
Abstract
Summary: We report a case of atypical manifestation of hyperintense lesions in a 64-year-old female patient with Wernicke's encephalopathy. Fluid-attenuated inversion recovery and T2-weighted images demonstrated symmetrical distribution of hyperintense lesions in cerebellar dentate nuclei, tegmentum of the lower pons, red nuclei, and tectum of the midbrain, and T1-weighted sagittal images showed atrophy of the mamillary bodies. The hyperintense lesions were completely resolved on follow-up MR images.
The usual findings at MR imaging in patients with Wernicke's encephalopathy are well documented (1–9) and include high signal intensities in the medial thalami and periaqueductal regions of the midbrain. We report a case of Wernicke's encephalopathy that showed an unusual location of hyperintense lesions on fluid-attenuated inversion recovery (FLAIR) and T2-weighted images.
Case Report
A 64-year-old woman was admitted to a primary hospital with a 2-week history of headache, nausea, and vomiting. One month prior to admission, she had experienced several days of upper respiratory tract infection symptoms. Her medical history was nonspecific. At the time of admission, she was mildly drowsy, and physical examination revealed neck stiffness. A lumbar puncture was performed and revealed pleocytosis (WBC 2470). Assuming bacterial meningitis, antibiotic therapy was started. On the third day after admission, she underwent brain CT scanning and was transferred to our hospital with a suspected brain abscess.
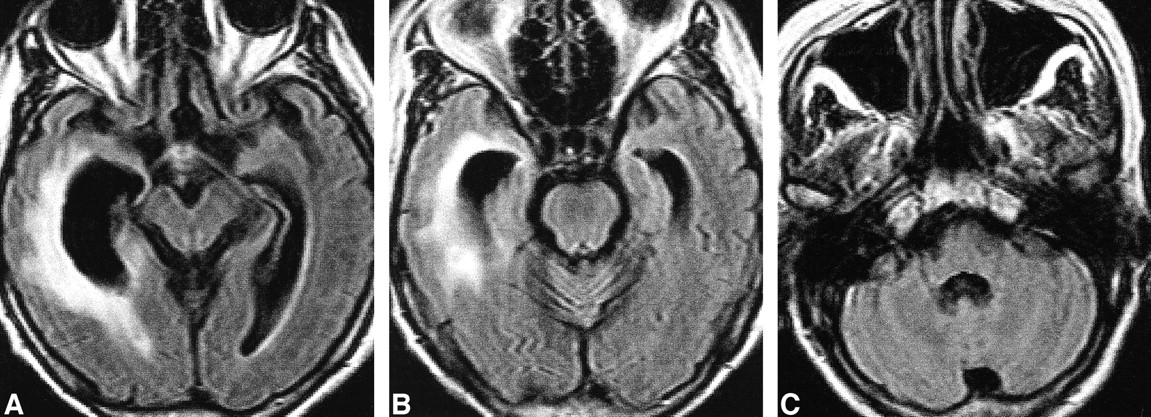
She continued to be mildly drowsy. Neurologic examination was negative except for a left homonymous hemianopsia. An initial brain MR study showed an abscess cavity in the right peritrigonal area (Fig 1A). The mamillary body appeared normal in size (Fig 1B). Antibiotic therapy was continued. During the therapy, her oral intake remained poor because of excessive vomiting. Her level of consciousness deteriorated to a stupor 80 days after her initial admission. On neurologic examination, the pupils were normal in size and reacted to light. The eyeballs were almost fixed with spontaneous bidirectional horizontal nystagmus. Papilledema was not detected. Spastic paraparesis was noted without pathologic reflexes. Electroencephalography showed diffuse delta slowings, suggestive of a metabolic cause. Follow-up brain MR at that time (77 days after the initial MR imaging) revealed symmetrical distribution of multifocal hyperintense lesions in the red nuclei and tectum of the midbrain, cerebellar dentate nuclei, and tegmentum of the lower pons (facial, abducens, and vestibular nuclei) on FLAIR (Fig 2A–C) and T2-weighted images. Atrophy of the mamillary body was also observed on T1-weighted sagittal images (Fig 2D) without definite hyperintensity on FLAIR and T2-weighted images (not shown). No definite hyperintensity was demonstrated in either medial thalami on FLAIR or T2-weighted images. The abscess cavity observed in the right peritrigonal area decreased in size (not shown). With her clinical features, the diagnosis of Wernicke's encephalopathy was made. At that time, a daily intravenous injection of 500–1000 mg of thiamine was started. One week from the start of the thiamine therapy, the ophthalmoplegia and nystagmus were almost absent. Her level of consciousness gradually improved over the next several weeks to the point where she was alert and communicative. On the third MR study (40 days after the second MR imaging), the multifocal hyperintense lesions detected on the previous MR images were completely resolved (Fig 3).
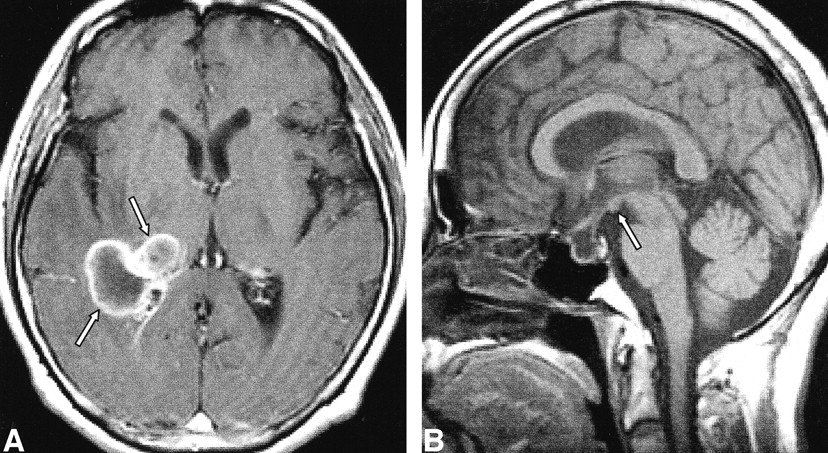
March 22.
