
Abstract
Summary: We present a case of nasopharyngeal teratoma that was discovered in association with a suprasellar heterotopic cerebellum in a newborn. Well-differentiated, heterotopic, cerebellar masses have been reported in the orbits, spine, and frontal encephalocele but not, to our knowledge, in the suprasellar region. In this report, we describe the imaging findings and discuss the possible origins of the two masses discovered in this case.
Well-organized, dysplastic collections of cerebellar cells resting at inappropriate locations in the cerebellum are common abnormalities, but these rarely cause any structural defects (1). On the other hand, a mass of heterotopic cerebellar tissue in locations far away from its normal position is distinctly uncommon. Such cerebellar heterotopias have been described in the spine and orbits in association with Chiari malformations and within frontal encephaloceles (2–4). The head and neck nasopharyngeal teratomas are presumed to arise from primitive germ cells that get trapped in the normal migratory channel during development. To our knowledge, there are no reports describing the occurrence of a nasopharyngeal teratoma in association with a suprasellar heterotopic cerebellum. Interestingly, well-formed cerebellar tissue occurring in association with in an ovarian teratoma has been described (5).
We propose a common origin of a nasopharyngeal teratoma and suprasellar heterotopic cerebellum from aberrant pleuripotent stem cells separated into two distinct clusters during embryogenesis. Our patient also had a unilateral choanal atresia as well as an interhemispheric arachnoid cyst, probably as a result of an unexplained embryologic abnormality indirectly related to the masses.
Case Report
A girl was born to a 29-year-old woman after an uneventful pregnancy. Soon after birth, she developed breathing difficulty. The patient had stridor and retraction of the chest wall. During intubation, a large nasopharyngeal mass was noticed. CT done on day 1 of life showed a large mass with fat and calcified densities in the nasopharynx (Fig 1). MR imaging done on day 2 showed a heterogeneous mass in the nasopharynx and a large nonenhancing suprasellar mass that was isointense to gray matter on T1- and T2-weighted sequences (Figs 2 and 3). A normal cerebellum was identified on MR and CT images. A presumptive diagnosis of hypothalamic hamartoma was made. MR imaging also revealed an interhemispheric cyst in the frontal region that corresponded to CSF signal intensity on all pulse sequences. Laboratory tests showed normal serum levels of cortisol, TSH, T3, and αFP.

