
Abstract
Summary: A 41-year-old patient with a history of low back pain underwent conventional radiography, CT, digital subtraction angiography (DSA), and MR imaging. An inhomogeneous sclerotic-lytic lumbar vertebra with slightly thickened spongiotic structure and intense contrast enhancement were compatible with an L4 vertebral hemangioma. Embolization and posterior surgical osseous decompression was performed. Histologic analysis of osseous parts revealed a vertebral lymphangioma instead of a hemangioma.
Primary lymphangiomas involving bone are extremely rare. Few cases have been reported in the literature, and lesions in these cases affected the mandible, tibia, humerus, calvaria and spine (1–8). Because of the rarity of this disease and the nonspecific clinical and radiologic features, establishing the diagnosis is extremely difficult. This report describes the case of a primary lymphangioma affecting a single vertebral body. It was investigated by means of conventional radiography, CT, MR imaging, digital subtraction angiography (DSA), and histologic analysis, and it was treated with endovascular embolization and surgery.
Case Report
A 41-year-old patient presented with low back pain, which had been occurring for years. More recently, intermittent sciatica had developed. Conventional radiographs depicted an inhomogeneous sclerotic-lytic L4 vertebra (Fig 1). On CT scans, an attenuated, slightly thickened spongiotic structure of this vertebral body was seen in combination with enlargement of the interspaces (Fig 2). MR imaging of the lumbar spine showed the L4 vertebra with an inhomogeneously hyperintense structure on T2-weighted images, combined with an inhomogeneous decrease in signal intensity on T1-weighted images. Intense enhancement was seen after the administration of gadolinium-based contrast agent. Images depicted a dorsal epidural soft-tissue mass with increased homogeneity and with comparably intense enhancement (Figs 3–5). A vertebral hemangioma was diagnosed.
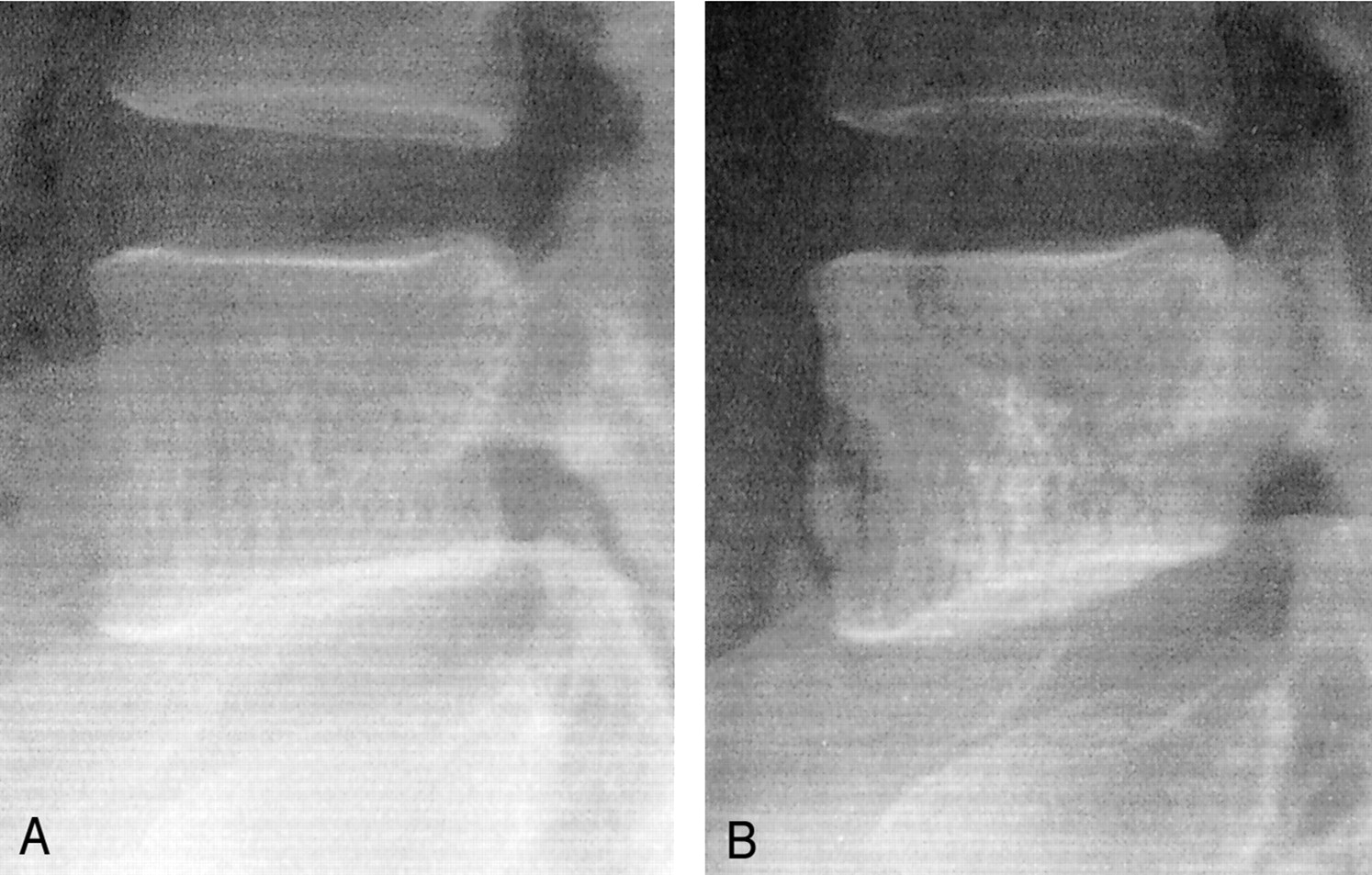
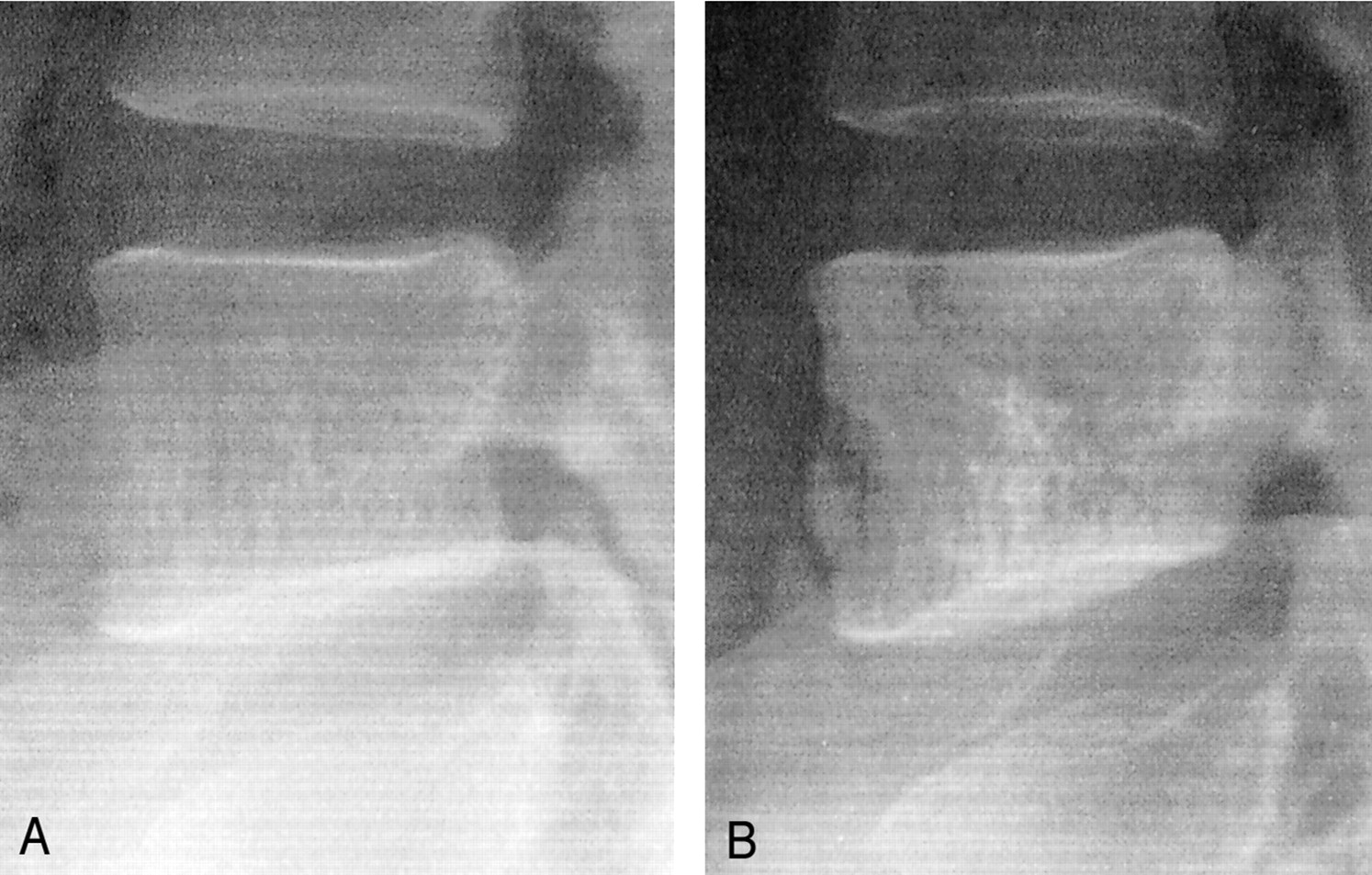
