
Recent clinical reports have indicated an aneurysm recurrence rate of 15% following Guglielmi detachable coil (GDC) embolization (1). Future research must emphasize the development of biologically active embolization devices, which accelerate endoluminal fibrosis in cerebral aneurysms, to prevent recanalization. While animal studies employing vein pouch aneurysms have consistently revealed complete fibrous organization of endoaneurysmal thrombus within 6 months of GDC embolization, several human investigations have revealed persistence of unorganized thrombus in cerebral aneurysms for as long as 8 months (2–5). This discrepancy has raised serious questions about the validity of the vein pouch aneurysm model in neurointerventional research. Studies have shown that vein pouch aneurysms have similar histologic responses to embolization devices, whether or not the devices are modified with biologically active materials (6). The results may simply reflect the exhuberant fibrous tissue reaction of a healthy surgical wound to implantation of a foreign body. Current research objectives require a valid aneurysm model that can be easily reproduced.
Although the elastase infusion model does not approximate the pathophysiology of cerebral aneurysms in humans, neither does the vein pouch aneurysm model. Physiologic aneurysm models have been described by Hashimoto et al (7); however, these models are not practical for the study of endovascular occlusion devices. The rat model consists of vessels, and aneurysms too small to permit endovascular embolization. The primate model is impractical as a result of the long latency period for aneurysm formation (1 year). In addition, both of Hashimoto's models are inefficient, resulting in aneurysm formation in only 10–40% of animals.
Stehbens doubts that aneurysmal arterial lesions can be created with elastase. Numerous investigators have reported the formation of aneurysms following elastase digestion of the arterial wall (8–11). Although Cawley et al did not use controls to assess the effects of elastase and exclude the possibility of traumatic artifact, the controlled series of experiments recently conducted by Cloft et al (9, 11) should dispel any notion that the morphologic and histologic changes produced by elastase infusion represent a form of artifact.
Although, Stehbens contends that “fashioning an aneurysmal sac” as a “lateral, berry, or fusiform aneurysm reproduces the hemodynamic condition found in humans,” laboratory studies conducted by Strother et al (12) have proven otherwise. In experimental terminal and bifurcation aneurysms, Strother et al found rapid flow, without vortex formation or endosaccular stasis. In contrast, they found central vortex formation with prolonged endosaccular stasis, lasting up to several minutes, in side-wall aneurysms. Kerber et al (13) illustrated how the orientation of the aneurysmal ostia to slipstream vectors in the parent artery determine whether or not an incompletely occluded aneurysm will continue to grow and rupture. Graves et al (14) have shown that hemodynamic forces strongly affect the compaction and migration of embolic agents in the sac of experimental aneurysms. The technical success of embolization in a side-wall model cannot be extrapolated to the clinical setting because the hemodynamic vectors that effect coil migration, coil compaction, persistent flow into incompletely occluded sacs, and formation of thromboemboli are disparate.
We did not allege that Stehbens denied enlargement of vein pouch aneurysms. We did indicate that his reports of enlargement contradicted the findings of other investigators (8). Although Stehbens claims that he observed progressive enlargement of vein pouch aneurysms, he never performed serial angiography (15–17). Others have failed to demonstrate expansion of vein pouch aneurysms when serial angiography was performed (18).
A major difference between human cerebral aneurysms and vein pouch aneurysms that cannot be easily reconciled is the vast difference in saccular structure. Human cerebral aneurysms are thin walled, acellular structures (Fig 1A and B). Although Stehbens argues that the morphologic measurements of human aneurysms we reported are erroneous, our measurements agree closely with those published by Suzuki and O'Hara (19) in their study of 45 human cerebral aneurysms. Although it is true that the walls of some aneurysms thicken as the sac undergoes expansion, and mural tears develop, leading to the intramural deposition of fibrin and foci of intimal hyperplasia, most cerebral aneurysms possess strikingly acellular sacs (19, 20). Stehbens (21) has previously reported that “larger and presumably older sacs usually had relatively acellular walls”. It is misleading to suggest that intimal hyperplasia within aneurysms is “characteristic.” In striking contrast, the walls of vein pouch aneurysms are uniformly cellular (Fig 2A and B). When comparing vein pouch aneurysms to human cerebral aneurysms, it is particularly troublesome that 27% of the vein pouch aneurysms in one series reported by Stehbens underwent osseous metaplasia (17).

Longitudinal cross section of the wall of a human cerebral aneurysm (hematoxylin and eosin).