Contrast-enhanced CT of the neck shows a large, heterogeneous, nasopharyngeal mass with fatty (arrow) and calcified (asterisk) densities compatible with a teratoma.fig 2. Midsagittal T1-weighted (450/12 [TR/TE]) MR image reveals a large well-defined mass in the suprasellar region (arrow) that is isointense to gray matter. An interhemispheric cyst, which is isointense to CSF (white asterisk), is also seen anterior to the suprasellar mass. Another heterogeneous mass with foci of T1 hyperintensities (black asterisk) fills the nasopharynx.fig 3. Coronal fast spin-echo T2-weighted (6000/98 [TR/TEeff]) MR image through the sellar area shows a large mass (black arrow) isointense to gray matter. The optic nerves and chiasm are not recognized because of severe compression and displacement. In the nasopharynx, a mixed signal mass (white arrow) with foci of low and high signal intensity is noted
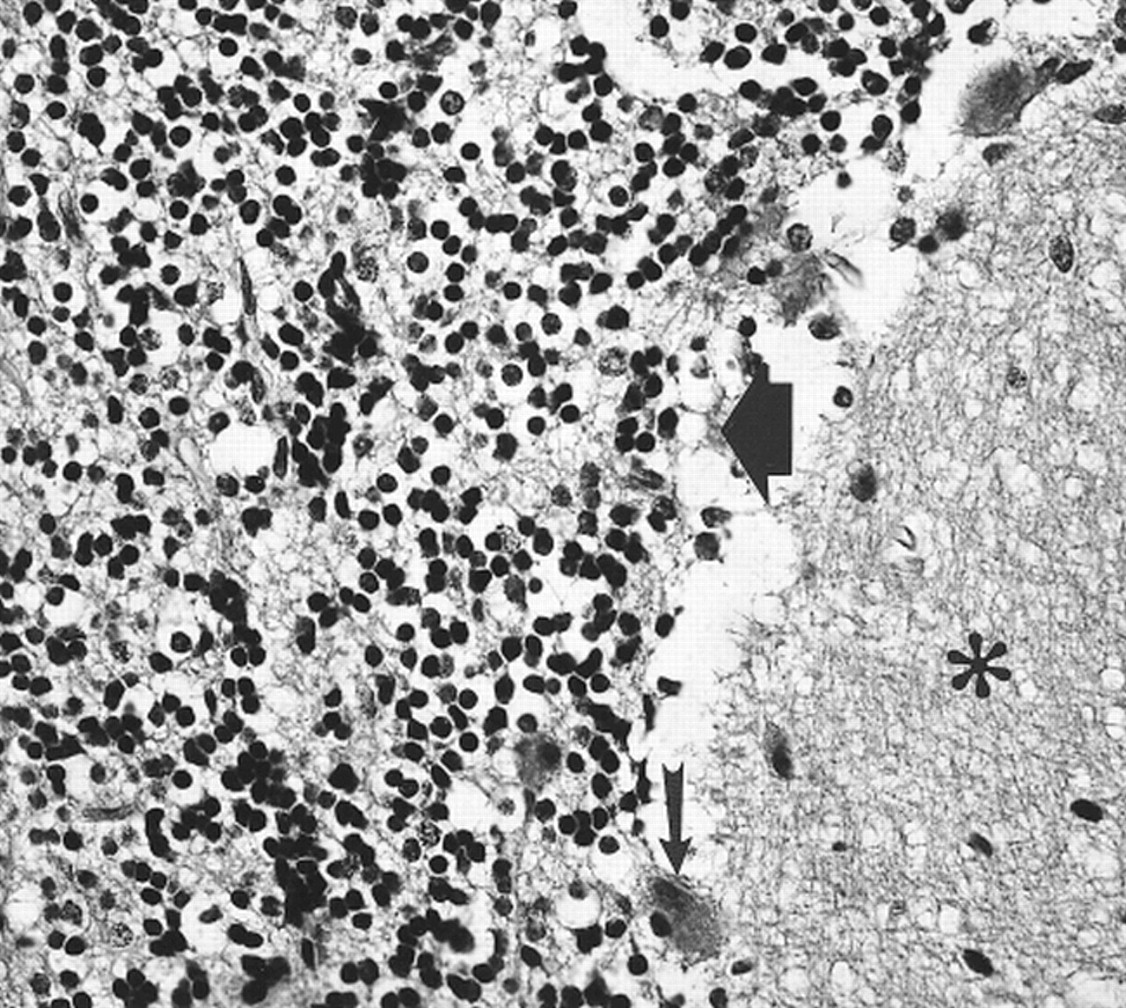
At surgery, a large mass filling the nasopharynx was found. The tumor had a 2-cm stalk attached to the right lateral nasophayrngeal wall. The mass was completely resected and was diagnosed as a mature teratoma based on histopathologic findings. During that admission, no surgical intervention was deemed necessary for the suprasellar mass, because the patient had no symptoms pertaining to the intracranial abnormalities. During a routine follow-up visit 3 months later, optic neuropathy was detected. Follow-up MR imaging revealed no change in the suprasellar mass; however, there was an increase in the size of the interhemispheric cyst. Surgical resection of the interhemispheric cyst and partial debulking of the suprasellar mass followed. Histopathologic analysis of the tissue specimen resected from the suprasellar mass revealed normal cerebellar tissue architecture, consisting of internal and external granular, molecular, and Purkinje cell layers (Fig 4). The thickness of the proliferating external granular layer was appropriate for a 4-month-old child.
