comparison of mid- to long-term occlusion rates between non-flow-diverter reconstructive techniques and flow-diverter techniques.

Meta-analysis. Comparison of retreatment rates between non-flow-diverter reconstructive techniques and flow-diverter techniques.
Meta-analysis—comparison of outcomes with flow-diverter versus non-flow-diverter reconstructive techniques
Discussion
Our meta-analysis demonstrated that both deconstructive (endovascular parent artery occlusion) and reconstructive (stenting/stent-assisted coiling/flow-diversion) techniques are effective in the treatment of ruptured BLAs. Deconstructive techniques achieved higher rates of initial complete angiographic occlusion compared with reconstructive techniques, albeit with higher rates of periprocedural stroke. However, there were no statistically significant differences between deconstructive and reconstructive techniques on mid- to long-term occlusion rates, retreatment, rebleeding, or clinical outcomes. Stroke severity was not reported in most of the studies; but it is possible that perioperative strokes were minor and did not result in substantial morbidity. Overall, these findings suggest that reconstructive techniques are as effective and potentially safer than endovascular parent artery occlusion, considering the ischemic risk. These findings are important, especially in deciding treatment options for patients who cannot tolerate parent artery occlusion.
When considering differences between different reconstructive techniques, our meta-analysis demonstrated that flow-diverter stents result in better occlusion rates and lower retreatment rates than non-flow-diverter reconstructive techniques (simple coiling, stent-assisted coiling, or overlapped stents). We found a trend toward better clinical outcomes with flow-diverter techniques, but our results were not statistically significant. These findings are particularly important given the increased use of flow-diverter stent placement in the treatment of complex intracranial aneurysms.
Most interesting is the higher rate of the overall mid- to long-term occlusion (72.8%; range, 64.2%–81.5%) compared with initial occlusion (40.6%; range, 28.5%–52.7%). We suppose that this improvement is mainly due to the remodeling after flow diversion because the patients treated with flow-diverter stents experienced an occlusion rate increase from 35.9% to 90.8%, while patients treated with non-flow-diverter reconstructive techniques experienced an increase from 32.8% initial occlusion to 67.9% at mid- to long-term follow-up and occlusion rates were quite stable for deconstructive techniques, varying only from 77.3% to 81% between initial and mid- to long-term evaluations. This increase in occlusion rates is potentially also driven by the interruption of antiplatelet treatment for flow-diversion and non-flow-diversion reconstructive techniques.
Comparing the safety and efficacy of various surgical and endovascular techniques in the treatment of BLAs is difficult because most studies were small single-center case series and did not compare the efficacy of various treatments. One recent systematic review published by Gonzalez et al4 evaluated the overall outcomes of patients with BLAs but pooled patients with and without rupture and surgical with endovascular treatments. This previous review included 87 patients treated with a primary endovascular approach, with rates of morbidity and mortality for endovascular techniques slightly higher than the numbers presented here. In the Gonzalez et al4 study, surgical morbidity for BLAs was estimated to be 21%, with a mortality rate of 17%, which is much higher than that observed in our systematic review, suggesting a favorable efficacy and safety profile for endovascular treatment in the management of ruptured BLAs. The higher morbidity and mortality rates among surgically treated aneurysms may be partly because these aneurysms lack a definitive saccular component and the parent vessel wall is often friable and involves a long vessel segment. These qualities tend to result in high rates of intraoperative rupture.2,28
To date, no large studies have compared the safety and efficacy of deconstructive and reconstructive endovascular techniques in the treatment of BLAs, to our knowledge. Reconstructive techniques should be strongly considered over deconstructive techniques in the treatment of BLAs for the following reasons: First, many patients are unable to tolerate balloon test occlusion of the parent vessel, and in these situations, reconstructive techniques may be the only available treatment option. Vasospasm is a commonly reported complication of subarachnoid hemorrhage resulting from BLA rupture. Deconstructive techniques may interfere with endovascular access for the treatment of potential delayed vasospasm, whereas reconstructive techniques with preservation of parent artery flow would allow access and treatment of vasospasm, when needed.22 In addition, the preservation of the parent artery flow can also result in the preservation of normal intracranial vascular hemodynamics.4
A number of reconstructive techniques have been used in the treatment of BLAs. Previous studies have reported the use of a stent-in-stent technique to promote flow diversion and decrease the hemodynamic stress on the BLAs without an intrasaccular device. However, the results of such treatments are complicated by high recurrence rates and a risk for stent misdeployment.21,25,28⇓–30 Endovascular treatment by using a traditional approach of coil embolization (with or without adjunctive stent placement) is difficult because of the very small size of BLAs without a defined saccular component to allow the introduction of coils safely.3,13,31⇓–33 In fact, the placement of coils into the saccular component of BLAs is a potentially dangerous maneuver and may cause perforation and rehemorrhage.28 Furthermore, the effectiveness of coil embolization for the management of dorsal wall ICA aneurysms remains controversial.34 One major disadvantage of flow diverters is the need for dual antiplatelet therapy in the acute phase of ruptured aneurysms. However, despite the uniform use of these medications in the perioperative period among flow-diverter placements, this meta-analysis demonstrated similar rebleeding, hemorrhage, and clinical outcomes between flow-diverter and other reconstructive therapies and higher rates of angiographic occlusion with flow diverters. These results suggest that in the correct clinical setting, flow diverters may be superior to other reconstructive methods in the treatment of BLAs.
