
Abstract
Summary: We report cases of two siblings with frontonasal dysplasia (FND) associated with multiple pericallosal lipomas in almost similar locations. In each sibling two separate curvilinear pericallosal lipomas were present—one in relation to the posterior part of the corpus callosum and the other in relation to the rostrum. To our knowledge, multiple pericallosal lipomas in association with FND have not been described before. Pericallosal lipomas in cases of FND are of the tubulonodular type; they have been reported only in relation to the anterior part of the corpus callosum.
Frontonasal dysplasia (FND) is a term that Sedano et al (1) used in 1970 to describe a constellation of findings limited to the face and head. The association between FND and pericallosal lipoma is well documented (2–5). In previous reports, the lipoma was always related to the anterior part of corpus callosum and was of the tubulonodular type that seldom extends posteriorly to surround the caudal aspect of corpus callosum. In our patients, the lipomas were curvilinear and were separate in relation to two portions of corpus callosum. The aim of this report is to present a pericallosal lipoma that is unusual in terms of its multiplicity, shape, and location in two siblings with FND.
Case Reports
We report the cases of two siblings of first-degree consanguinous parents who had eight other healthy children. At the time the first affected child was conceived, the father was 50 years old, and the mother was 40 years old. Our patients were the sixth and eighth among the siblings. Both parents and all siblings were phenotypically healthy.
Case 1
A 12-year-old girl with hypertelorism and congenital craniofacial deformities in the form of a median cleft affecting the palate, lip, and nose presented to our hospital for surgical correction. The mother’s pregnancy and delivery were uneventful. The patient’s intelligence was normal. The patient had no history of seizures or headache. CT scans of the facial bones showed hypertelorism, a depressed and bifid nasal bridge, and depression of the floor of the anterior cranial fossa. Findings from a skeletal survey were unremarkable. MR imaging revealed two pericallosal lipomas, one in relation to the rostrum and the other in relation to the splenium; these measured 0.8 and 1.9 cm in maximum diameter in the axial plane (Fig 1). The corpus callosum was well developed.
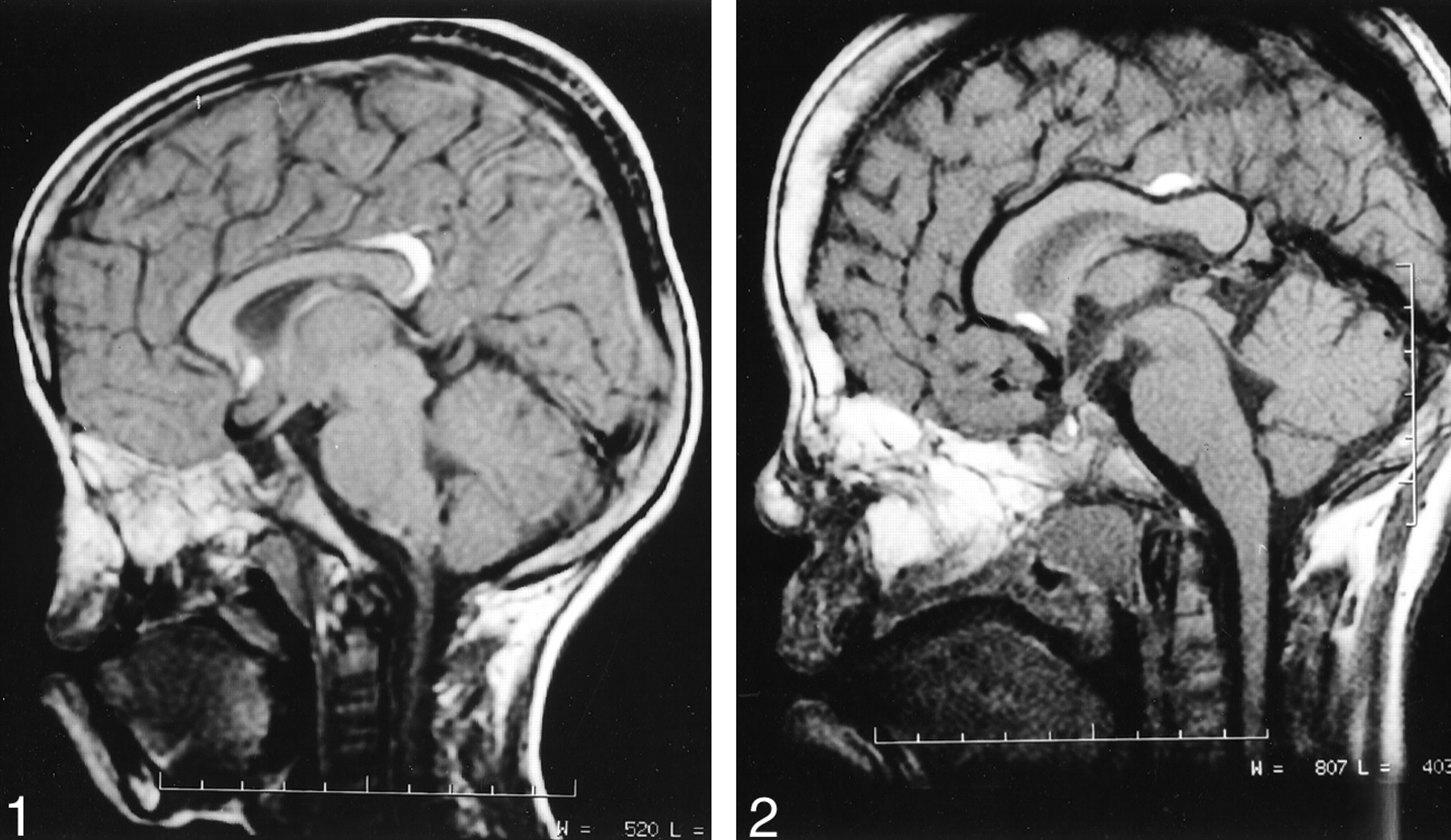
Case 1. Midsagittal T1-weighted MR image (TR/TE/NEX, 550/20/1.5) of the brain shows two small curvilinear pericallosal lipomas, one in relation to the rostrum and the other in relation splenium of corpus callosum. The corpus callosum is well developed. The deformity in the nasal region is depicted.