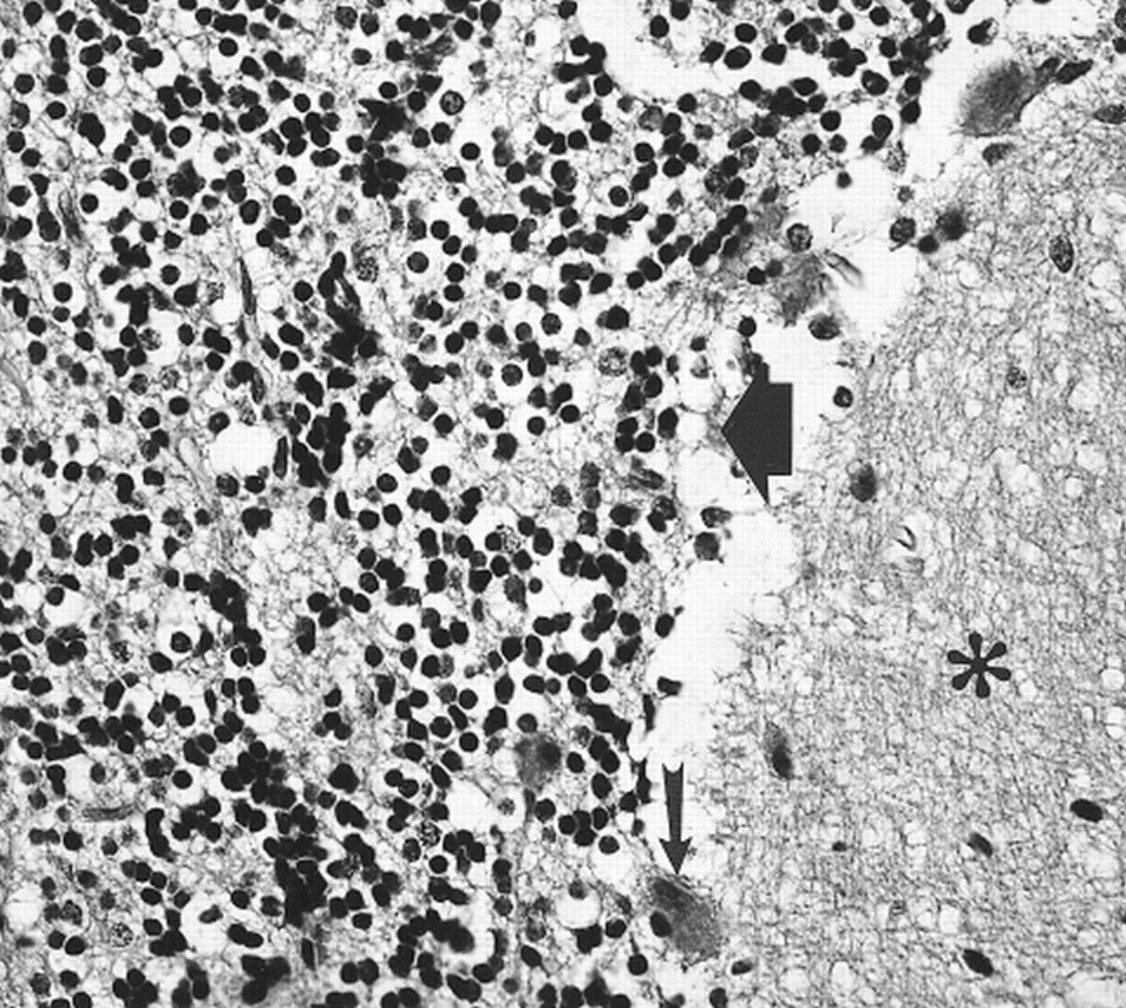
High-power microphotograph of the tissue specimen stained with hematoxylin and eosin shows molecular layer (asterisk) and granular cell layer (large arrow) separated by a monolayer of Purkinje cells (small arrow)
Discussion
Microscopic cerebellar dysplasias are common in the cerebellar white matter, dentate nuclei, nodulus, and cochlear nuclei during the neonatal period (1). These are considered normal variations and usually consist of single or mixed cell layers arranged in a disorganized manner. In contrast, heterotopias consist of tissue or organs found in an abnormal location, and may become symptomatic, depending on their location and size. A heterotopic cerebellum occurring away from its normal location usually exhibits organized, normal, cellular constituents. A heterotopic cerebellum that is found in a location far distant from normal is extremely rare and has been anecdotally reported in the lower cervical and thoracic spine, the orbit, and frontal encephaloceles (2–4). In a report describing a heterotopic cerebellar mass in the lower cervical spine, the authors hypothesized that the process was related to the presence of pleuripotent cells in the accessory elementary canal, which traverse the notochord and neural tube, a mechanism similar to the pathogenesis of split-notochord malformations (6). There are other reports of cerebellar heterotopias in the cervical spine occurring among patients with Chiari malformations (7). In one case report, the presence of heterotopic cerebellar tissue in the orbit was explained by either abnormal germ cell migration or abnormal germ cell differentiation (3).