Strengths and Limitations
The strengths of this study include following: an a priori established protocol, a comprehensive literature search that involved multiple databases, and the process of study selection by independent reviewers. The main limitation of this analysis is the noncomparative nature of the studies. Our study undoubtedly has publication bias. Moreover, treatment modalities have varied during the time course of the published series; these differences make standardization of treatment paradigms difficult. Furthermore, given the small size of some of the treatment groups included in this analysis, our ability to detect differences among groups is limited. Last, uniform assessment and reporting of complications in a standardized fashion were lacking. When we used the Grading of Recommendations, Assessment, Development and Evaluation framework, the quality of evidence (confidence in estimates) was very low because of imprecision, heterogeneity, and methodologic limitations of the included studies; most important, they were noncomparative.35,36 Nevertheless, to the best of our knowledge, this systematic review is the first one focusing on endovascular treatment for ruptured BLAs. The last systematic review of BLAs published in 2014 by Gonzalez et al4 reported only 87 patients treated with a primary endovascular approach. Given the low number of reported BLAs and the difficulty of collecting prospective data, this meta-analysis provides useful information to share with patients and families when assessing the risks of treatment of BLAs and represents a benchmark against which future studies can be compared.
Conclusions
Endovascular treatment of ruptured BLAs is associated with high rates of complete occlusion and good mid- to long-term neurologic outcomes. Deconstructive techniques result in higher rates of immediate complete angiographic occlusion but carry a higher risk of ischemic complications compared with reconstructive techniques. Among reconstructive techniques, flow diversion appears to have a higher rate of complete occlusion and lower rate of retreatment. Use of either deconstructive or reconstructive endovascular treatment seems to be safe and effective in the right clinical setting. When one opts for the reconstructive treatment, flow diversion appears to be a reasonable choice despite the need for antiplatelet treatment.
Footnotes
Disclosures: David F. Kallmes—UNRELATED: Board Membership: GE Healthcare, Comments: Cost-Effectiveness Board; Consultancy: ev3,* Comments: planning and implementing clinical trials; Grants/Grants Pending: MicroVention,* Codman,* SurModics,* NeuroSigma,* Sequent,* Comments: preclinical and clinical research; Royalties: University of Virginia Patent Foundation, Comments: spine fusion. *Money paid to the institution.
Aymeric Rouchaud received financial support by a research grant from the French Society of Radiology and the Fondation Therese Planiol.
REFERENCES
- Received February 2, 2015.
- Accepted after revision April 9, 2015.
- © 2015 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Finnish flow diverter study: 8 years of experience in the treatment of acutely ruptured intracranial aneurysms
- The Safety and Efficacy of Flow Diversion versus Conventional Endovascular Treatment for Intracranial Aneurysms: A Meta-analysis of Real-world Cohort Studies from the Past 10 Years
- Endovascular Treatment of Ruptured Intracranial Blister Aneurysms: A Systematic Review and Meta-analysis
- Treatment of Ruptured Blister-Like Aneurysms with the FRED Flow Diverter: A Multicenter Experience
- Flow diversion treatment for acutely ruptured aneurysms
- Treatment of blood blister aneurysms of the internal carotid artery with flow diversion
- Stent and flow diverter assisted treatment of acutely ruptured brain aneurysms
- Acutely Ruptured Intracranial Aneurysms Treated with Flow-Diverter Stents: A Systematic Review and Meta-Analysis
- Surpass Streamline Flow-Diverter Embolization Device for Treatment of Iatrogenic and Traumatic Internal Carotid Artery Injuries