
Abstract
BACKGROUND AND PURPOSE: Esophageal invasion (EI) by head and neck neoplasm has important prognostic and surgical management implications. Our purpose was to determine the accuracy of MR imaging for predicting neoplastic cervical esophageal invasion.
METHODS: MR scans of the neck obtained from 22 patients with periesophageal masses were retrospectively reviewed independently and by consensus by two experienced head and neck radiologists who were unaware of surgical findings. The patients were selected from clinical, radiologic, or pathologic reports suggesting EI. The following imaging criteria for EI were evaluated: effacement of periesophageal fat planes, circumferential mass, paraesophageal lymph nodes, luminal size, wall thickening, increased T2 wall signal, and wall enhancement. There were eight patients with EI and 14 patients without EI, as confirmed by surgical findings or pathologic examination.
RESULTS: The consensus criteria with the best sensitivities were any wall thickening (100%), effaced fat plane (100%), and any T2 wall signal abnormality (100%). The criteria with the best specificities were circumferential mass greater than 270 (100%) or 180 degrees (93%) and focal T2 wall signal abnormality (86%). The overall kappa value for the two readers for all criteria was 0.57 (moderate agreement).
CONCLUSION: A circumferential mass or focal T2 signal abnormality on the esophageal wall suggests the presence of EI. An intact fat plane, absence of wall thickening, and no T2 wall signal abnormalities imply that the esophagus is not invaded.
Direct esophageal invasion is an uncommon but significant sequela of advanced head and neck squamous cell carcinomas, thyroid tumors, and bronchogenic carcinomas.
Direct esophageal invasion in squamous cell carcinoma and bronchogenic carcinoma portends poor patient survival (1–4) (24–27% 5-year survival); however, patients may benefit from surgical resection of the tumor for palliative maintenance of oral alimentation and prevention of airway compromise. In cases of advanced well-differentiated thyroid papillary and follicular carcinoma, the effect of esophageal invasion on patient survival is debated (4, 5), and patients may still benefit from complete resection of the tumor (1–6) with an overall 70% 5-year survival.
Esophageal invasion increases the surgical complexity for tumor removal. Esophageal resection with either gastric pull-up or free jejunal transfer are the two most commonly advocated surgical procedures (1, 2, 6, 7). Both of these procedures require the involvement of three operative fields: neck, thorax, and abdomen. Therefore, determining neoplastic esophageal involvement becomes very important for preoperative surgical planning and coordination of various surgical subspecialties (1, 2, 6, 8). Because esophageal invasion is more often from extrinsic disease (adenopathy or thyroid neoplasm) than from spread of pharyngeal/larygeal disease, endoscopy is of little value in this regard.
The literature assessing the ability to evaluate EI is limited radiologically (9–11). The purpose of this project was to develop MR imaging criteria for the detection of esophageal invasion and determine the accuracy of various criteria.
Methods
Twenty-two patients were identified over a 4-year period (1994–1998) by reviewing reports of MR imaging of the neck that specifically suggested secondary neoplastic involvement of the esophagus, pathologic reports confirming direct esophageal invasion by adjacent neoplasms, and/or retrospective identification of cases from the recall or computerized records search from head and neck surgeons. Eleven patients were women and 11 men, who had a mean age of 63 years (range, 30–81 years).
The determination of the presence or absence of esophageal invasion was made by pathologic evidence from surgical resection or biopsy (n=3), operative findings (n=4), endoscopy, and/or clinical impression (n=1). Eight patients had evidence of esophageal invasion by laryngeal squamous cell carcinoma (n=4), thyroid papillary carcinoma (n=2), tracheal squamous cell carcinoma (n=1), and bronchogenic adenocarcinoma (n=1). Fourteen patients did not have esophageal invasion; they were included because their MR scans were interpreted prospectively as being suspicious for esophageal involvement. EI was excluded by head and neck surgeons during operative evaluation and lack of progression on follow-up scans. These patients had laryngeal squamous cell carcinoma (n=5), thyroid papillary or follicular carcinoma (n=4), benign multinodular goiter (n=1), thyroiditis (n=1), tracheal squamous cell carcinoma (n=1), parathyroid hyperplasia (n=1), and tongue-base squamous cell carcinoma, with extension into the supraglottic larynx (n=1).
