
Abstract
BACKGROUND AND PURPOSE: The purpose of this study was to determine the safety and reliability of the mechanical detachment system of a new platinum coil, Detach-18, when used as a vascular occlusive device for neurovascular disease.
METHODS: Forty-one patients (nine male and 32 female patients; age range, 26–75 years; mean age, 54.4 years) underwent treatment at seven centers. Twenty-two patients had dural arteriovenous fistulae of the transverse sinus treated by a transvenous route. Fourteen patients underwent internal carotid artery occlusion in the treatment of aneurysms, meningioma, facial tumor, or carotid injury. One patient underwent occlusion of the basilar artery and one patient underwent occlusion of the vertebral artery for treatment of aneurysms. In two patients, coils were used as part of the treatment of their arteriovenous malformations. In all cases, the Detach-18 coils were delivered through a microcatheter with two distal markers. Two types of coils, a 0.015-inch-diameter “regular” coil and a 0.014-inch-diameter “soft” coil, were used.
RESULTS: A total of 569 coils were used, 541 of which were detached. The number of coils in ranged from four to 53 (average number of coils, 14). The coils passed easily through the microcatheter. The detachment maneuver occurred within 10 to 25 s with 20 turns of the introducing wire. No premature coil detachment occurred. Complete occlusion of the vessel lumen was achieved in 35 cases. In three cases, 80% to 90% occlusion was achieved. In two cases, 70% to 80% occlusion was achieved. There were no device-related complications.
CONCLUSION: The detachment system was safe, reliable, consistent, and fast. This is a useful system for coil embolization in neurovascular applications.
The use of coils in interventional neuroradiology is now an accepted treatment alternative to surgery in the treatment of many neurovascular pathologic abnormalities (1–10). Endovascular techniques have become the treatment of choice for some intracranial vascular pathologic abnormalities such as basilar tip aneurysms. Although there are several detachable coil systems presently available to treat vascular disease, only the Guglielmi detachable coil system (Target Therapeutics, Inc., Freemont, CA) (11–14) is widely used because of its deployment and retrieval reliability. This system uses electrolysis to separate a coil from the pusher wire. However, as more coils are placed, the time for electrolytic detachment becomes progressively prolonged. The alternative detachable coil systems currently available are mechanical and detach as soon as the junction (the detachment zone) between the coil and the pusher wire protrudes beyond the microcatheter tip (15–20). This makes premature detachment a significant risk, and coil repositioning can be problematic. All currently available detachment mechanisms require that the detachment zone protrude beyond the microcatheter tip. This can result in vessel trauma as the hard pusher wire protrudes into the vascular lumen during and after detachment.
In conjunction with the University of Geneva, William Cook Europe A/S (Bjæverskov, Denmark) developed a mechanically detachable platinum coil system called the Detach-18 system that does not require the pusher wire to protrude beyond the microcatheter tip during detachment. The purpose of our study was to obtain experience with the detachment system and to determine the safety and reliability of coil detachment when used as a vascular occlusive device for neuroradiology applications. We report the clinical experience in a multicenter European trial of this coil.
Methods
Forty-one patients (nine male and 32 female patients; age range, 26–75 years; average age, 54.4 years) underwent treatment at seven European academic medical centers during a 12-month period. Twenty-two patients had dural arteriovenous fistulae (AVF) (Fig 1). These were treated by conventional retrograde cannulation and coil packing of the transverse sinus. Fourteen patients underwent internal carotid artery occlusion for the treatment of aneurysms (Fig 2), a meningioma, a facial tumor, and a carotid injury. One patient underwent occlusion of the basilar artery for treatment of an aneurysm, and one patient underwent occlusion of the intracranial vertebral artery for treatment of an aneurysm. In two patients, coils were used as part of the treatment of arteriovenous malformations.

Images from the case of a 60-year-old man who presented with seizures and a history of a left-sided bruit.
A, Left transverse sinus/sigmoid region dural AVF fed by internal and external carotid artery branches can be seen. The patient underwent a transvenous embolization with Detach-18 coils. Six Detach-18 6 mm × 30 cm coils were deployed via a transtorcular route.
B, Control angiogram of the left vertebral artery shows AVF occlusion.
C, Control angiogram of the left common carotid artery shows AVF occlusion.
