
Abstract
BACKGROUND AND PURPOSE: Decreases in N-acetyl aspartate (NAA) as seen by proton MR spectroscopy are found in hippocampal sclerosis, and elevated levels of lipids/lactate have been observed after electroconvulsive therapy. Our purpose was to determine whether increased levels of lipids/lactate are found in patients with acute seizures of hippocampal origin.
METHODS: Seventeen patients with known temporal lobe epilepsy underwent proton MR spectroscopy of the mesial temporal lobes within 24 hours of their last seizure. Four of them were restudied when they were seizure-free. Five healthy individuals were used as control subjects. All MR spectroscopy studies were obtained using a single-voxel technique with TEs of 135 and 270. The relationship between the presence of lipids/lactate and seizures was tested using Fisher's exact test. Mean and standard deviations for NAA/creatine (Cr) were obtained in the hippocampi in patients with seizures on initial and follow-up studies and these values were compared with those in the control subjects.
RESULTS: Seizure lateralization was obtained in 15 patients. Of the 17 seizure locations that involved hippocampi, 16 showed lipids/lactate by proton MR spectroscopy. Of the 13 hippocampi not directly affected by seizures, 10 showed no lipids/lactate and three showed lipids/lactate. The relationship between lipids/lactate and seizure location was confirmed. A comparison of NAA/Cr ratios for the involved hippocampi with those in control subjects showed significant differences on initial MR spectroscopy; however, no significant difference was found between acute and follow-up NAA/Cr ratios in hippocampi affected by seizures.
CONCLUSION: Lipids/lactate were present in the hippocampi of patients with acute seizures and decreased when the patients were seizure-free. Thus, lipids/lactate may be a sensitive marker for acute temporal lobe seizures.
Proton MR spectroscopy has been shown to be useful in the preoperative evaluation of patients with temporal lobe seizures (1–3). Specifically, proton MR spectroscopy may help to identify the epileptogenic hippocampi by showing low levels of N-acetyl aspartate (NAA). The utility and features of proton MR spectroscopy in the evaluation of patients with acute temporal lobe seizures has not been addressed. It is known that patients undergoing electroconvulsive therapy (which induces seizures) may show significant elevation of lipids/lactate on cerebral MR spectroscopy studies (4). In addition, blood-flow studies, such as 99mTc-HMPAO single-photon emission CT (SPECT), show high uptake in the affected temporal lobe when patients are studied during or immediately after a seizure. Our purpose was to determine whether increased levels of lipids/lactate are found in patients with acute seizures of temporal lobe origin.
Methods
Seventeen patients, 35 to 64 years old (mean age, 42 years), who were known to have refractory partial complex seizures of temporal lobe origin underwent proton MR spectroscopy within 24 hours of their last seizure. All patients were taking antiseizure medications and were outpatients (no patients from the epilepsy monitoring unit were included in this study as they were usually taken off medication for diagnostic purposes). Four patients also underwent follow-up proton MR spectroscopy 2 to 12 months after the first study and were seizure-free at the time of the follow-up examination. Five healthy volunteers, 35 to 55 years old (mean age, 40 years), were studied as control subjects. (The number of control subjects used was limited owing to restrictions imposed by our Institutional Review Board.) All patients had previously undergone one or more MR imaging studies with high-resolution sections of the temporal lobes, and, in combination with clinical, electroencephalographic (EEG) data, and video EEG monitoring, lateralization as to the epileptogenic hippocampus had been established in 15 patients.