All examinations were performed with a 1.5-T scanner using an anteroposterior volume neck coil (Medical Advances, Madison, WI). The images of the neck extended from the level of the cavernous sinus to the thoracic inlet. The MR imaging protocol consisted of standard spin-echo sagittal T1-weighted images (550–750/11–30 [TR/TE]), axial spin-echo T1-weighted images (550–750/11–30), and axial fat-suppressed fast spin-echo T2-weighted images (3500–4000/70–95). Seventeen patients received 0.1 mmol/kg IV gadopentetate dimeglumine, and were imaged with either postcontrast axial fat-suppressed 3D fast multiplanar spoiled gradient-echo (FMPSPGR) (150–250/1–4; flip angle, 90°) or axial fat-suppressed spin-echo T1-weighted sequences (TR/TE range, 550–750/11–30). Axial 3D FMPSPGR images were obtained with contiguous 5-mm sections, 24- to 26-cm fields of view, a matrix size of 256 × 128, and one excitation. Sagittal T1-weighted images were obtained with a slice thickness of 5 mm with no interslice gap, a 30-cm field of view, a matrix size of 256 × 128, and one or two excitations. All other sequences were obtained with contiguous 3- to 5-mm sections (3-mm sections were performed for laryngeal carcinomas), 24- to 26-cm fields of view, a matrix size of 256 × 192, and one or two excitations.
Retrospective image analyses were performed independently by two head and neck radiologists who were unaware of the surgical and pathologic findings during a consensus session. For each case, the available MR images were evaluated for the presence or absence of the following findings with respect to the cervical esophagus: effacement of the adjacent fat plane, paraesophageal adenopathy, and luminal distention. In addition, the following MR imaging criteria were graded for each subject: circumferential mass around esophagus (graded as 0 = less than 180°, 1 = greater than 180° but less than 270°, and 2 = greater than 270°); esophageal wall thickening (0 = no wall thickening, 1 = diffuse wall thickening, and 2 = focal wall thickening); increased wall signal on T2-weighted images compared with skeletal muscle (0 = normal esophageal wall signal intensity approximately equal to skeletal muscle [12], 1 = diffuse increased wall signal, and 2 = focal increased wall signal); and wall enhancement (0 = no wall enhancement, 1 = diffuse wall enhancement, and 2 = focal wall enhancement).
