Abstract
SUMMARY: Children who present with acute transient focal neurologic symptoms raise concern for stroke or transient ischemic attack. We present a series of 16 children who presented with transient focal neurologic symptoms that raised concern for acute stroke but who had no evidence of infarction and had unilateral, potentially reversible imaging features on vascular and perfusion-sensitive brain MR imaging. Patients were examined with routine brain MR imaging, MRA, perfusion-sensitive sequences, and DWI. Fourteen (88%) children had lateralized MRA evidence of arterial tree pruning without occlusion, all had negative DWI findings, and all showed evidence of hemispheric hypoperfusion by susceptibility-weighted imaging or arterial spin-labeling perfusion imaging at presentation. These findings normalized following resolution of symptoms in all children who had follow-up imaging (6/16, 38%). The use of MR imaging with perfusion-sensitive sequences, DWI, and MRA can help to rapidly distinguish children with conditions mimicking stroke from those with acute stroke.
Children who present with sudden onset of focal neurologic symptoms raise concern for acute stroke and transient ischemic attack. Yet certain conditions, such as complex migraine, postictal hemiparesis, or conversion disorder, can imitate acute stroke and are considered “stroke mimics.” Patients with stroke mimics present with an acute onset of focal neurologic symptoms but, on further evaluation, do not have an infarction or hemorrhage. Rapid differentiation of a stroke mimic from a cerebrovascular emergency constitutes a critically important diagnostic step before the initiation of time-dependent treatment such as thrombolysis or thrombectomy. Neuroimaging and MR imaging, in particular, provide essential information in the diagnosis of stroke.1⇓–3 Diffusion imaging documents irreversible tissue infarction.1 Arterial spin-labeling and susceptibility-weighted imaging provide information on regional differences in brain perfusion, which can include the core infarct but also encompass tissue beyond it that is hypoperfused but not yet irreversibly infarcted.2,4 MRA, which is based on flow-related enhancement, is used for documentation of vascular attenuation or obstruction consistent with both a patient's clinical symptoms and core infarct location.3
We report a case series of 16 children with transient neurologic symptoms who had unilateral cerebral hypoperfusion and lateralized vascular pruning without associated diffusion abnormalities by MR imaging. The resolution of neurologic symptoms without stroke-specific intervention and the normalization of the initial MR imaging features in patients with follow-up imaging confirm this clinicoradiologic entity as a stroke mimic. Recognition of these imaging patterns may help distinguish true stroke requiring urgent intervention from a stroke mimic condition in children presenting acutely with focal neurologic symptoms.5
Case Series
Cases were collected retrospectively as part of a larger, institutional review board–approved review of children with transient neurologic symptoms presenting to a free-standing children's hospital. A total of 16 children met both the clinical criteria of transient focal neurologic symptoms and the imaging criteria of focal hypoperfusion and/or focal vascular pruning. We collected clinical information on each of the children, including symptoms at presentation, time from presentation to imaging, headache at presentation, and history of migraines. All clinical information was reviewed by a pediatric neurologist.
Clinical Features
Our cohort of 16 children included 6 females (38%). The children ranged from 2 to 16 years of age. Among the 16 children, 13 (81%) had headache at presentation. Only 6 (38%) had a previous diagnosis of migraine (Table 1). Most patients (94%) did not meet the International Classification of Headache Disorders criteria for hemiplegic migraine.6 All patients had complete resolution or marked improvement in symptoms by 24 hours after symptom onset. Only 6 (38%) had recurrence of transient neurologic symptoms since the initial presentation; none had stroke at the time of presentation or at follow-up. We had a median follow-up of 0.7 years with a range of 1 day to 3.4 years.