All MR spectroscopic data used in this investigation were obtained during a 4-year period (1997–2000) on 1.5-T MR units using a single-volume technique with voxels that included the amygdala/head of the hippocampi. The voxels, which measured 1 × 1 × 1 cm to 2 × 2 × 2 cm, were located away from the fat at the base of the skull to avoid potential lipid contamination. It has been shown that by using a technique identical to the one we used, no significant fat contamination occurs, even when the voxel is placed in proximity to the base of the skull (5). After water suppression, a point-resolved spectroscopy (PRESS) technique was used for localization and the studies were obtained with parameters of 1500/135,270/128 (TR/TE/excitations). The data were postprocessed and choline (Cho) was assigned at 3.2 ppm, creatine (Cr) at 3.03 ppm, and NAA at 2.0 ppm. Lipids/lactate were assumed to be present when a broad peak above the baseline extended from 0.7 to 1.8 ppm (centered at 1.2 ppm) on the longer TE studies. Lactate was assumed to be present when an inverted (below the baseline) peak having a doublet configuration and centered at 1.32 ppm was seen on the studies with TE = 135. When lipids/lactate were identified, the patients were questioned as to the time of their last seizure. The spectroscopic data were reviewed by two observers, and the curve-fitting program provided by the MR unit manufacturer was used to measure peak areas. Owing to differences in techniques (as the patients were studied over a relatively long period of time), peak areas were obtained in 11 patients (65%) and in the five control subjects. Peak areas were not obtained in six patients. In all patients, the two observers determined the presence or absence of lipids and/or lactate. NAA was measured, because it is known to be a putative neuronal marker and is decreased in the presence of hippocampal sclerosis (1–3). NAA was normalized to the Cr peak, as this metabolite is known to remain stable in most brain disorders. In the six patients in whom no peak areas were obtained, the same two observers documented only the presence or absence of lipids/lactate. We compared the mean NAA/Cr ratios for the group of hippocampi affected by seizures with a group of healthy control subjects using Student's t test. The relationship of the presence of lipids/lactate in hippocampi with seizures compared with absence of lipids/lactate in hippocampi unaffected by seizures was analyzed using Fisher's exact test.
Results