Conventional radiographs show a progressive attenuation of the L4 vertebral body, with trabecular pattern as well as erosion of the anterior cortex of the vertebral body.
A, Initial image.
B, Image obtained 5 months later (right).

CT scan (section thickness, 3 mm; bone algorithm reconstruction) of L4 reveals a coarse bony trabecular structure, with the shape of the vertebral body preserved. This finding suggests a hemangioma.

Sagittal T1-weighted MR images obtained before (left) and after (right) contrast medium administration shows inhomogeneous signal intensity in L4, with homogeneous intense enhancement of the soft-tissue mass.
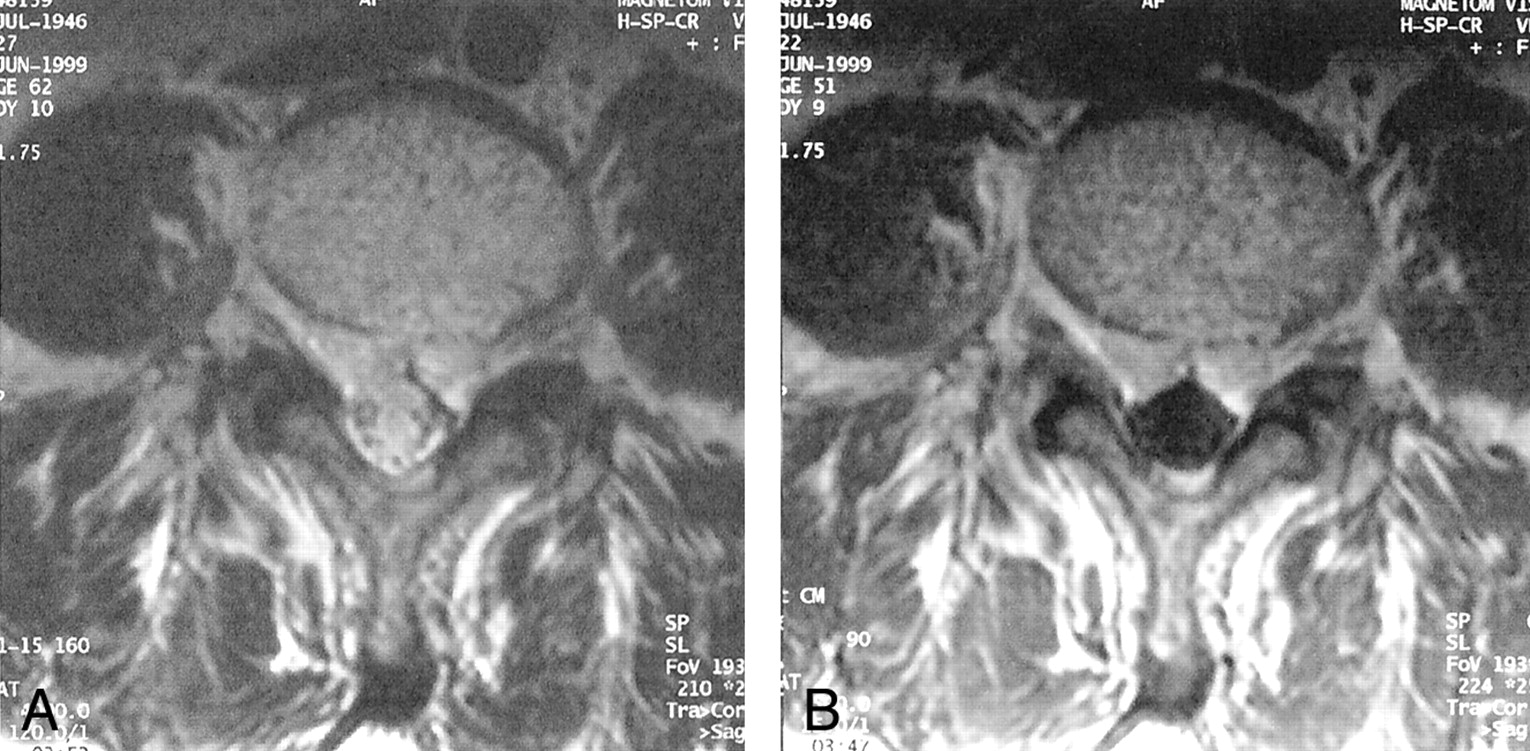
Axial MR images.
A, T2-weighted image reveals the coarse, inhomogeneously hyperintense structure of L4 and the soft-tissue mass.
B, T1-weighted image obtained after the administration of contrast material shows enhancement of vertebral body and the soft tissue.

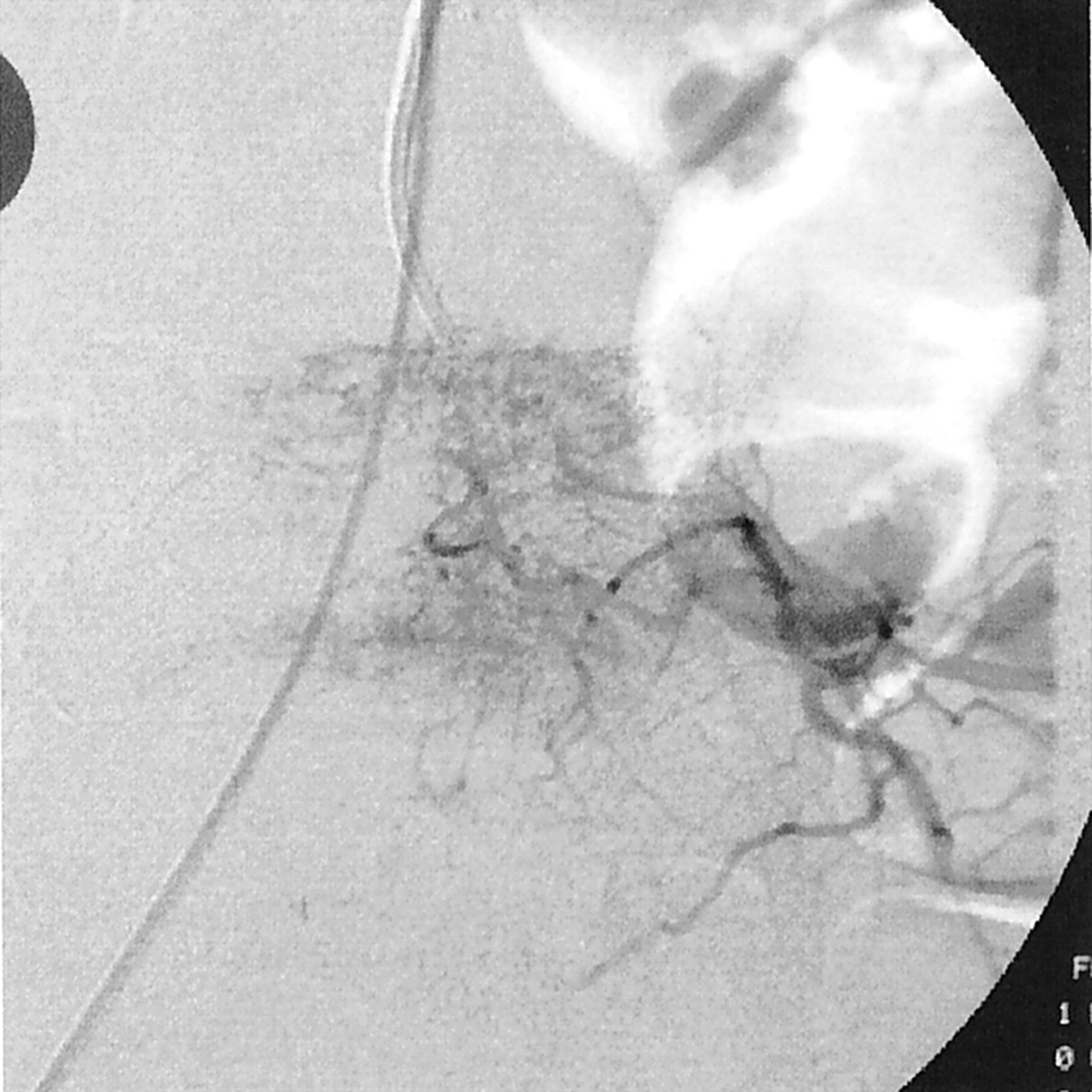
Superselective angiogram of the lumbar spinal artery at L4 on the left side shows a major feeding radicular artery as well as the hypervascularized vertebral body.