A, Original magnification ×20.
B, Original magnification ×40.
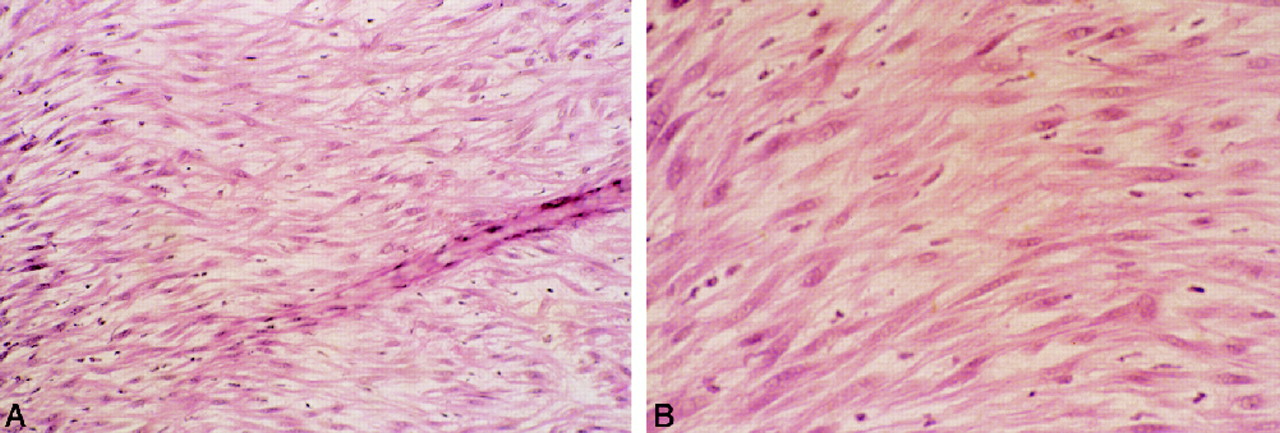
Longitudinal cross section of the wall of a swine vein pouch aneurysm (hematoxylin and eosin).
A, Original magnification ×20.
B, Original magnification ×40.
Stehbens denies stating that intimal proliferation develops in vein pouch aneurysms within 2 weeks. However, he has previously published that “within 2 weeks, there was considerable intimal thickening of the sac wall with stellate cells and abundant intercellular matrix as if edematous” (15). Furthermore, according to his own observations, vein pouch aneurysms developed “hypertrophy of medial bundles of muscle” within 2 weeks of grafting (15). Stehbens also wrote that within 11 days “intimal thickening was present in both venous and arterial segments of the aneurysm” (17). Other investigators have reported that intimal hyperplasia in vein grafts develops as early as 3–5 days after grafting, and increases rapidly during the first 7 days (22).
Regarding the criticism that interspecies comparison of pathologic models is without meaning, we would like Stehbens to consider that all animal models of disease are developed for comparison to the human condition. We have selected rabbits as the species for our elastase aneurysm model because the carotid artery approximates the size of the human middle cerebral artery, enabling a more realistic assessment of microcatheter interventions. We employed the swine vein pouch aneurysm in our study because it has become entrenched in the literature as the favored model. We believe that creation of vein pouch aneurysms in rabbits is more difficult and less reliable. In a rabbit model of vein pouch aneurysms, Spetzger et al reported a 24% operative mortality, a 24% technical failure rate secondary to thrombosis of the parent artery, and procedure times routinely exceeding 3 hours (18). Currently, in our laboratory, rabbit carotid artery aneurysms are created in less than 60 minutes by using elastase infusion, with uniform technical success and minimal mortality.
Stehbens points out that our recent comparison of experimental aneurysms to human intracranial aneurysms was without controls. We hope that our readers understand the difference between a comparative study and a controlled scientific experiment, and appreciate that each is a form of scientific inquiry. Stehbens suggests that the human aneurysm depicted in Figure 5 of our recent report could not have ruptured “recently,” since it contained organizing thrombus near the rupture site. However, organization of the thrombus that seals the site of rupture in human cerebral aneurysms is completed within 3 weeks (19). Stehbens confuses the meaning of angiographic patency by criticizing our reporting of “excellent patency” as being inconsistent with our microscopic findings (8). We have used the terms thrombus and clot to describe the material in the lumina of vein pouch aneurysms, since the material has features of both. We stand by our study design and results. We would like to apologize for any spelling errors and paraphrases that may have been perceived as misquotes.
References
- Copyright © American Society of Neuroradiology
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.