Visual inspection of the proton MR spectroscopy studies (total, 72 voxels) showed lipids/lactate in all 17 patients, each of whom had seizures within 24 hours of the MR spectroscopy studies (Fig 1). Despite prior hippocampal lateralization by MR imaging and clinical parameters, six patients showed bilateral abnormalities even when the previous imaging findings suggested only a unilaterally abnormal hippocampus. Lactate (seen at TE = 135) was present in seven patients (right side, 2; left side, 2; bilateral, 3). Lipids/lactate were present in 11 patients (right side, 4; left side, 5; bilateral, 2) (Fig 2). In 11 patients with unilateral lipids or lactate, their location matched the hippocampus presumed clinically to be the seizure focus. In the six patients with bilateral MR spectroscopy abnormalities, the degree of the abnormality did not reflect the side of involvement. Table 1 provides a summary of the clinical and MR spectroscopic data in all patients. Neither lipids nor lactate was seen in any of the control subjects or in the four patients who underwent follow-up MR studies (Fig 3).
Clinical and MR spectroscopic data in patients with hippocampal lactate and acute seizures

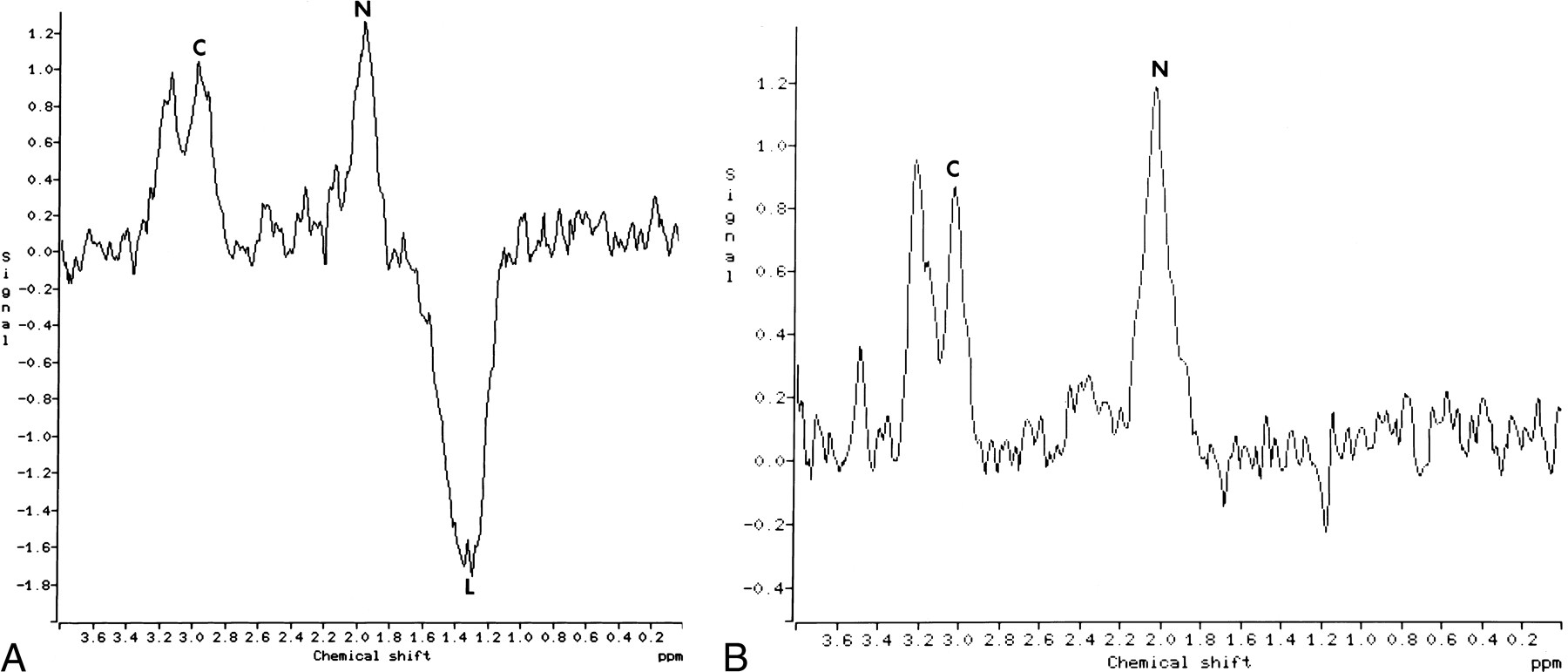
Proton MR spectroscopy in a patient with left hippocampal seizures and lactate.
A, Single-voxel MR spectrum (TE = 135) of the abnormal left hippocampus shows inverted peak with doublet configuration, corresponding to lactate (L). The relationship between NAA (N) and Cr (C) is normal. The NAA peak is normally lower in the hippocampi as compared with gray matter elsewhere.
B, Single-voxel MR spectrum of the right hippocampus shows no lactate.

Proton MR spectroscopy in a patient with left hippocampal seizures and lipids/lactate. Single-voxel MR spectrum (TE = 135) shows mildly decreased NAA and the presence of lipids/lactate (LIP). The right hippocampus was normal

Initial and follow-up proton MR spectroscopy in a patient with left hippocampal seizures.
A, Single-voxel MR spectrum (TE = 135) shows inverted doublet of lactate (L). The level of NAA (N) is normal.
B, The right hippocampus shows no lipids/lactate and a normal relationship between NAA (N) and Cr (C).
C, Study obtained 4 months after initial examination, with patient seizure-free, shows no significant lipids/lactate in the left hippocampus. Relative to the contralateral hippocampus, the level of NAA is slightly decreased with respect to Cr and Cho.
D, MR spectrum shows the right hippocampus to be normal.
