
Abstract
Summary: We describe a new sequence, flow artifact–insensitive fluid-attenuated inversion recovery (FAIS-FLAIR), that capitalizes on the advantages of fluid-attenuated inversion recovery (FLAIR) while minimizing FLAIR-related artifacts such as those often encountered in the posterior fossa. Twenty-eight patients with posterior fossa disease underwent FAIS-FLAIR, conventional FLAIR, and spin-echo MR studies, and the findings yielded by the three techniques were compared. In this patient population, postcontrast FAIS-FLAIR imaging was obtained in 20 patients and compared with postcontrast T1-weighted images. The images were assessed for lesion conspicuity by three radiologists. FAIS-FLAIR markedly reduces the inflow artifacts from noninverted CSF on FLAIR images. It does so with and without contrast agent administration, and produces higher lesion conspicuity compared with T1- and T2-weighted spin-echo sequences and conventional FLAIR images of the posterior fossa.
The high sensitivity of the fluid-attenuated inversion-recovery (FLAIR) sequence has already been established in a wide range of CNS disease processes (1–15). In spite of the advantages of FLAIR imaging, however, CSF inflow artifacts shown with this technique demand improvement.
Previous reports have described in detail inflow artifacts, related to noninverted CSF on FLAIR images, that frequently mask subtle lesions in the basal cisterns, ventricular atria, suprasellar cistern, and posterior fossa (7, 11, 16). These locations are deemed especially troublesome with regard to hyperintense FLAIR-related flow artifacts.
Technically, the attenuation of the otherwise hyperintense CSF can be achieved with FLAIR imaging by targeting selective inversion prepulses on each slice to accomplish signal nulling of CSF. The flow artifact–insensitive FLAIR (FAIS-FLAIR) sequence overcomes the problem of flow artifacts associated with FLAIR by using a nonselective inversion pulse.