Clinical details of the presentation of the children
Imaging Approach and Features
MR imaging was performed at a median of 6.4 hours, with all patients imaged within 16.5 hours of presentation. All examinations were performed on a 3T Magnetom Skyra or Trio imaging system (Siemens, Erlangen, Germany) with a 32- or 64-channel head coil. All patients were examined with the standard institutional brain imaging sequences, including the following: sagittal T1 MPRAGE (TR = 1520–2530 ms, TE = 1.63–3.39 ms, section thickness = 0.90–1 mm, echo-train length = 1, matrix = 220–256/220–256, one or 4 excitations); axial fast spin-echo T2 (TR = 4400–14,143 ms, TE = 89–100 ms, section thickness = 2.5 mm, echo-train length = 13–19, matrix = 269–359/512, two-to-three excitations); axial T2 FLAIR (TR = 6800–9000 ms, TE = 135–137 ms, section thickness = 4 mm, echo-train length = 13–16, matrix = 250–320/320, one-to-two excitations); diffusion tensor imaging with 30 or 35 directions, b=1000 s/mm2 (TR = 5300–13,800 ms, TE = 88–92 ms, section thickness = 2–4 mm, echo-train length = 1,48, or 51, matrix = 128/128, one excitation); and 3D time-of-flight angiography (TR = 21–22 ms, TE = 3.43–3.88 ms, section thickness = 0.60–0.80 mm, echo-train length = 1, matrix = 230–344/384–512, one excitation). Perfusion-sensitive sequences, including perfusion-weighted pulsed arterial spin-labeling (n = 11 patients: TR = 2500–5000 ms, TE = 11–35 ms, section thickness = 3–5 mm, echo-train length = 1–51, matrix = 64–96/64–84, one-to-sixty excitations, TI = 700 ms); velocity-selective arterial spin-labeling (n = 2 patients: TR = 3000 ms, TE = 13 ms, section thickness = 5 mm, matrix = 64/64, one excitation, TI1 = 700 ms, TI1,stop = 1400 ms, and TI2 = 2000 ms [to the center section]); and axial susceptibility-weighted imaging (n = 16 patients: TR = 28 ms, TE = 20 ms, section thickness = 1.25 mm, echo-train length = 1, matrix = 184–336/256–384, one excitation) were also performed.
Images were independently reviewed by 2 pediatric neuroradiologists. The final interpretation was reached by consensus in cases of disagreement between the reviewers. Each MR imaging examination was evaluated for the following imaging abnormalities: linear sulcal signal abnormality on FLAIR imaging, subcortical hypointensity on T2-weighted imaging, localized brain parenchymal signal or diffusion abnormalities, gyral swelling, venous prominence on susceptibility-weighted imaging, perfusion abnormality on arterial spin-labeling, abnormal leptomeningeal and parenchymal enhancement following the administration of intravenous contrast, and evidence of increased/decreased flow-related enhancement or vessel stenosis on 3D TOF MR angiography. Imaging abnormalities were further characterized according to vascular distribution for MRA and lobes of the brain involved in SWI and arterial spin-labeling.
DWI revealed no areas of decreased diffusivity in any patient. None had evidence of gyral swelling. Linear sulcal signal abnormality in the hemodynamically affected region was seen on FLAIR imaging in 2 patients (2/16, 13%). One patient had subcortical hypointensity on T2-weighted imaging (1/16, 6%). All 16 patients had unilateral increased prominence of the cortical or medullary veins in ≥1 cerebral lobe on SWI, suggesting elevated venous deoxyhemoglobin, indicative of hypoperfusion. Of the 11 patients evaluated with arterial spin-labeling, decreased perfusion to ≥1 lobe of the brain was evident in all. Diminished flow-related enhancement due to decreased hemispheric flow in at least 1 branch vessel of the circle of Willis was evident in 14 patients (14/16, 88%). Multivessel unilateral vascular pruning was present in 9 patients. None of the patients demonstrated hemodynamic change in the posterior fossa structures. Arterial beading on MRA was not demonstrated in any patient. Intravenous contrast was administered in 3 patients (3/16, 19%) with increased leptomeningeal prominence seen in the regions corresponding to those with arterial spin-labeling, SWI, and MRA changes in all 3. No parenchymal enhancement was observed in any of the 3 patients administered contrast. The Figure represents an example of the imaging findings observed in our cohort. Follow-up imaging was performed in 6 patients (6/16, 38%). Resolution of MR imaging changes, including normalization of arterial spin-labeling, SWI, and MRA findings, was observed in all 6 patients who had follow-up imaging (Table 2).