After unsuccessful conservative therapy, arterial embolization of the presumed hemangioma was performed. digital subtraction angiography (DSA) revealed a major feeding artery arising from the right spinal artery at L4, which subdivided in numerous smaller vessels (Fig 5). These single feeders and finally the distal spinal artery L4 were occluded by using a total of 1.8 cm3 of 20% dilution of Ethibloc (Johnson & Johnson, Brussels, Belgium), which was administrated by using a microcatheter (Tracker-18; Boston Scientific, Cork, Ireland). After 3 days, the initial clinical progress diminished. Four months later, MR images showed the epidural mass described before, with the same signal intensity characteristics. Conventional radiography showed a progression with a mixed sclerotic-lytic appearance. To stabilize the vertebral body and for pain treatment, a vertebroplasty with a total of 14 cm3 of methyl acrylate was performed transpedicularly and bilaterally. Again, the initial clinical improvement was only transient. Two months later, the patient developed paresis and hypesthesia precisely at L5. CT revealed a spinal stenosis due to the compression of the lateral recesses by methyl acrylate, leading to a bilateral involvement of the nerve roots at L5. Surgical osseous decompression, removal of the displaced methyl acrylate, partial hemilaminectomy, and bilateral foraminotomy were performed. Histopathologic examination showed an osteolytic lesion composed of numerous dilated lymphatic vessels appearing as microscopic cysts. These were filled with a slightly eosinophilic mass. The irregular, thin-walled vascular channels showed dissection of the collagen bundles and poor lymphocytic infiltrate in the surrounding fibrosis stroma. The spaces were lined by a single layer of flat endothelial cells with, at most, very mild cytologic atypia. Their lumina often appeared empty or contained a few red blood cells and proteinaceous material (which was mostly washed out with fixation and preparation). Immunohistochemical procedures showed CD34-positive staining, identifying lymphatic endothelium (Figs 6 and 7). The bone of the turbulence body showed slight signs of resorption.
