
Abstract
Summary: Hemangioendotheliomas are rare vascular tumors that can affect bone. They account for 0.5% to 1.0% of malignant primary bone tumors. Only four cases have been reported involving the temporal bone. A 5-year-old child with grade II hemangioendothelioma of the right temporal bone is presented, and the radiologic findings on different imaging studies are described. The patient was treated with preoperative endovascular embolization followed by wide surgical resection. The imaging patterns of this malignant tumor may be similar to those of a benign lesion.
Hemangioendothelioma is a rare vascular tumor composed of endothelial cells that can involve soft tissue or bone (1). The lesion has had multiple synonyms, including angiosarcoma, which is a less specific term for uniformly malignant vascular tumors, including proliferations of lymphatic vessels (2). Hemangioendotheliomas account for only 0.5% to 1.0% of malignant primary bone tumors. Most of them arise in the third decade, in vertebral bodies and long bones, with a minority growing in other bones, such as the pelvis, skull, or clavicle. Multicentric lesions also occur, and involve either multiple bones or multiple sites in a single bone (2). There are a few reports of involvement of the head and neck by hemangioendothelioma; however, to the best of our knowledge, only four cases involving the temporal bone have been reported (3–6). We present the findings of various radiologic studies of this malignant tumor of the temporal bone in a child.
Case Report
A 5-year-old girl was noted to have a small bony prominence in the right temporal region after sustaining minor trauma. No fever or hearing impairment was reported, and her medical history was unremarkable. On physical examination, the head was slightly asymmetric with a right temporal prominence, narrowing of the right external auditory canal, and right facial paresis.
Plain radiographs of the skull revealed a cephalic expansion of the petrous portion of the right temporal bone (Fig 1A), and a bone scan showed increased activity in this region (Fig 1B). CT studies revealed a well-defined expansile lytic lesion with trabecula formation involving mainly the petrous and squamous portions of the right temporal bone with focal extension into the tympanic and mastoid portions. No intracranial extension of the process was seen (Fig 1C). MR imaging showed a large expansile mass in the right temporal bone that was mostly isointense on T1-weighted sequences with small areas of high signal that most probably represented methemoglobin (Fig 1D). On T2-weighted images, the lesion was mostly hyperintense with areas of flow voids representing vessels within the tumor (Fig 1E). Significant enhancement was seen after intravenous administration of contrast material (Fig 1F).

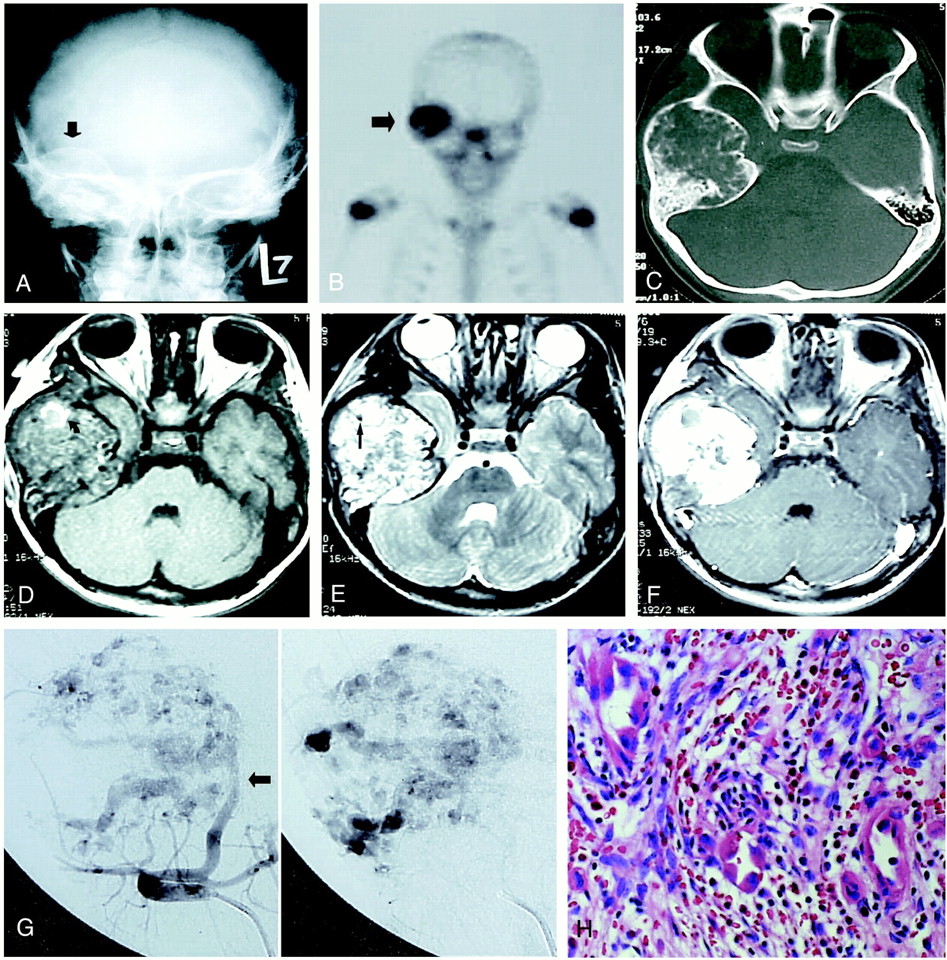
5-year-old girl who underwent imaging studies for a small bony prominence in the right temporal region after sustaining minor trauma.