Description of Technique and Results
FAIS-FLAIR is a modified FLAIR sequence using a specifically added nonselective inversion pulse. Although nonselective FLAIR (using fast spin-echo imaging with an initial unselected 180° inversion prepulse) can reduce inflow CSF artifacts, image contrast is not constant, and an insufficient number of slices may be generated. With FAIS-FLAIR, images are acquired by two scans that are obtained in reverse order of slice excitation, and corresponding location images from each sequence are summed in order to create tailored signal intensity for each slice and constant slice contrast. Therefore, this results in FLAIR images without highlighted inflow artifact at the aqueduct, the foramen of Monro, the third ventricle, and the cerebellopontine angle cisterns (Fig 1).
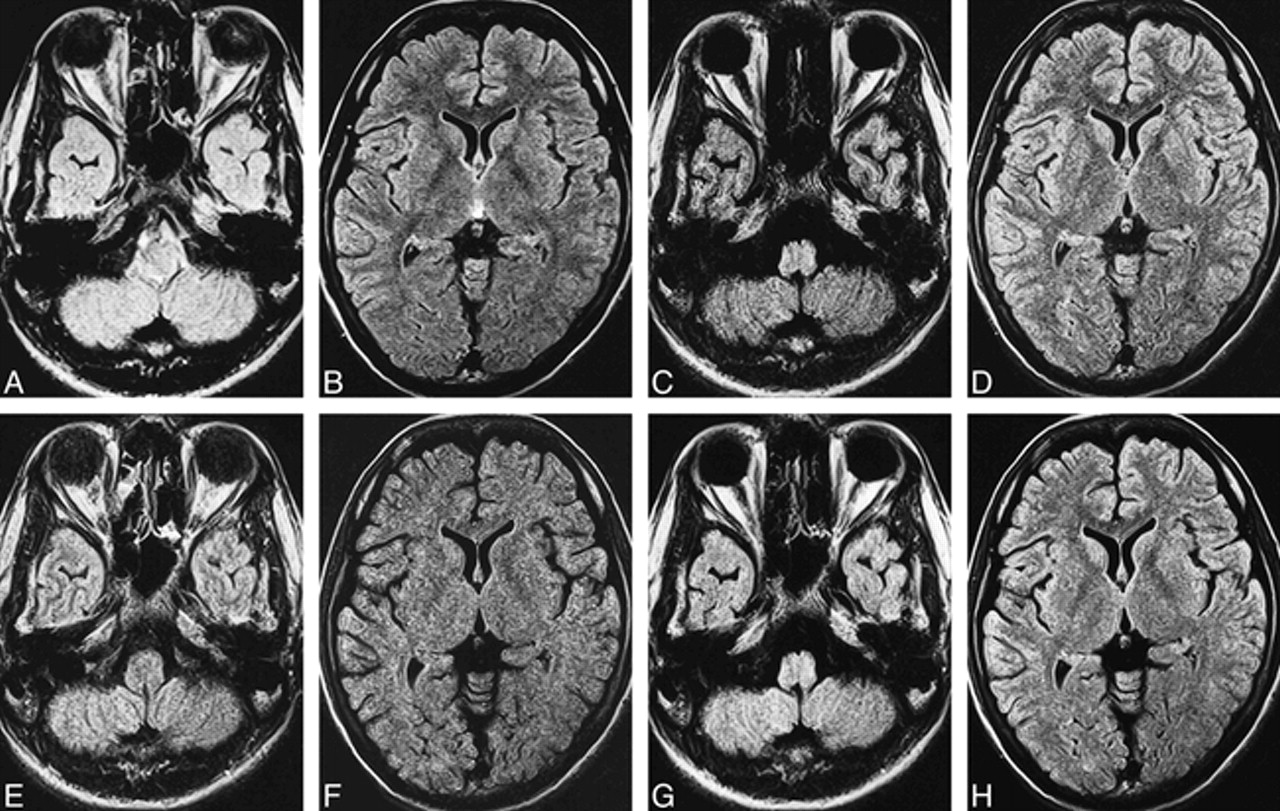
Conventional FLAIR images showing artifacts in the cerebellopontine angle cistern (A) and in the third ventricle (B). By combining the information from two reverse-ordered sequences, Scan 1 (C, D) and Scan 2 (E, F), the FAIS-FLAIR images result in a conspicuous absence of flow-related FLAIR artifacts (G, H). It is a simple summation of images, which are processed automatically in line with the image-array processor. Note flow-related artifacts lessen on Scan 1 and Scan 2, but image contrast is not constant. On Scan 1, signal intensity is increasing from C to D, whereas on Scan 2, it is decreasing from E to F.
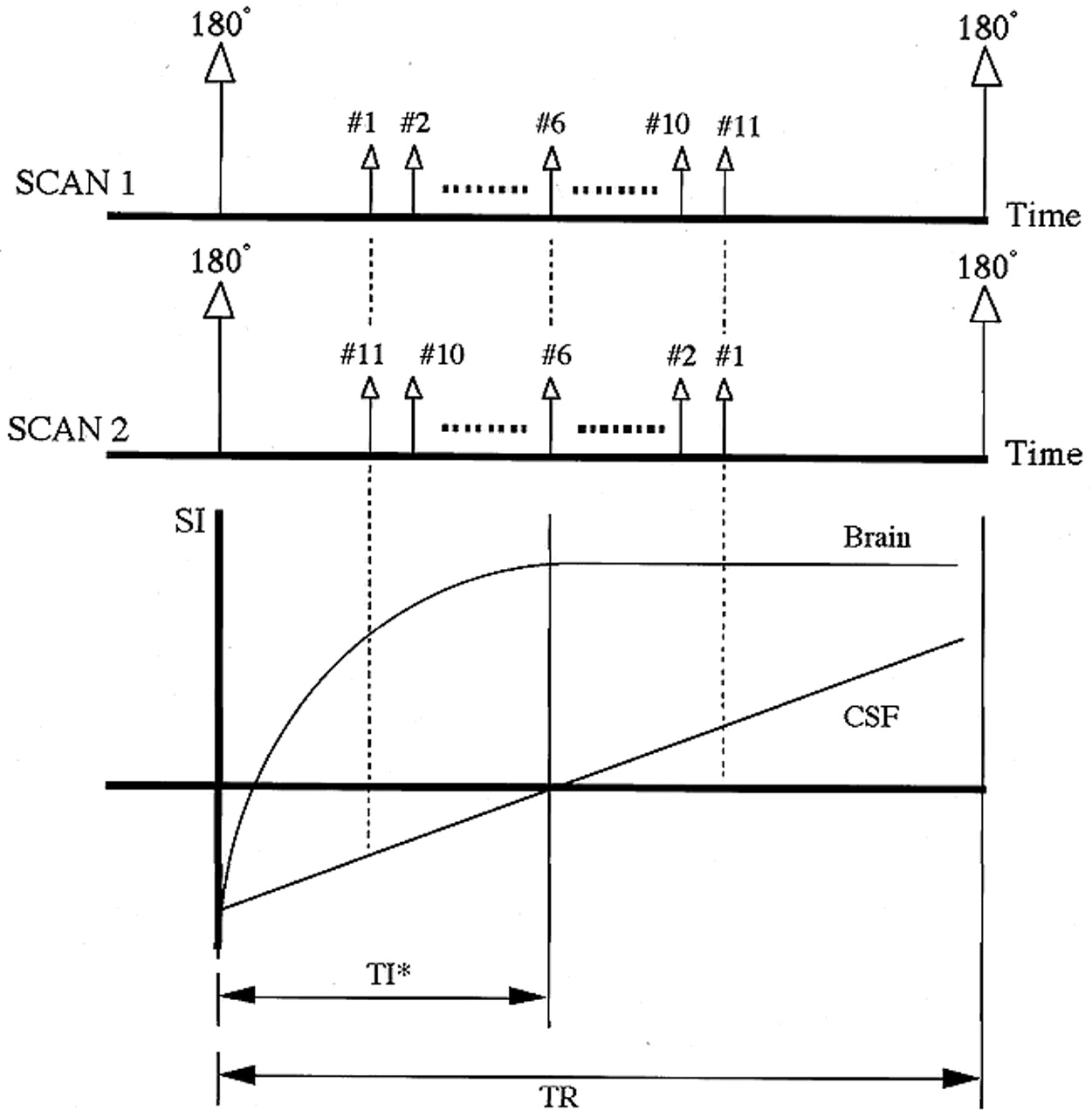
Twenty-eight patients (7 male, 21 female; mean age49.4 years) with posterior fossa disease were examined with FAIS-FLAIR MR imaging in addition to T1- and T2-weighted spin-echo sequences. Postcontrast FAIS-FLAIR and T1-weighted images were obtained from 20 of these 28 patients. The