MR spectroscopy showed evidence of lipids/lactate in one or both hippocampi in 17 patients. Eight of these patients had seizures lateralized to the left hippocampus, five had seizures lateralized to the right, two had bilateral seizures, and in two patients the seizure location was not determined. These last two patients were not used in this analysis. Hippocampi affected by seizures (17 total) were compared with hippocampi not directly affected by seizures (13 total) for the presence of lipids/lactate. A contingency table was built comparing the presence or absence of seizures affecting individual hippocampi with the presence or absence of lipids/lactate on proton MR spectroscopy (Table 2). Of 17 hippocampi affected by seizures, 16 had evidence of lipids/lactate on proton MR spectroscopy; one did not. Of 13 hippocampi not directly affected by seizures, only three had evidence of lipids/lactate, 10 had no evidence of lipids/lactate. The relationship of the presence of lipids/lactate in hippocampi with seizures compared with absence of lactate in hippocampi unaffected by seizures was confirmed using Fisher's exact test (P < .01). Video EEG monitoring, obtained at a different time from the MR spectroscopy, showed that in five of 17 patients the seizures originated in one temporal lobe but became generalized (tonic clonic).
2 × 2 contingency table shows relationship between presence of lipids/lactate in hippocampi with seizure and absence of lactate in hippocampi unaffected by seizures
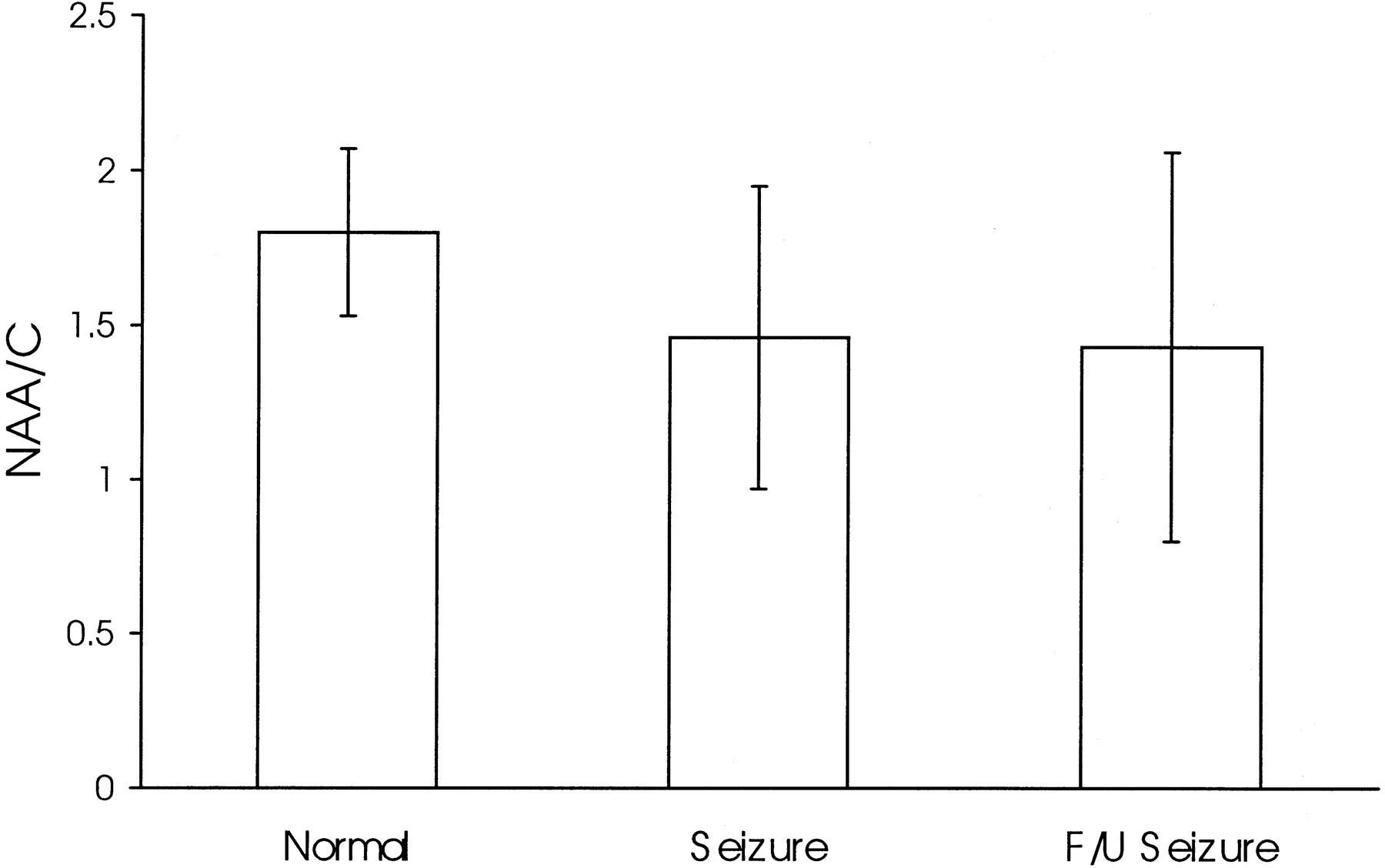
Of the patients with evidence of lipids/lactate, quantitative proton MR spectroscopy results were available in 11. Four of these patients had follow-up examinations. The NAA/Cr ratios for the group of hippocampi affected by seizures (mean, 1.46 ± 0.48; n = 12) were significantly lower than those in the group of healthy control subjects (mean, 1.80 ± 0.27; n = 10). No significant difference was found between acute and follow-up NAA/Cr ratios in hippocampi affected by seizures (mean follow-up NAA/Cr, 1.42 ± 0.64; n = 4) (Fig 4).

NAA/Cr ratios for hippocampi in healthy control subjects (Normal) and in patients with seizures at initial (Seizure) and follow-up (F/U Seizure) examinations
Discussion