{kind=link}
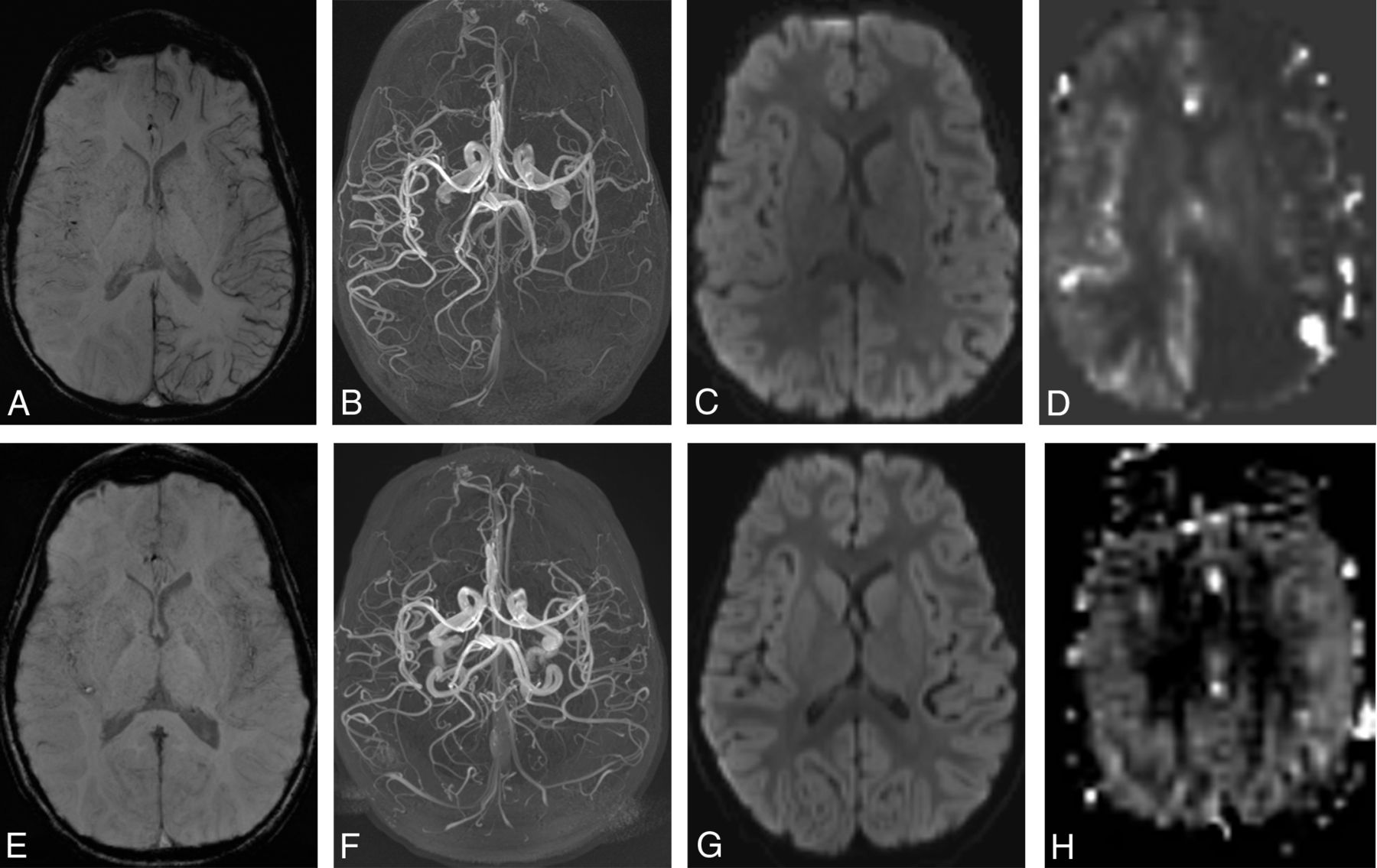
A 5-year-old boy presenting with right-sided weakness. Symptoms were improving at the time of the initial MR imaging performed 3 hours after presentation (A–D). A, Susceptibility-weighted imaging shows increased prominence of the cortical veins throughout the left cerebral hemisphere, indicating increased deoxyhemoglobin on the left. B, Collapsed maximum intensity projection from time-of-flight MR angiography shows reduced flow-related enhancement in the left anterior, middle, and posterior cerebral arteries. C, The average trace of the diffusion tensor image shows no abnormality of diffusion. D, Pulsed arterial spin-labeled perfusion-weighted imaging relative CBF map shows a marked decrease in perfusion throughout the left cerebral hemisphere. Follow-up imaging at 4 days after presentation (E–H). E, SWI shows resolution of venous asymmetry. F, MRA shows normal flow-related enhancement in the left anterior, middle, and posterior cerebral arteries. G, Findings of the average trace image continue to be negative. H, Pulsed arterial spin-labeling relative CBF map shows resolution of perfusion asymmetry.