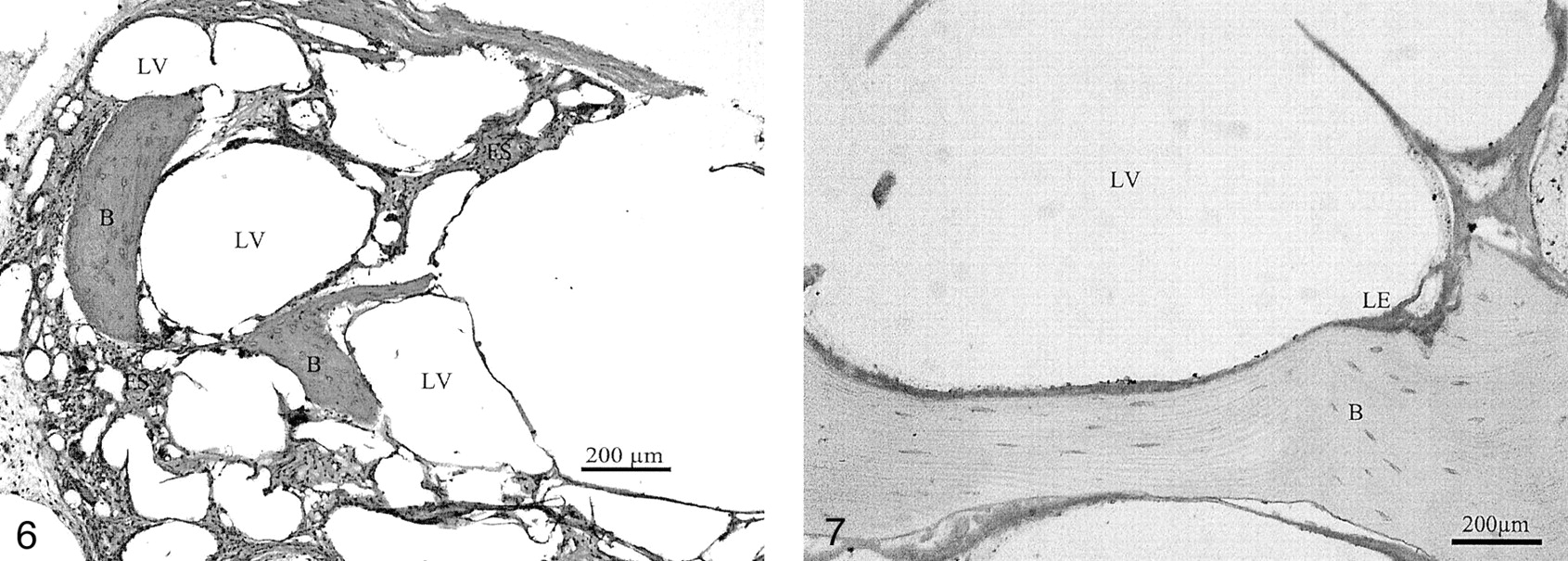
Histologic section shows numerous dilated vessels within the bony structures of the vertebral body. The bone shows areas of slight resorption. The vascular channels have irregular, thin walls (hematoxylin-eosin).
Note.—LV indicates lymphatic vessel; LE, lymphatic endothelium; B, bone.

Immunohistochemical procedures show CD34-positive staining, depicting lymphatic endothelium. The bone of the turbulence body shows slight signs of resorption.
Note.—LV indicates lymphatic vessel; LE, lymphatic endothelium; B, bone.
One year later, the right-sided hypesthesia at L5 and the lower back pain persisted, but a mild right-sided paresis developed at L5. The pain intensified as a result of flattening of the vertebra, which finally lead to corpectomy of L4. Two-year follow-up was performed. The patient reported considerable improvement in the low back pain, which only occurred after long periods of sitting. Findings at neurologic examination were normal.
Discussion
Lymphangiomas are benign and uncommon tumors composed of sequestered and non-communicating lymphoid tissue lined by lymphatic endothelium probably of malformative origin. Bickel and Broder first described this entity in 1947, in the ilium of a 5-year-old child. Since then, several reports of this entity have been published. The lesions affect almost every part of the body, with a predilection for the head, neck, and axilla. In fact, this diagnosis is much more common in children than in adults, as 90% of the tumors are found by the time the patient is aged 2 years. In a more recent review of the embryology of the vascular system, Fordham et el (9) described the lymphatic system as an outgrowth of the venous system starting at the 8th week. They state that lymphatic malformations “are thought to be secondary to an intrauterine obstruction or arrest in lymphatic development,” and therefore, they are different in terms of the histologic findings and their embryologic age.
Solitary lymphangiomas involving bone are extremely rare. To our knowledge, only nine patients have been reported since 1956, when Falkmer and Tilling (1) published the first case (Table). The exact incidence of pure lymphangiomas involving the skeleton is not well documented, perhaps because of its clinical, radiologic, and histologic similarity to hemangiomas and because of the common overlapping elements in both entities. Thus, multiple terms have been used, including skeletal hemangiomatosis, multiple lymphangiectasis of bone, cystic lymphangiomatosis of bone, and others; these are probably different forms of the same hamartomatous abnormality of the lymphatic system.