Proton MR spectroscopy has been used to examine patients with hippocampal epilepsy (1–3). Most reported studies were performed using a single voxel and long TEs (similar to the technique we used). In the affected hippocampus, proton MR spectroscopy may show decreases of NAA between 15% and 31% as compared with the unaffected hippocampus (6). Accordingly, proton MR spectroscopy may correctly lateralize hippocampal epilepsy in more than 90% of patients (6). The low NAA in the diseased hippocampus appears to reflect the decreased number of neurons in hippocampal sclerosis (1–3). This observation was confirmed in our patients, who showed a significant decrease in NAA/Cr as compared with the control subjects.
Proton MR spectroscopy may also have a greater sensitivity in the detection of bilateral disease than any other noninvasive imaging technique (6). In some studies, 50% of patients had abnormal proton MR spectra on the side contralateral to a sclerotic hippocampus (6). Thus, it seems that proton MR spectroscopy is helpful in the lateralization of a diseased hippocampus and in the identification of bilateral disease; its role in regard to active seizures has not been established.
Small amounts of cerebral lactate may be seen by proton MR spectroscopy in infants immediately after birth (7). Large amounts of lactate or its presence beyond the first few days of life is abnormal and may indicate brain injury. Cerebral lipids are not normally observed at any age, and when present may be the result of contamination from fat residing in or close to the volume of tissue sampled (7). With the use of an MR unit identical to the one in this study and a PRESS localization sequence with long TEs, lipid contamination of voxels abutting fat-containing structures is insignificant (5).
We found that all patients who were imaged within 24 hours of their last seizure episode had lipids and/or lactate in one or both hippocampi. This was not the case among the limited number of healthy control subjects. For this study we only imaged patients with active seizures and therefore cannot comment about the occurrence of lipids/lactate in patients whose seizures are under adequate control. Four of our patients who underwent follow-up studies in a seizure-free state did, however, show no lipids or lactate. We found a strong relationship between the involved hippocampi and the presence of lipids/lactate. Only a few other reports of patients with hippocampal seizures mention the presence of lipids/lactate (3). From our observations, it seems that lipids/lactate are temporally related to seizure occurrence and may be a marker for acute seizures. The time course and significance of lipid/lactate decay remain to be determined, but one study suggests that these metabolites may persist for as long as 7 hours postictally (8).