clinical diagnoses included nine cases of neuroma/schwannomas, five meningiomas, three metastases, three astrocytomas, and one each of the following: epidermoid and potine hemorrhage, cerebellar infarction, subarachnoid hemorrhage, cerebellar infarction, choroid plexus papilloma, meningosarcoma, cavernous hemangioma, and fungal meningitis. MR imaging was performed with a 1.5-T MR unit, and a birdcage receiver head coil was used. The FAIS-FLAIR sequence is illustrated in Figure 2. The FAIS-FLAIR sequence as implemented consists of two scans. In the first scan, a 180° inversion prepulse is nonselectively applied to the whole brain, and is then followed by a multislice fast spin-echo sequence. The intent of the prepulse is to null the water-dependent signal by inducing a delay before the center-slice excitation. The second scan consists of similar parameters as the first, with the exception that each slice is excited in reverse order.

The FAIS-FLAIR sequence consisted of two scans. On the first scan, a 180° inversion prepulse is nonselectively applied to the whole brain, and is then followed by a multislice fast spin-echo sequence. The intent of the prepulse is to null the water-dependent signal by inducing a delay before the center-slice ex
The FAIS-FLAIR scanning parameters used in this study were: 8000/2340/110/1 (TR/TI*/TEeff/excitations); echo train length, 5; 8-mm slice thickness with 2-mm interslice gaps;22-cm field of view; and 256 × 256 matrix. Half-Fourier transformation was used to reduce acquisition time, and the total acquisition time of the two scans was 4 minutes 28 seconds. Because of varying TI relaxation, the dependent image contrast was expected to differ when comparing similarly located slices on each of the two scans. The two images were averaged in a composite manner, so that we could tailor the signal intensity of each slice.