Our case is perplexing because of the detection of multiple abnormalities, which were found on the midline and on both sides of the skull base. We speculate that the heterotopic cerebellum and nasopharyngeal teratoma developed from imperfect migration of primitive pleuripotent stem cells across the sphenoid bone early during embryogenesis.
Understanding the process of normal pituitary development and associated developmental aberrations may help explain the presence of bilateral masses on the skull base. The anterior part of the pituitary gland develops from ectoderm of the primitive mouth cavity (stomodeum) through Rathke's pouch, which ascends via an opening between the chondrification centers of the presphenoid and basisphenoid bones (8). During normal development, the connection between Rathke's pouch and the stomodeum diminishes. In some cases, however, the path traversed by Rathke's pouch remains patent and is called the basipharyngeal canal. Therefore, during embryogenesis, there are normal channels through which germinal cells are exchanged between the future upper digestive tract and the sellar region. We theorize that separation of pleuripotent cells across the future sphenoid bone occurred through this pathway. Our hypothesis is supported by occasional reports of craniopharyngioma in the nasopharynx and Rathke's pouch cysts in the sellar region.
The presence of heterotopic cerebellar tissue has been described in an ovarian teratoma by Ferrer et al (5). The authors attributed this to the presence of an abnormal germinal focus analogous to one normally seen in alar plates of developing rhombencephalon. This example is relevant to our case, because it suggests the possibility of selective growth of one cell line among many available in a teratoma.
The reason for maturation of pleuripotent cells into different types of masses is poorly understood. Newman et al (9) proposed possible mechanisms of heterotopic brain: 1) preferential growth of one germ cell line of a teratoma into brain tissue; 2) herniation or prior presence of cells resting in aberrant locations during embryogenesis; and 3) true astrocytoma. One or more of these factors may have been responsible for the masses that developed in our patient. We hypothesize that the presence or absence of an intrinsic signaling process is responsible for initiating and controlling preferential differentiation of pleuripotent cells into various forms. Anatomically distinct and isolated normal cerebellum in our case weakens the argument of heterotopic cerebellum being related to migration of germinal cells during formation of the normal cerebellum. Herniation of the germinal tissue through the ependyma into the CSF to distant locations is an attractive postulation; however, the presence of concomitant nasopharyngeal teratoma cannot be attributed to this process alone.
Our case is further complicated by the presence of an arachnoid cyst and unilateral choanal atresia. These, we believe, reflect the predisposition among patients with major congenital malformations to a multitude of other anomalies.
Teratomas are neoplasms containing all three germinal layers. In the head and neck, they arise from the embryonic tissue that breaks off or fails to migrate to its normal destination and is then subjected to defective regional influences. Teratomas are readily visible on CT or MR images and can be identified by the presence of fat and calcification (Fig 1).
The differential diagnosis of a suprasellar mass includes hypothalamic hamartomas and astrocytomas. In contrast to teratomas, hamartomas are nonneoplastic masses composed of parts derived from local tissue. Histologically, hypothalamic hamartomas resemble gray matter. These present in early childhood as well-defined, nonenhancing, suprasellar masses that are isointense to gray matter. Based on this case, we can suggest that there are no characteristic findings on MR or CT images for differentiating a heterotopic cerebellum from a hypothalamic hamartoma. Astrocytomas arising in the hypothalamic region have ill-defined outlines and show inhomogeneous enhancement.
Conclusion
We report a case of a suprasellar mass of heterotopic cerebellar tissue with an associated nasopharyngeal teratoma, both of which, we believe, originated in pleuripotent stem cells detached during embryogenesis.
Footnotes
1 Address reprint requests to Deepak Takhtani, MD, Department of Neuroradiology, 600 N. Wolfe Street, B-108, Houck Basement, Baltimore, MD 21287.
References
- Received September 29, 1999.
- Accepted after revision January 19, 2000.
- Copyright © American Society of Neuroradiology




{kind=link}
{kind=link}