Lipids/lactate have been observed with proton MR spectroscopy in subjects treated with electroconvulsive therapy and in at least one patient with temporal lobe epilepsy off medications (4). In the latter patient, the lipid/lactate resonances disappeared after repeat medication. Lipid/lactate resonances in patients treated with electroconvulsive therapy diminished within 32 hours but, in some cases, did not return to baseline. The lipids/lactate were generally bilateral, but larger peaks were seen on the stimulated side. Lipids may be produced by increased blood flow and leakage of serum triglycerides into the affected brain regions or they may result from the effects of electrical current on membrane fluidity, resulting in increased visibility on proton MR spectra (4). In addition, a breakdown of neurotransmitters, such as phosphatidylinositol, may induce the release of free fatty acids (arachidonic acid and diacylglycerol), which are visible on proton MR spectra (4). We found that lipids/lactate were present in three hippocampi unaffected by seizures. The presence of lipids/lactate in regions of the brain distal to the original epilepsy focus may be due to the propagation of seizure activity in the brain. Elevated fatty acid levels in turn lead to an increase in intracellular potassium and this may contribute to the spread of activity by depolarization of the presynaptic terminals. It is unclear whether a correlation exists between the presence of MR spectroscopy-visible lipids/lactate and outcome in patients with seizures. In the shaken baby syndrome, the presence of lipids/lactate is probably related to neuronal membrane damage and solubilization of phospholipids and ischemia (9). The release of acid hydrolase and phospholipase contributes to the visibility of lipids on MR spectra and accompanies neuronal damage.
Brain lactate may be detected by proton MR spectroscopy in several brain diseases. Lactate is seen in patients with acute infarctions and mitochondrial encephalopathies (10). Tissue necrosis, such as seen in tumors, also contains lactate. Lactate reflects a conversion from aerobic to anaerobic metabolism due to ischemia and failure of oxidative brain metabolism (10). In children, brain lactate as seen by proton MR spectroscopy implies a poor prognosis, regardless of the underlying cause, and most of these patients are likely to die or develop serious long-term disabilities (9). It is thus possible that the presence of lactate in a hippocampus after seizures represents the end-product of ischemia. In some patients, elevation of lactate may conversely reflect acceleration of glycolysis with accumulation of lactate rather than simple ischemia (10, 11). This has been noted in some tumors and in tissues recovering from hypoxia. In addition, fatty acids are known to inhibit pyruvate dehydrogenase and this also leads to conversion of pyruvate via lactic acid dehydrogenase into lactate.
Caveats of our study include the lack of correlation between the duration of the seizure and its relationship to the levels of lipids/lactate. We did not quantitate the levels of lipids/lactate but simply studied their presence or absence. Because we only questioned the patients regarding seizure activity within 24 hours of the MR spectroscopy study, we do not know how early lipids may by seen with acute seizures. We believe that our observations are valid only for seizures originating and remaining in the temporal lobes. Generalized spread of seizure activity may lead to abnormalities elsewhere in the brain, and MR spectroscopy may lose its value in lateralization. MR spectroscopy also provides information regarding brain areas involved throughout the seizure, unlike with other imaging techniques (such as ictal SPECT), in which a “snapshot” of cerebral blood flow at the time of the seizure is obtained. Mapping of seizure activity with MR spectroscopy necessitates that a patient be studied during or immediately after the seizure and that multivolume techniques be used to assess the extent of the metabolic changes induced by seizures.
Conclusion
We have shown that proton MR spectroscopy in patients with temporal lobe epilepsy obtained within 24 hours of seizure activity shows the presence of lipids and/or lactate in the hippocampi. When lipids/lactate were found in only one temporal lobe, no false lateralizations occurred. Thus, in the period immediately after ictus the presence of lipids/lactate is helpful in lateralizing seizure activity. Significant differences in the levels of NAA/Cr were found in these patients as compared with the control subjects. In a limited number of patients, we found that lipids/lactate disappear once the seizures are under control.
Footnotes
↵1 Address reprint requests to Mauricio Castillo, MD.
- Received April 5, 2000.
- Copyright © American Society of Neuroradiology




{kind=link}
{kind=link}
{kind=link}
{kind=link}