Cases of primary lymphangiomas involving bone reported in the literature
Although some have questioned the real existence of lymphatic vessels in medullary bone (10), others, using different methods, have demonstrated its presence (6). Dilated endothelium-lined channels appear similar or identical to both lymphangiomas and hemangiomas. The absence of erythrocytes inside channels, as well as the presence of a proteinaceous eosinophilic fluid material within it, is critical for a definitive diagnosis of lymphangioma.
Primary lymphangiomas affecting the spine are extremely uncommon; to our knowledge, only one case involving a single vertebral body has been previously reported. In 1995, Keenan et al (8) reported the first case, which was in a 12-year-old girl with a lymphangioma of the third lumbar body without extension to the spinal canal; it was associated with a big cystic mass arising from the vertebral body. However, in 1956, Falkmer and Tilling (1) did report the first case of a primary lymphangioma that affected the bone, with involvement of several vertebral bodies and sacrum. Some years ago, Wenz et al (6) reported another case that affected two vertebral bodies with late extension to a rib, as confirmed at lymphangiography. Those reports and a similar one by Hayashi et al (7) describe patients with a primary lymphangioma involving a thoracic rib and thoracic spine. To our knowledge, these are the only cases in the literature regarding primary involvement of vertebral bodies in this entity without an association with lymphangiomatosis. Rogers and Chou (11) also reported a case of a lymphangioma involving upper cervical vertebrae and calvaria, but in the follow-up period, Edwards et al (12) demonstrated the true diagnosis for that patient was a lymphangiomatous, massive osteolysis of the cervical spine. This lesion is a rare and aggressive entity of primary lymphangiomatosis, angiomatosis, or a combination of the two. It is reported to be associated with lymphangiomatosis or lymphangiomas and is characterized by the progressive reabsorption of bone.
Bone involvement is more commonly associated with lymphangiomatosis, a rare disorder characterized by replacement of visceral organs, soft tissue, and/or skeleton by multiple lymphangiomas located in the same or widely separated regions (12, 13). Histopathologically, it is usually mixed with angiomatosis, and by convention, the term is reserved for cases with a predominant or exclusive lymphatic component.
Most lymphangiomas are usually found in children; however, 80% of reported cases of primary lymphangiomas arising from bone, including our case, occur in adult patients.
As can be seen in the Table, all cases with vertebral involvement were symptomatically related by different degrees of bone lysis and/or nerve compression. (In the article by Hayashi et al [7], information related to symptoms was not available.) Our case showed progressive weakness and vertebral collapse requiring fixation and bone autograft. In the case reported by Wenz et al (6), the lesion extended to the neighboring right rib after 5 years of follow-up. Cases involving the humerus, the calvaria, and the tibia had an excellent response to surgery or radiation therapy, without complications or recurrence during follow-up. (No information was available concerning the evolution of the cases reported by Ellis and Brannon [4]). When lesions are located in the axial skeleton, the diagnosis is difficult because more common diseases have similar radiologic features. Lytic, lytic-sclerotic, and cystic multiloculated radiologic patterns, in addition to the cortical or intraosseous location, make the list of differential diagnoses long. In vertebrae, the coarse bony trabeculae, the inhomogeneous aspect of the vertebral body, and the CT and MR imaging features described previously make hemangioma the primary diagnostic possibility. A definite diagnosis can be made only by means of histopathologic analysis. According to the various radiologic features reported, the differential diagnosis must include diseases that can cause lesions with honeycomb patterns. These include aneurysmal bone cysts as well as other vascular tumors, giant cell tumors, eosinophilic granulomas, fibrous dysplasias, osteomyelitis, and metastases.
From a practical standpoint, the diagnosis of vertebral lymphangioma does not change the therapeutic approach, in comparison to hemangioma. Nevertheless, the examination of cases of this rare entity could lead to a better understanding of the embryologic development and clinical presentation of such lesions.
Acknowledgments
We are very grateful to Mr Glenn Balke for his useful editorial assistance.
- Accepted after revision June 17, 2002.
- Accepted after revision June 28, 2002.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.