Protocols used for comparison included a T1-weighted spin-echo sequence (500/15/1 [TR/TE/excitations], 8-mm slice section thickness with 2-mm interslice gaps, 256 × 256 matrix, 22-cm field of view). The fast spin-echo T2 parameters included: 4500/112/1, an echo train length of 9, an 8-mm slice thickness and 2-mm interslice gaps, a 512 × 512 matrix, and a 22-cm field of view. The conventional fast-FLAIR sequence was performed with the following parameters: 6800/110/1700/1 (TR/TE/TI/excitations), 8-mm slice thickness and 2-mm interslice gaps, 256 × 256 matrix, and 22-cm field of view.
The T1- and T2-weighted, spin-echo, and FAIS-FLAIR images, including 20 postcontrast images, were assessed for lesion conspicuity by three radiologists. The lesion conspicuity comparisons were performed between FAIS-FLAIR and T1-weighted spin-echo, FAIS-FLAIR and T2-weighted spin-echo, and postcontrast FAIS-FLAIR and postcontrast T1-weighted spin-echo images. Additionally, FAIS-FLAIR sequences were compared with conventional fast-FLAIR sequences to assess absence of CSF-flow artifacts. Lesion conspicuity on FAIS-FLAIR images was superior to that on T1-images in 21 of 28 cases and was equal in four cases. In three cases, T1-weighted images were superior to FAIS-FLAIR for showing lesion conspicuity. Compared with T2-weighted images, FAIS-FLAIR produced superior lesion conspicuity in 21, equal conspicuity in five, and inferior conspicuity in two cases.
An illustrative case of a vestibular schwannoma revealed the superior lesion conspicuity on FAIS-FLAIR images when compared with spin-echo and FLAIR images (Fig 3). In this particular example, the FAIS-FLAIR image shows greater conspicuous enhancement when compared with the T1-weighted images, and also shows a lack of inflow artifacts, which interfere with the conventional FLAIR image set. In spite of our success with obtaining postcontrast FLAIR images, there have been only a few reports of postcontrast FLAIR imaging (12, 17). Compared with postcontrast T1-weighted imaging results, we found that lesion conspicuity on postcontrast FAIS-FLAIR images was superior in nine, equal in seven, and inferior four cases. In four cases, we performed conventional FLAIR imaging in addition to FAIS-FLAIR imaging to compare lesion conspicuity shown by these two sequences. In all four cases, the lesion conspicuity found with FAIS-FLAIR was found to be superior to that of conventional FLAIR, presumably because of greater lesion-to-CSF contrast from more effectively nulled CSF inflow artifacts (Fig 3).

A vestibular schwannoma is demonstrated on multiple images in a 58-year-old woman, including unenhanced conventional FLAIR (A), unenhanced (B) and enhanced (C) FAIS-FLAIR, and T1-weighted (D) images. FAIS-FLAIR shows the tumor in the cerebellopontine cistern more clearly than does T1-weighted imaging. The same lesion is even more visible with postcontrast FAIS-FLAIR imaging. On the FLAIR image, the tumor is depicted, but inflow artifacts in the cerebellopontine and prepontine cistern interfere with interpretation citation. The second scan consists of parameters similar to the first, with the exception that each slice is excited in reverse order. TI* means the interval between 180° inversion prepulse and the excitation pulse of the center slice
Discussion
Numerous prior reports have demonstrated specific advantages of FLAIR sequences when compared with more conventional spin-echo sequences. The advantages of FLAIR imaging relate to its high sensitivity for a variety of pathologic processes including cerebral infarction, trauma, multiple sclerosis, subarachnoid hemorrhage, epilepsy, infectious and inflammatory processes, and intracranial tumors (1–15). FLAIR imaging in the posterior fossa is complicated by flow-related phenomena in the basal cisterns and several authors have specifically reported the inflow artifacts from noninverted CSF, which are present on FLAIR images, and can mask pathologic abnormalities (7, 16).