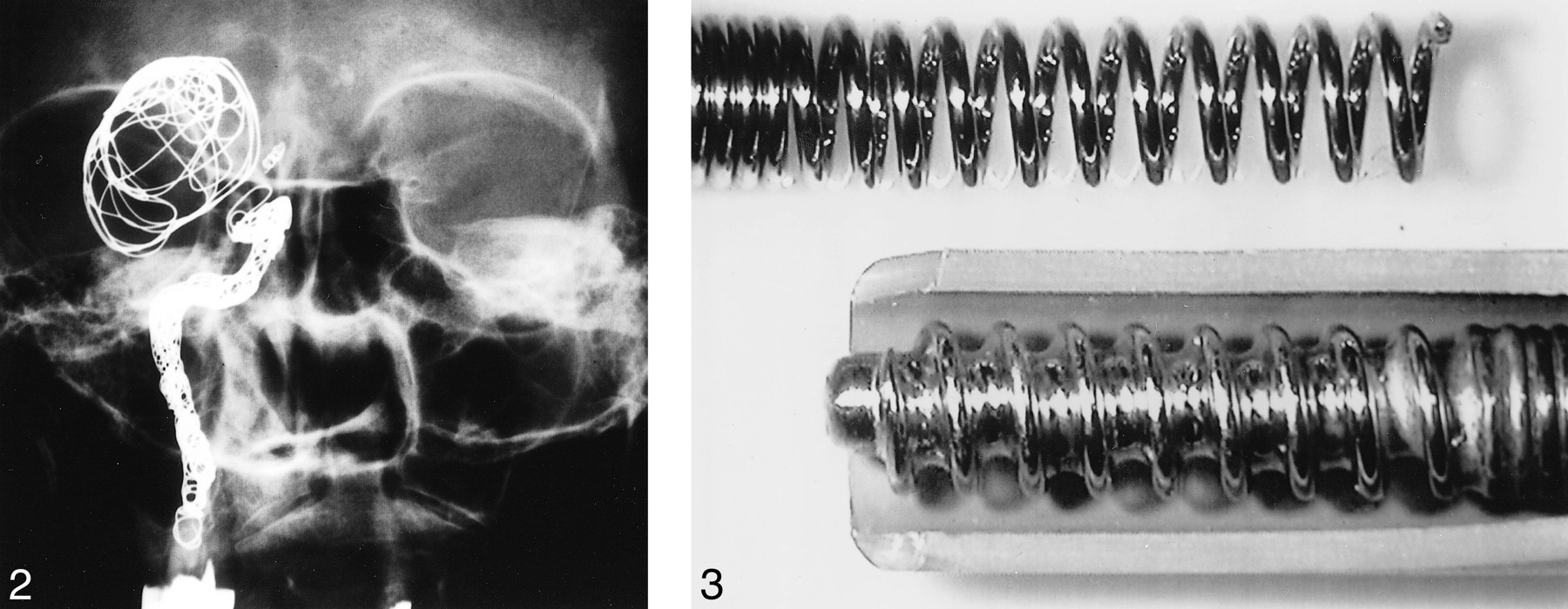
Images from the case of a 65-year-old woman who presented with headache and was found to have a giant C1 internal carotid artery region aneurysm. After passing a temporary carotid occlusion test, the patient underwent partial aneurysm coiling and internal carotid artery coil occlusion. Nine coils were deployed (four 6 mm × 30 cm, three 6 mm × 20 cm, and two 5 mm × 12 cm). Total occlusion was obtained. There were no complications. The coils and the patient's condition were stable and unchanged at the 1-year follow up. fig 3. Magnified view of the detachment system shows the corkscrew-like base of the platinum coil from which the pusher wire is unscrewed
All patients enrolled in the study were suffering from a cerebral disease for which conventional endovascular embolization was indicated and were 18 years of age or older. Informed consent was obtained from the patient or from the patient's guardian. Institutional Review Board approval was obtained at each participating institution. All procedures were videotaped.
Exclusion criteria were participation in other clinical trial(s) that might interfere with this trial, any history of mental illness or psychiatric complaint, life-threatening illness other than the neurologic disease to be treated with the Detach-18 system, any septic hemodynamically unstable condition, or intubation due to other complications. Patients with saccular aneurysms on the cerebral arteries were excluded from the study but will be included in a future study.
Two types of coils, a 0.015-inch-diameter regular coil and a 0.014-inch-diameter soft coil, were used in the study. These are available in preshaped diameters and lengths. They are mounted on a 0.018-inch Teflon-coated stainless steel pusher wire by means of a microthread that screws clockwise into the hollow base of the platinum coil. The coils are provided mounted and ready for introduction. The pusher wire is not reused. The coil is delivered through a microcatheter with a 2.5F to 1.9F distal lumen, with two distal markers 3 cm apart. Constant heparinized flush was infused under pressure, through both the microcatheter and the guiding catheter, consistent with the standard Guglielmi detachable coil technique. When a 1-cm-long marker on the pusher wire is positioned just proximal to the proximal marker on the microcatheter, the coil is correctly positioned for detachment. When the coil has been placed in the desired position, the pusher wire is locked in place at the valve of the Y adapter by a locking device (essentially a modified torque device). This prevents unwanted motion of the coil and pusher wire that could potentially cause vascular injury during the rotations of the detachment process. The coil is deployed by counterclockwise rotation of the pusher wire, using the locking device. With the final counterclockwise rotation, the coil is released from the microcatheter tip (Fig 3). The detachment process takes place in the microcatheter. As with other coil systems, the regular 0.015-inch-diameter coils were used early in the procedure to create a basket and the softer 0.014-inch-diameter coils were used to pack the interstices tightly as the case progressed. Coil detachment can be identified by inward deflection of the most proximal part of the coil into the basket and by the ability to retrieve the coil pusher without moving the coil.