The MR findings were correlated with the pathologic, surgical, endoscopic and clinical findings. The data were analyzed to determine the accuracy, sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) of each imaging criterion. Interobserver agreement regarding image interpretation was based on percent agreement and kappa analysis.
Results
The normal cervical esophagus (Fig 1) shows an intact fat plane and a homogeneously thin wall (less than 5 mm) (13) on MR images, and is isointense to skeletal muscle on T2-weighted imaging (12). The normal esophagus has diffuse enhancement of the mucosa (13). The mucosa of the esophagus is visible on T2-weighted studies (13).
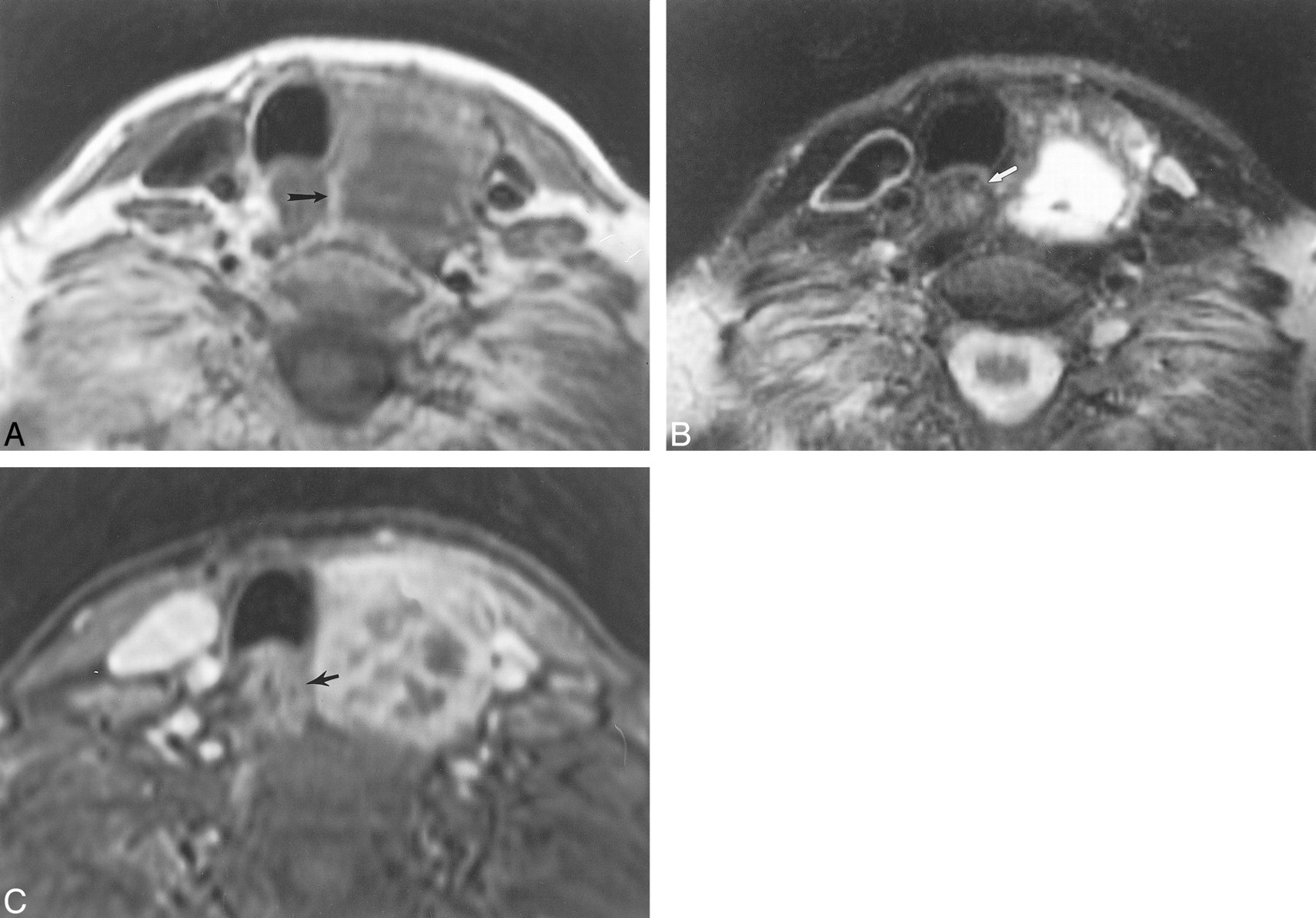
This 68-year-old woman with a benign, left, thyroidal multinodular goiter demonstrates the normal MR imaging appearance of the adjacent esophagus.
A, Axial T1-weighted image (500/16 [TR/TE]) shows an intact fat plane (arrow) between the esophagus and the mass. The thyroid mass is adjacent to the esophagus, and the esophageal lumen is collapsed.
B, Axial T2-weighted image (3500/84) shows normal hypointense signal of the wall musculature of the esophagus (arrow).
C, Axial enhanced 3D FMPSPGR image (220/27; flip angle, 90o) shows mild enhancement of the mucosal lining of the esophageal wall (arrow).
Table 1 lists the MR findings obtained from 22 patients that were evaluated during the consensus interpretation session. Table 2 lists the performance of the individual MR imaging criteria for the evaluation of EI. The criteria evaluated by consensus with the best accuracies for predicting esophageal invasion (Figs 2 and 3) were focal wall signal on T2-weighted images (86%), any (diffuse or focal) wall T2 signal (81%), circumferential mass greater than 180° (77%), and circumferential mass greater than 270° (73%). The consensus criteria with the highest sensitivities and negative predictive values were effaced fat plane (100%), any (diffuse or focal) wall thickening (100%), and any wall signal on T2-weighted images (100%). The consensus criteria with the highest specificities were circumferential mass greater than 270° (100%), circumferential mass greater than 180° (93%), focal wall signal on T2-weighted images (86%), and paraesophageal adenopathy (86%). The following MR criteria had low accuracies (59–61%) owing to low specificities (36–50%): any (diffuse or focal) wall thickening and any wall enhancement. Paraesophageal adenopathy had lower accuracy (59%) owing to low sensitivity (13%).