Patients who may manifest posterior fossa artifacts on conventional FLAIR images have narrow prepontine, perimesencephalic, and perimedullary cisterns, and CSF accelerates when passing through these constrained regions. Alternatively, in young patients in whom the flow of the CSF is relatively rapid, the inflow artifacts may also be more prominent. These disadvantages may be easily addressed by the FAIS-FLAIR approach by performing two reverse-order scans with summation, yielding improved CSF saturation even in areas of expected artifact generation.
With our technique, FAIS-FLAIR was superior to conventional pre- and postcontrast T1- and T2-weighted images when assessing lesion conspicuity. Additionally, FAIS-FLAIR images were better for assessing lesions in the posterior fossa when compared with conventional FLAIR images. This improved conspicuity of FAIS-FLAIR may be attributed not only to the considerable increase in lesion-to-CSF contrast found by more optimally nulling CSF signal, but also is believed to be at least in part because of suppressed hyperintense marrow signal found surrounding the cerebellopontine angle cistern on T1-weighted images after intravenous administration of gadolinium.
Of particular interest is the fact that postcontrast FAIS-FLAIR images produced greater or equal lesion conspicuity compared with postcontrast T1-weighted images in nine of 20 assessed cases. The MR contrast agents in clinical use are mostly gadolinium-based, and as paramagnetic metal ions, they shorten the T1 of the tissues in which they accumulate. Although there is also a T2 shortening effect, this has been thought of little consequence in the low reactive concentrations used clinically (18). The conventionally generated FLAIR images produce T2-weighted, CSF-nulled images by coupling an inversion pulse followed by a long inversion time to a long echo time readout (19). As such, the potential utility of MR contrast agents when combined with FLAIR sequences, which may be considered T2-weighted, has not been used to full advantage. Our results support the usefulness of this particular combination. The T1 shortening effect with MR contrast agents results in an upward shift of the T1 relaxation curve during FLAIR imaging (Fig 4). The difference in signal intensity between the pre- and postcontrast T1 relaxation curves at the end of the inversion-recovery time is predictive of the amount of tissue contrast enhancement expected with FLAIR imaging.

The T1 shortening effect with MR contrast agents results in an upward shift of the T1 relaxation curve during FLAIR imaging
As a result of this preliminary data, we believe that FAIS-FLAIR is not only preferable to conventional FLAIR imaging in specific applications, such as when evaluating the posterior fossa, but is superior to conventional T1-weighted postcontrast sequences when assessing the posterior fossa. These advantages are especially apparent at the periphery of the cerebellum adjoining the brain stem, in the internal auditory canal area, and in the periventricular region where the inflow artifacts of CSF often interfere with interpretation of FLAIR images. FAIS-FLAIR sequences with and without intravenous contrast administration may even prove sufficiently valuable to supplant spin-echo sequences as a basic screening or postoperative examination for posterior fossa evaluation. In spite of our cautious enthusiasm, we recognize that clinical studies of a large number of patients with a wide range of disorders will be needed to establish the exact role of this new FAIS-FLAIR sequence.
Acknowledgments
We gratefully acknowledge the assistance of Alexander M. Norvash (Department of Interventional Neuroradiology, Massachusetts General Hospital) and Koji Shimizu (Shimadzu Corporation) for manuscript preparation.
Footnotes
1 Presented in part at the annual meeting of the American Society of Neuroradiology, Toronto, May 1997.
↵2 Address reprint request to Norimitsu Tanaka, M.D.
References
- Received May 11, 1999.
- Accepted after revision December 27, 1999.
- Copyright © American Society of Neuroradiology




{kind=link}
{kind=link}
{kind=link}
{kind=link}