Results
A total of 569 coils were used, 541 of which were detached. Twenty-eight were deployed but retrieved before detachment. The number of coils deployed ranged in each patient from four to 53, with an average of 14. One hundred percent occlusion of the vessel lumen was achieved in 35 (85%) cases. In three (7%) cases, 80% to 90% occlusion was achieved. In two (5%) cases, 70% to 80% occlusion was achieved.
During the delivery process, the friction between the coils and the catheter was minimal and retrieval was easy. Coil delivery was smoother with the soft 0.014-inch-diameter coil than with the regular 0.015-inch-diameter coil. When the detachment zone of each coil was passed beyond the catheter tip before detachment, it was possible to retrieve into the microcatheter without premature detachment. Rotation of the pusher wire during the detachment process did not cause rotation of either the coil being deployed or the coil pack.
In one patient, one coil was placed but did not detach. The coil was readily retrieved, and the procedure was completed without further use of the Detach-18 system. The coil was readily detachable on “bench testing.” The problem may have been related to inadequate tightening of the torque device, such that while the torque device was rotating, the pusher wire was not and, therefore, the coil did not detach.
During this study, there were no device-related complications. The coils passed easily through the microcatheter. The detachment maneuver occurred within 10 to 25 s with 20 turns of the introducing wire. No premature coil detachment occurred, and there was no evidence of coil stretching, fracture, or migration.
Procedure-related complications occurred in four patients. One suffered a carotid dissection from an arterial catheter placed for control injections during a transvenous embolization of a dual AVF. One patient died as a result of intracranial hemorrhage after incomplete dual AVF closure. A review of the videotape in this case revealed that the venous sinus closure had resulted in the closure of a normal Labbé‘s vein. We assume this resulted in cortical vein rupture, leading to a fatal hemorrhage 3 hours after treatment. One patient was treated under emergent conditions for surgical trauma of the internal carotid artery siphon during pituitary adenoma surgery. Emergent internal carotid artery occlusion was performed with the Detach-18 system in the operating room. The patient died secondary to hemispheric infarction after left internal carotid artery occlusion. One patient suffered transient IXth and XIIth cranial nerve palsy after occlusion of a dual AVF of the condylar vein due to mass effect, but this resolved spontaneously. The images and videotapes of all procedures in which there were complications were reviewed by the study principals and were deemed related to the therapy but not to the Detach-18 coils.
Discussion
These in vivo tests showed that the Detach-18 system design is robust. A total of 569 coils were used, 541 of which were detached. Twenty-eight were deployed but retrieved. No premature coil detachment occurred. The coil is manufactured from platinum and therefore should not be subject to “corrosion” during long-term follow-up, which was recently reported to occur with tungsten coils (21).
Only one coil did not detach, which may have been because of a technical error on the part of the operator. In all other cases, detachment was fast and reliable. Of importance is that detachment time did not increase with progressive coil deployment. This is a common problem in the experience of most interventionalists when the Guglielmi detachable coil system is used in a large coil pack. The rapid detachment of the Detach-18 system may therefore have significant patient benefit in reduced procedure time and may reduce per procedural stroke risk and duration of anesthesia. The rapid occlusion of the internal carotid artery in the patient with surgical trauma is a good example of the benefit of the speed of this system. Because the coils are supplied mounted and the pusher wire is not reused, use of the system avoids the laborious and often difficult coil-loading procedure encountered with other mechanical coil systems. In vitro testing of this coil system reported by Piotin et al (22) has shown that the stiffness of these coils compares favorably with that of the Guglielmi detachable coils. The European Clinical Trial of these coils in the endovascular occlusion of intracranial aneurysms is ongoing.
Conclusion
We conclude that the Detach-18 system is a safe, reliable, consistent, and fast neurovascular embolization device. It may represent a significant addition to the interventional radiologist's armamentarium, allowing for a safe and reliable deployment of a large number of coils in clinically acceptable time. The European Clinical Trial will continue until 70 patients have been treated, and this patient population will be followed up for 1 year.
Footnotes
↵1 Address reprint requests to Kieran J. Murphy, MD, FRCPC, Director of Interventional Neuroradiology, Department of Radiology, B-100, 600 North Wolfe Street, Baltimore MD 21287.
References
- Received March 23, 2000.
- Copyright © American Society of Neuroradiology
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.