Findings revealed by MR imaging
Esophageal invasion. Comparison of MR imaging criteria

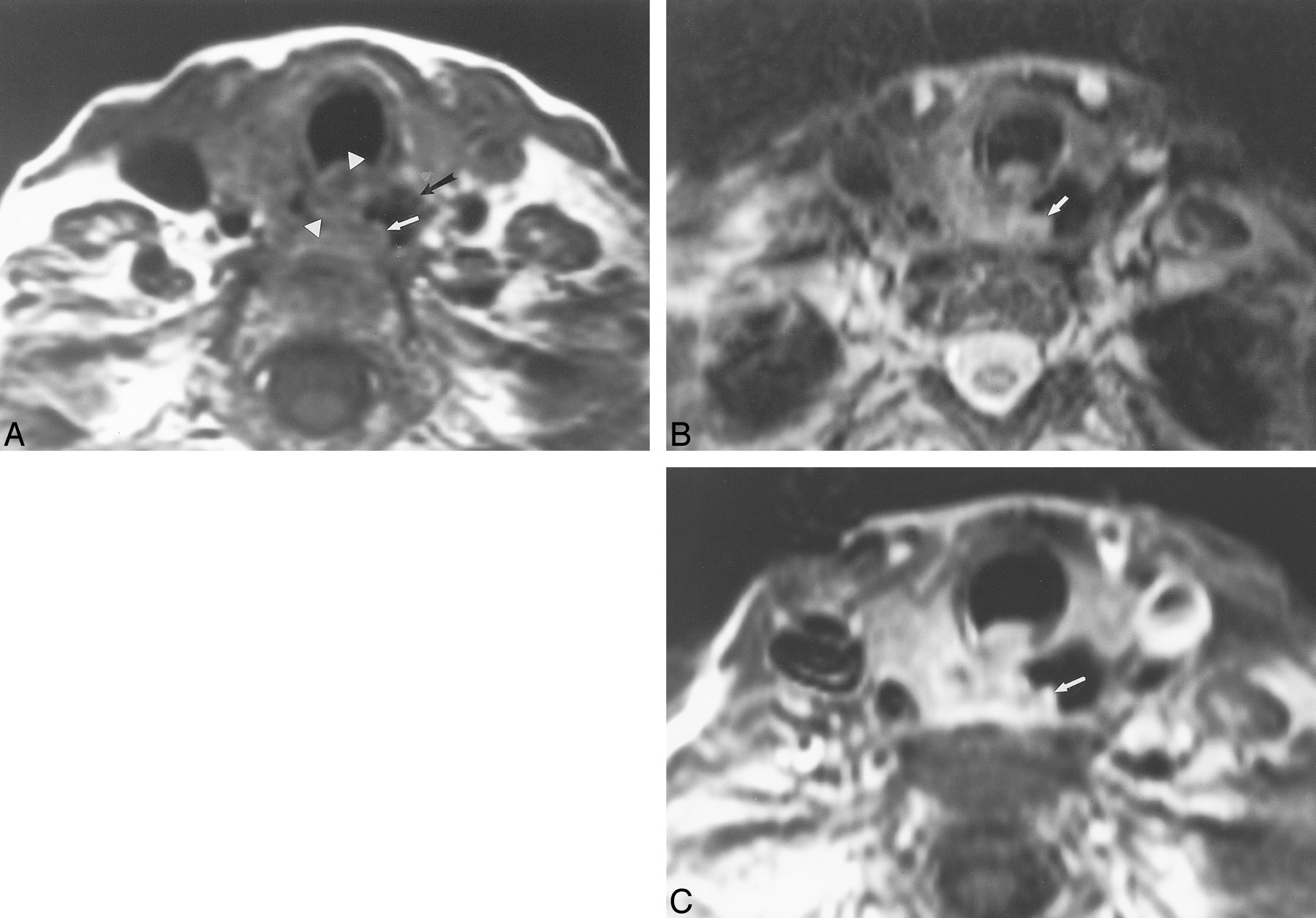
This 62-year-old man with metastatic laryngeal carcinoma to cervical lymph nodes had surgically proven esophageal invasion.
A, Axial T1-weighted image (700/17) shows obliteration of the fat plane between the mass (arrowheads) and the right lateral esophageal wall. There is focal wall thickening of the esophagus (white arrow). The esophageal lumen is distended with air (black arrow). The mass abuts the esophageal wall for less than 180o.
B, Axial T2-weighted image (4000/80) demonstrates increased esophageal wall signal (arrow) adjacent to the mass.