Radiology findings of children with ASL and SWI reported in lobes and MRA in vessels involved
Discussion
We describe a cohort of children with a specific radiologic presentation that included negative diffusion-weighted imaging findings, evidence of lobar or hemispheric hypoperfusion by susceptibility-weighted imaging, and/or arterial spin-labeled perfusion imaging associated with transient focal neurologic symptoms. MRA evidence of arterial pruning without occlusion was usually present. In all children who had repeat imaging, the vascular and perfusion findings had normalized and there was no evidence of infarction. Most children had headache at presentation, and only one-third had recurrence of symptoms. Most interesting, only 1 of the children met the International Classification of Headache Disorders criteria for hemiplegic migraine.5,6
The literature describing the neuroimaging findings in children with transient focal neurologic symptoms is limited. Imaging findings of focal hypoperfusion and vascular pruning have been reported previously in pediatric and adult patients with hemiplegic migraine (genetically proved or clinically diagnosed) in case reports and small case series.7⇓–9 Perfusion findings have been reported and are temporally variable in children with acute onset of migraine with an aura. In a case-control study, 10 patients with migraine with an aura were acutely imaged with arterial spin-labeled perfusion imaging and found to have a change in perfusion compared with controls. The children had decreased perfusion if scanned <14 hours from the onset of symptoms, while evidence of increased perfusion was found if imaging was performed at >17 hours from symptom onset.10 In addition, Safier et al11 reported a series of 8 children with hemiplegic migraine who demonstrated vascular narrowing by MRA. However, in their case series, only the middle cerebral artery was examined.11 The study by Safier et al did not report on the other branch vessels of the circle of Willis. Consequently, it is not certain whether the vascular changes occurred in only the middle cerebral artery in their patients or if other vessels were similarly affected but not evaluated as part of the study. In our patient cohort, several branch vessels were usually affected.
Children who present with the acute onset of focal neurologic symptoms raise concern for stroke. Rapid neuroimaging of these children is extremely important, given the availability of treatment with thrombolysis or endovascular thrombectomy for acute stroke. DWI permits differentiation of a stroke from a stroke mimic.5 While negative DWI excludes an infarction requiring acute stroke therapy, the addition of perfusion-sensitive imaging in patients with diffusion-negative transient neurologic deficits can provide additional information regarding the etiology of the neurologic symptoms. Our findings indicate that a subset of children with symptoms mimicking acute stroke lack the anatomic or diagnostic diffusion-related changes of infarction but exhibit perfusion and flow-related vascular changes indicating reduced regional perfusion as a cause of symptoms. All children in our cohort with anatomic- and DWI-negative but perfusion-positive imaging findings demonstrated decreased rather than increased regional perfusion. The decreased perfusion findings in these children help to differentiate symptoms due to an ischemic cause from other conditions that may mimic stroke, such as a postictal state that typically shows increased regional blood flow.12⇓–14
We recognize limitations in our study. Our series is retrospective in nature and small in number. Furthermore, only a portion of the children we report had repeat imaging following resolution of symptoms. Finally, we have only limited outcome information.
Conclusions
The use of combined MR imaging to include perfusion-sensitive, diffusion-weighted, and angiographic imaging can help to rapidly distinguish children who present with stroke mimics whose symptoms are likely to be transient and who do not require stroke treatment from those with an acute stroke. In our series, the imaging findings of unilateral, often multilobar, hypoperfusion and arterial vascular pruning without evidence of diffusion restriction in a child presenting with focal neurologic symptoms reflect a benign stroke mimic and confirm a vasoconstrictive basis for the patient's symptoms. Our observations support the routine use of perfusion-sensitive sequences as part of the neuroimaging evaluation of any child presenting with stroke or strokelike symptoms.
Footnotes
R.L. Robertson and M.J. Rivkin are co-senior authors.
Disclosures: Richard L. Robertson—UNRELATED: Other: GE Healthcare*. *Money paid to the institution.
References
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- Received January 30, 2017.
- Accepted after revision May 9, 2017.
- © 2017 by American Journal of Neuroradiology