A, Plain radiograph shows expansile lesion involving mainly the petrous portion of right temporal bone (arrow).
B, Technetium bone scan shows increased isotope uptake in the right temporal region (arrow).
C, Axial CT scan (bone window) shows an expansile tumor of the right temporal region with a coarse trabecular pattern and well-defined borders, involving the squamous, mastoid, and petrous portions of the temporal bone.
D, Axial unenhanced T1-weighted (500/20/2) MR image shows a large mass in the right temporal bone with well-defined borders, isointense signal in relation to brain, and scattered areas of high signal (arrow), most probably representing methemoglobin from thrombosed vessels (at histopathologic examination, the tumor lacked fatty tissue, a common cause of increased signal intensity).
E, Axial T2-weighted (2500/80/2) MR image shows the same lesion to be hyperintense relative to brain parenchyma, with evidence of flow voids, indicating the presence of vessels (arrow).
F, After contrast administration, axial T1-weighted (500/15/2) MR image shows marked enhancement of the lesion.
G, Anteroposterior view of the right external carotid angiogram (arterial and capillary phases, left and right, respectively) shows dilated vascular channels in the lesion, which is primarily supplied by the middle meningeal artery (arrow). The pooling of contrast material within the vascular channels of the lesion persisted well into the venous phase of the angiogram (not shown).
H, Photomicrograph shows vascular channels lined by plump endothelial cells having large, hyperchromatic nuclei, in a loose background stroma (hematoxylin eosin, original magnification ×40).
At angiography, the mass was hypervascular, with numerous dilated vascular channels and pooling of contrast material within the lesion. The tumor was primarily supplied by the middle meningeal branch of the external carotid artery, and there was no arteriovenous shunting (Fig 1G).
After preoperative embolization, the patient underwent a gross total surgical resection via a subtemporal-infratemporal-translabyrinthine approach. The petrous portion of the internal carotid artery was exposed owing to involvement of the bone of the carotid canal, and the facial nerve was exposed from the pontine dura to the pes anserinus, owing to tumoral involvement of the internal auditory canal and middle ear. The condylar fossa, the zygomatic arch, and a large area of the squamosal temporal bone were also resected, and reconstruction was performed of the entire area with titanium mesh. The patient was neurologically intact postoperatively except for a House-Brackmann grade V facial weakness, which improved to grade I over 6 months. The patient otherwise had an excellent cosmetic and functional recovery, including mastication. Microscopic examination showed a tumor composed of vascular channels lined by plump endothelial cells, which had enlarged hyperchromatic nuclei, producing a hobnail appearance of the neoplastic thin-walled blood vessels (Fig 1H). Nucleoli were not prominent, and mitotic figures were rare. Immunohistochemical stains confirmed the vascular nature of this tumor; however, these stains, which include factor VIII, CD31, and cytokeratin, are more useful in high-grade and poorly differentiated types, which have fewer vascular channels. On the basis of these combined findings, a diagnosis of grade II hemangioendothelioma was made.
Discussion
In 1903, Mallory introduced the term hemangioendothelioma to designate a vascular tumor that infiltrates surrounding tissue, recurs locally, and may metastasize (3). Hemangioendotheliomas are neoplastic proliferations of blood vessel endothelial cells, forming thin-walled blood vessels and sheets of neoplastic cells. These lesions have variable malignant behavior, depending on their microscopic features. In contrast, hemangioma is a benign neoplastic proliferation of blood vessel endothelial cells. Most, but not all, hemangioendotheliomas show poor histologic differentiation as compared with hemangiomas, as well as nuclear atypia and/or the presence of mitotic figures (2).