C, Axial enhanced 3D FMPSPGR image (235/21; flip angle, 90o) shows increased enhancement of the esophageal wall (arrow) as well as diffuse enhancement of the adjacent mass.
There was moderate overall interobserver agreement (κ = 0.57) with a 73% agreement in observations for the 22 patients with respect to the three binary MR imaging criteria and the four graded criteria. Individual kappa values for imaging criteria were as follows: circumferential mass greater than 180° (κ = 0.77), effaced fat plane (κ = 0.70), luminal distention (κ = 0.62), and any esophageal wall thickening (κ = 0.48). The remainder of the imaging criteria had kappa values below 0.40.
Discussion
Esophageal metastases have been found to occur in 3% of patients dying of carcinoma in an autopsy series. Most of these cases represent esophageal involvement by direct extension of primary tumor or adjacent adenopathy rather than hematogenous metastases (14). The malignancies associated with EI include thyroid carcinoma, hypopharyngeal carcinoma, laryngeal carcinoma, and bronchogenic carcinoma. Well-differentiated papillary and follicular thyroid carcinomas demonstrate local invasion of surrounding viscera in only 5–15% (15–17). In a study by Czaja and McCaffrey (5), which evaluated locally invasive well-differentiated thyroid carcinoma, there was EI in 21% (60/286) of the cases. In anaplastic thyroid carcinoma, five (26%) of 19 (18) patients overall demonstrated EI. The incidence of EI for hypopharyngeal and laryngeal carcinoma is more difficult to ascertain because, in advanced tumors involving the cervical esophagus, the exact site of origin of the neoplasm may be indeterminate (19). Hypopharyngeal carcinoma does have a propensity to involve the cervical esophagus, as the boundaries between these anatomic regions are artificial and merge with each other (19). In 100 pharyngectomies for hypopharyngeal carcinoma, 23% of the tumors demonstrated inferior extension to the cervical esophagus (20). In a study of T4 non–small cell bronchogenic carcinoma, six of 44 tumors with mediastinal extension demonstrated EI (21).
EI by advanced head and neck or mediastinal tumors may affect patient survival (1–4, 6, 8, 21, 22); however, there may still be benefit for surgical resection of the offending lesion (2, 4, 8, 23). There is some debate in the literature about the consequence of EI for advanced thyroid papillary or follicular carcinoma. The 5-year survival of patients with papillary and follicular cancers is greater than 70% (8). Czaja and McCaffrey (5) found that the reduction in patient survival for invasion of the esophagus was not significant in patients with well-differentiated thyroid carcinoma (P>.1), although, previously, EI was believed to be a significant factor for survival (3, 4, 8). In any case, most authors contend that patient survival with well-differentiated thyroid carcinoma may be improved when there is complete resection of the tumor (4, 5, 8, 23), particularly from the involved portion of the cervical esophagus. In patients with extensive laryngeal and hypopharyngeal squamous cell carcinomas, EI automatically upgrades primary tumor staging to a T4 classification (24) and heralds poor survival (2). The overall 5-year survival for patients with stage IV squamous cell carcinoma of the head and neck is 24–27% (2) and has not significantly changed in the last 25 years. For T4 bronchogenic carcinoma invading the mediastinum and esophagus, the overall 5-year survival is only 7% (22), and complete surgical resection is usually not possible (21). In such advanced cases, accurate determination of EI is essential for effective surgical intervention whether it is an attempt to cure or merely to restore normal oral food intake (2).
Predicting EI is important for planning an appropriate surgical strategy for the treatment of advanced head and neck tumors (1, 2, 6, 8), as reconstructions of the esophagus will need to be planned (7). Once the cervical esophagus is involved, the surgery for complete tumor removal becomes significantly more complex. A thoracic or general surgeon usually becomes involved in the procedure with the head and neck surgeon. At our institution, if the upper cervical esophagus is invaded and can be resected above the mediastinal inlet, the reconstruction requires an interposition of jejunum or other microvascular tubed fasciocutaneous flaps to repair the cervical esophagus and the hypopharynx. If the tumor involves the esophagus below the manubrium, complete removal of the esophagus, removal of a portion of the cervical trachea and sternum, and mediastinal lymph node dissection have to be considered. In this case, a total esophagectomy is performed, followed by gastric pull-up and pharyngogastric anastomosis. Mediastinal anastomoses, such as with colonic interpositions or intestinal grafts, are usually avoided because of the potentially fatal complications of infection or flap loss. Both techniques require extensive planning with involvement of three operative fields: neck, thorax, and abdomen (1, 2, 6, 7). In recent years, the overall morbidity and mortality for performing these extensive esophageal resections and reconstructions has been declining (1, 2, 6, 7). The incidence of major morbidity has declined from 23% to 9% for gastric pull-up and pharyngogastric anastomosis (6), whereas the incidence of major morbidity or mortality for free jejunal interposition grafts occurred in five (12.5%) of 40 patients in one series (25). Thus, in the surgical literature, there have been calls for new diagnostic methods for determining which patients will require radical excision because of EI (8).