A, Contrast-enhanced T1-weighted axial image shows abscess cavity (arrows) in the right peritrigonal area.
B, T1-weighted sagittal image shows normal-appearing mamillary body (arrow).

May 29.
A–C, FLAIR axial images.
A, Red nuclei of the midbrain are hyperintense compared with the brain parenchyma (solid arrows). White matter hyperintensity (open arrow) adjacent to the dilated right lateral ventricle is probably a change due to the abscess cavity.
B, Tectum of the midbrain also shows symmetric hyperintensities (arrows).
C, At the lower pons level, symmetrical hyperintense lesions are also detected in facial nuclei (solid arrows), vestibular nuclei (open arrows), and abducens nuclei (arrowheads) of the pontine tegmentum and cerebellar dentate nuclei (double arrows).
D, T1-weighted sagittal image shows atrophy of mamillary body (arrow).
July 10.
A–C, FLAIR axial images show complete resolution of the previously detected unusual hyperintense lesions. Residual white matter hyperintensity is noted along the dilated right lateral ventricle.
Discussion
Wernicke's encephalopathy is a neurologic disorder with acute onset, characterized by the triad of ocular abnormalities, ataxia, and a confused state (2, 5–7). It is caused by a thiamine deficiency due to poor oral intake in chronic alcoholics, food refusal, or recurrent vomiting in a pregnant patient. When the patient is in a comatose state, diagnosis of Wernicke's encephalopathy is difficult. In our case, the diagnosis of Wernicke's encephalopathy was initially based on her clinical manifestations. Her clinical setting of long-standing poor oral intake due to recurrent vomiting, the neurologic findings of ophthalmoplegia with nystagmus, and mental confusion made the possibility of Wernicke's encephalopathy likely. Good clinical response to the thiamine challenge was consistent with the diagnosis.
The usual locations of involvement on MR images in patients with Wernicke's encephalopathy are the medial thalami, tectum of the midbrain, and the periaqueductal region (1–9). In addition, the acute stage may show mamillary body enhancement (6), while the chronic stage may show atrophy of the mamillary bodies and midbrain tegmentum, as well as dilatation of the third ventricle (1, 4, 8). To our knowledge, there has been only one report describing additional symmetrical involvement of hyperintense lesions in central and precentral sulci other than the usual diencephalic and brain stem lesions (10). In our case, the hyperintense lesions in the tectum of the midbrain and the atrophy of the mamillary bodies were compatible with the previous literature, whereas the red nuclei of the midbrain, the tegmentum of the lower pons, and the cerebellar dentate nuclei were unusual locations of involvement, and those lesions resolved completely at follow-up MR imaging.
The mechanisms underlying the pathogenesis of the lesions observed in Wernicke's encephalopathy are not understood completely. The phosphoric esters of thiamine are involved in the function of excitable membranes, glucose metabolism, and neurotransmitter production. Thiamine-deficient membranes are unable to maintain osmotic gradients, which results in the swelling of intra- and extracellular spaces. In the periventricular regions, the blood-brain barrier is defective and there is a high rate of thiamine-related glucose and oxidative metabolism (3). This could explain the hyperintense lesions adjacent to the fourth ventricle in our case. However, we cannot explain the selective involvement of the cranial nerve nuclei of the lower pons and the red nuclei of the midbrain.
Pathologic changes in Wernicke's encephalopathy have been reported in a few studies. Microscopically, typical features are edema, marked spongy degeneration of the neuropil and neuron sparing, swelling of capillary endothelial cells, and extravasation of red blood cells (5). In chronic lesions, there is tissue destruction by macrophages and hypertrophic astrocytosis (10).
Ashikaga et al (9) reported that MR imaging with FLAIR sequences in a case of Wernicke's encephalopathy demonstrated better lesion conspicuity than did T2-weighted imaging. The lesions in our case were also more conspicuous at the first follow-up MR imaging with FLAIR sequence.
The hyperintense lesions in our case were located mainly in deep gray matter and were symmetrically distributed. Thus, the differential diagnosis could include demyelinating/dysmyelinating disease, such as multiple sclerosis, Behcet's disease, or central pontine or extrapontine myelinolysis. However, demyelinating diseases could be excluded due to their asymmetrical distribution, while central pontine myelinolysis mainly involves pontine basis without an association with the fourth ventricle, and Behcet's disease can involve the brain stem, but it typically shows asymmetrical distribution.
Wernicke's encephalopathy can show various findings on MR images, thus the clinical feature is essential to diagnose it.
Footnotes
1 Address reprint requests to Ho Kyu Lee, MD, Department of Radiology, Asan Medical Center, 388–1 Poongnap-Dong, Songpa-Ku, Seoul 138–040, South Korea.
References
- Received October 16, 2000.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Metronidazole-induced encephalopathy after prolonged metronidazole course for treatment of C. difficile colitis
- Walking unsteadily: a case of acute cerebellar ataxia
- Spectrum of MR Imaging Findings in Wernicke Encephalopathy: Are Atypical Areas of Involvement Only Present in Nonalcoholic Patients?
- MR Imaging: An Increasingly Important Tool in the Early Diagnosis of Wernicke Encephalopathy
- MR Imaging Findings in 56 Patients with Wernicke Encephalopathy: Nonalcoholics May Differ from Alcoholics
- Bright red nuclei