These tumors may be divided into three groups: grade I, grade II, and grade III. The diagnostic grades I through III (7) are based on the presence of (in grade I) abundant vascular channels lined by only mildly atypical neoplastic endothelial cells and rare mitoses. Grade III lesions show the most dramatic anaplastic features: dedifferentiation to epithelial areas resembling metastatic adenocarcinoma, fewer vascular channels, more striking nuclear atypia, including tumor giant cells, numerous mitotic figures, and tumor necrosis. Grade II hemangioendothelioma, to which the current neoplasm corresponds, shows anaplastic features intermediate between grades I and II: reduced numbers of neoplastic vascular channels, prominent nuclear atypia, and easily identifiable mitoses. In one large series (2), more hemangioendotheliomas of bone were classified as grade II (46%) than as either grade I (29%) or grade III (25%). Grade I hemangioendotheliomas can be distinguished from hemangioma because the angioblastic cells are larger and plumper in the former and do not mature into differentiated endothelial linings and vascular cavities. These tumors stain positive for factor VIII-related antigen (8).
The radiographic findings of hemangioendothelioma usually demonstrate an osteolytic pattern (2). Unni et al (7) found a positive correlation between the radiographic picture and the histologic grade, with low-grade tumors showing sharply demarcated margins and some bony trabeculae, whereas high-grade tumors had indistinct and irregular margins.
The CT and MR imaging findings in our patient revealed a large, well-defined expansile lesion involving most of the temporal bone with a honeycomb configuration and trabeculation; on angiography, the lesion was highly vascular. In previously reported cases of temporal bone hemangioendothelioma, only one patient had both MR imaging and angiography (4). In that case, the MR study showed mixed signal intensity on precontrast T1- and T2-weighted images and marked enhancement after contrast administration. The differential diagnosis in that case included glomus tympanicum, hemangioma, schwannoma, and granulation tissue. Angiography did not show a highly vascular lesion, contrary to that seen in our patient. Owing to the angiographic pattern and CT features, our patient's lesion was thought to represent an intraosseous hemangioma preoperatively.
Intraosseous hemangiomas of the cranium are benign tumors that represent only 0.2% of all bone neoplasms. They are more frequently seen within the frontal and parietal bones, less commonly within the occipital, temporal, and sphenoid bones (9, 10). CT may show an expansile, well-circumscribed bone lesion with a honeycomb configuration and a classic sunburst pattern of intradiploic trabeculation. MR imaging may show a mottled area of high signal on T1- and T2-weighted sequences; histopathologic studies reveal that fatty tissue is the main cause for the increased signal intensity on T1-weighted images, whereas the high signal on T2-weighted images is caused by the slow flow or pooling of blood. After intravenous contrast administration there is a rapid enhancement during an early phase that spreads into the entire lesion in a later phase (11). Similar characteristics were seen in our case of temporal bone hemangioendothelioma, except that on T1-weighted images only a small area of high signal intensity was seen, most probably related to the presence of methemoglobin. The radiologic findings are similar and difficult to differentiate from hemangiomas. However, high-grade (II and III) hemangioendotheliomas, present with indistinct and irregular margins and no evidence of trabeculation. Preoperative differentiation, when possible, is important because hemangioendothelioma is a malignant and aggressive lesion.
The treatment of choice for hemangioendothelioma has been surgical resection, combined with radiation, especially in high-grade lesions (1, 2). Radiation therapy has been used alone when surgery was not feasible (8). Chemotherapy currently has no significant role in the treatment. Orchard et al (12) reported successful treatment with α-interferon in two infants with hemangioendotheliomas, one in the head and neck region.
The overall survival is mostly related to the grade of the lesion (2). Grade I lesions have a 95% survival rate; however, survival falls to 62% for grade II lesions and to just 20% for grade III lesions.
Conclusion
Hemangioendothelioma of the temporal bone is a malignant bone lesion that can resemble a benign lesion on imaging studies.
Acknowledgments
We thank Luisa de Ibarra for preparation of the manuscript.
Footnotes
↵1 Address reprint requests to Prabhakar Kesava, MD, Department of Radiology, Division of Neuroradiology, University of Texas Health Science Center, 7703 Floyd Curl Dr, MC 7800, San Antonio, TX 78229.
References
- Received September 27, 2000.
- Copyright © American Society of Neuroradiology
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.