The radiologic detection of esophageal invasion by either adjacent neoplasms or adenopathy has been addressed only on a limited basis in the literature. The findings on a barium esophagram of direct invasion of the cervical esophagus include irregular luminal narrowing, eccentric mass effect, nodular or serrated contour, ulceration, and/or obstruction (10, 26). However, the findings on esophagram may be nonspecific for metastatic disease or primary esophageal disease (10, 26). CT of bronchogenic carcinoma with EI may show contralateral displacement of the esophagus, partial obstruction, or a bronchoesophageal or tracheoesophageal fistula (9). CT for the evaluation of anaplastic thyroid carcinoma suggested esophageal involvement in four of five cases of pathologically proven invasion, although specific criteria for determining invasion were not stated (18). In the case of piriform sinus carcinoma, CT has been shown to be better than endoscopy for revealing the inferior limit of tumor relative to the esophagus (27). MR imaging has been used only on a limited basis for evaluation of the esophagus (12, 28–30); we found only one case of EI by metastatic thyroid carcinoma in the recent English-language literature (11).
The accurate evaluation of patients at risk for EI requires specific criteria for defining or excluding tumor invasion of the esophagus. Our results indicate that the following MR imaging criteria can suggest secondary EI: circumferential mass greater than 270° (PPV = 100%), circumferential mass greater than 180° (PPV = 80%), and focal increased esophageal wall signal on T2-weighted images (PPV = 75%). Conversely, the following MR imaging criteria can suggest that the esophagus is uninvolved: intact fat plane (NPV = 100%), no wall thickening (NPV = 100%), and normal wall signal on T2-weighted images (NPV = 100%). Some of the criteria were more useful for determining invasion (accuracy range, 67–86%): focal or any increased wall signal on T2-weighted images, circumferential mass either greater than 270° or 180°, disrupted fat plane, focal wall thickening, and focal wall enhancement. The remaining criteria suffered from low accuracies (55–62%): paraesophageal adenopathy, distended lumen, diffuse wall thickening, diffuse wall enhancement, and diffuse increased wall signal on T2-weighted sequences.
A limitation of the imaging criteria used for evaluating EI is the low kappa values for several MR imaging criteria. There are probably two main reasons for this interobserver variability. First, when the cervical esophagus is surrounded by a complex mass, it is sometimes very difficult to distinguish the esophagus from the mass. On the consensus readings, which were performed after the independent readings, distinguishing the cervical esophagus separate from the adjacent mass was the most important step in assessing for EI. The second reason is that it is usually easier to agree on binary criteria rather than graded criteria. For example, it is easier to characterize any esophageal wall enhancement rather than dividing the enhancement pattern into focal or diffuse.
MR imaging is more accurate at predicting the lack of EI rather than its presence (Fig 4). Perhaps the use of oral contrast for MR imaging (11, 30) may improve specificity for detecting esophageal invasion. Although there is no single perfect MR criterion, the combination of the various criteria with the higher accuracies listed above are recommended for predicting EI. This is important for surgical planning in cases that may require complex esophageal resections and reconstructions.

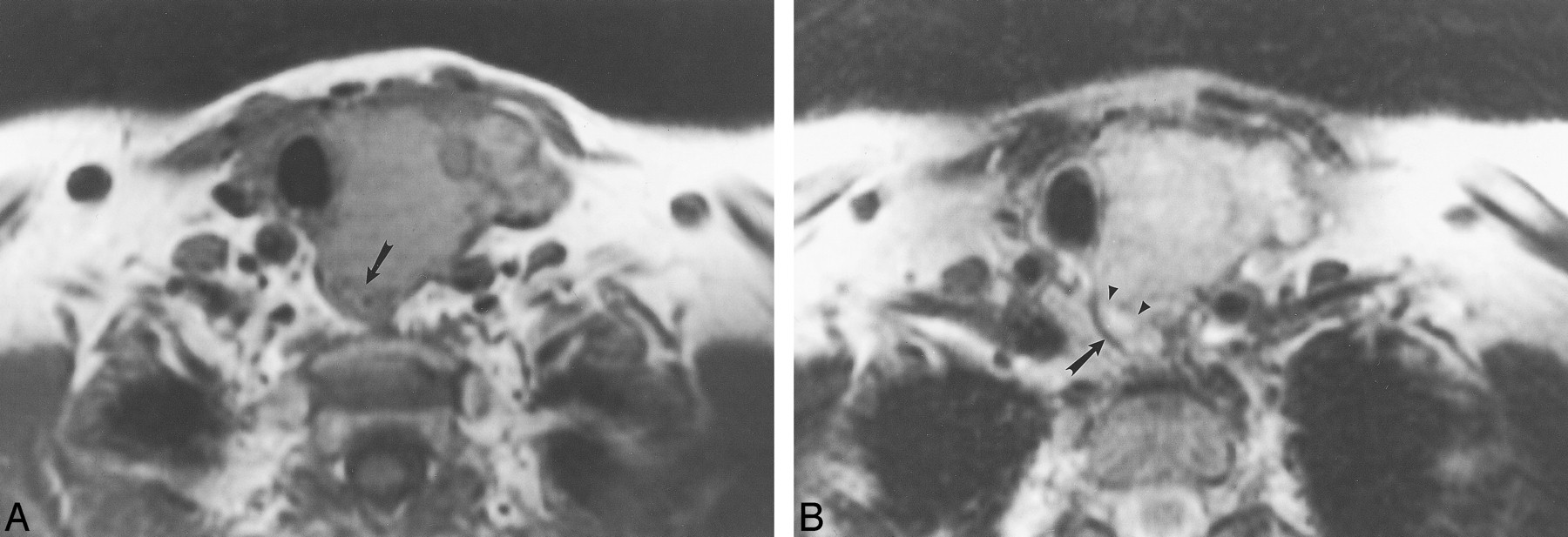
This 66-year-old man had direct EI by laryngeal carcinoma, resulting in a tracheo-esophageal fistula.
A, Axial T1-weighted image (600/17) shows a mass that surrounds the esophagus (arrows) by approximately 270o. The fat plane between the mass and the esophagus is obliterated. The esophageal lumen contains air.
B, Axial T2-weighted image (4000/80) shows focal increased signal (arrow) in the esophageal wall adjacent to the mass.
This 72-year-old woman had follicular carcinoma of the left lobe of the thyroid. This case represents a false-positive interpretation of esophageal invasion. There was no evidence of esophageal invasion by surgical or pathologic evaluation.
A, Axial T1-weighted image (700/17) shows effacement of the fat plane between the esophagus and the left thyroid (arrow).
B, Axial T2-weighted image (3000/78) shows focal increased signal within the esophageal wall adjacent to the thyroid mass (arrowheads) compared with the normal right lateral wall of the esophagus (arrow).
Conclusion
The detection of EI in cases of advanced head and neck neoplasms is important for determining prognosis and for developing a surgical strategy in cases where an esophagectomy may be required for either treatment or palliation. MR imaging findings of a circumferential mass or focal T2 signal abnormality on the esophageal wall suggests the presence of EI. An intact fat plane, absence of wall thickening, and no T2 signal abnormalities on the esophageal wall imply that the esophagus is not invaded. A prospective analysis of EI by use of MR imaging would be important for future investigation.
Footnotes
1 Presented at the annual meeting of the American Society of Neuroradiology, Philadelphia, PA, May 1998, and awarded as best paper in head and neck radiology.
2 Address reprint requests to Laurie Loevner, M.D., Hospital of the University of Pennsylvania, Department of Radiology, Neuroradiology Section, 3400 Spruce Street, Philadelphia, PA 19104.
References
- Received April 28, 1999.
- Accepted after revision April 27, 2000.
- Copyright © American Society of Neuroradiology
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.