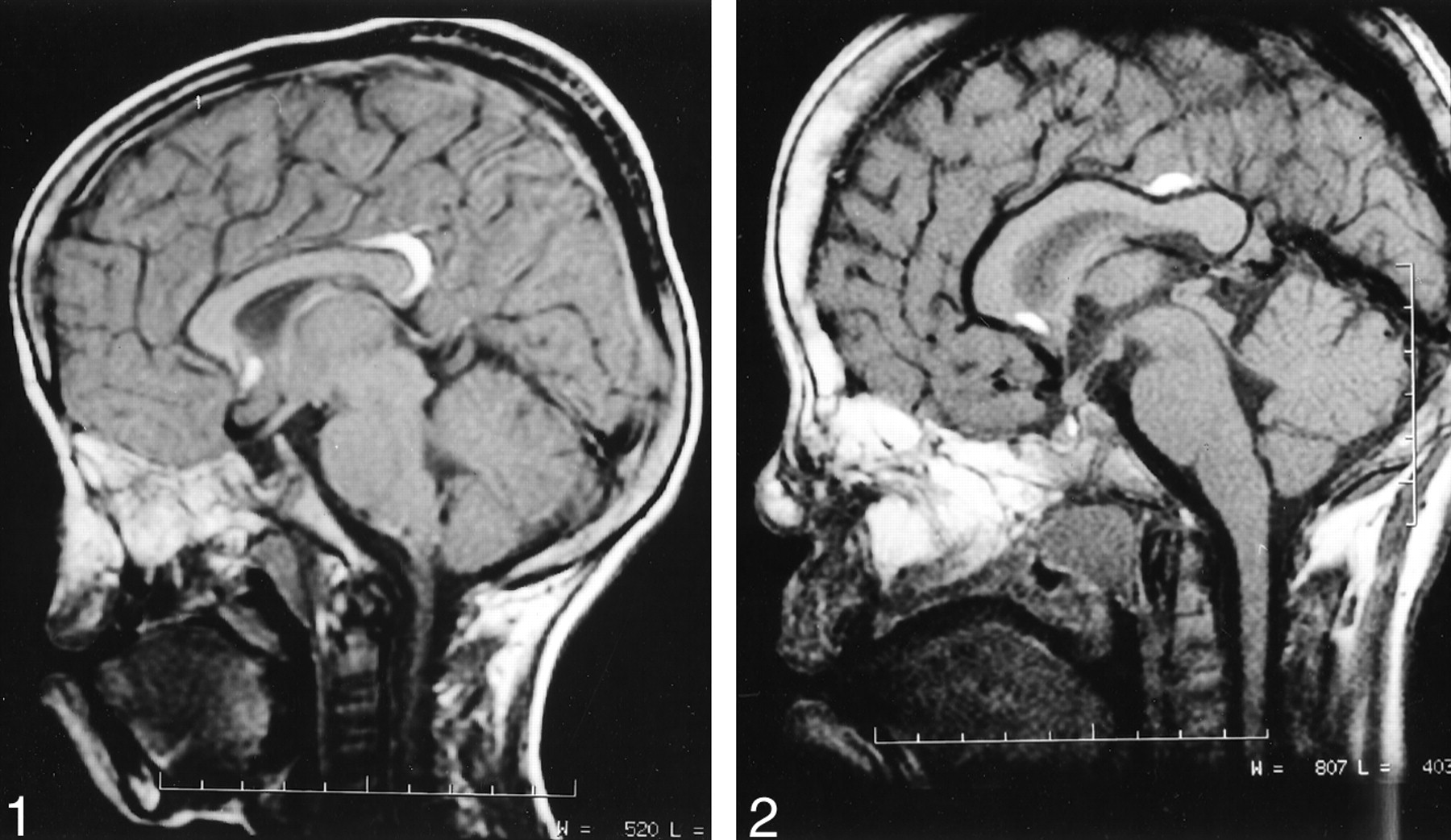
Case 2. Midsagittal T1-weighted MR image (500/20/3) of the brain shows two small curvilinear pericallosal lipomas, one in relation to the rostrum and the other in relation to the junction of body and splenium of corpus callosum. The corpus callosum is well developed. The deformity of the nose is depicted.
Case 2
A 7½-year-old boy wih a cleft palate, bifid nose, absent nasal bridge, and hypertelorism presented to our hospital for surgical correction. The mother’s pregnancy and delivery were uneventful. The patient’s intelligence was normal. He had no history of seizures or headache. CT scans of the facial bones showed hypertelorism, an absent nasal septum, an anteriorly bifid nasal bone, and a depressed nasal bridge. All paranasal sinuses were absent except the anterior ethmoidal air cells. Findings from a skeletal survey were unremarkable. MR imaging revealed two pericallosal lipomas, one in relation to the rostrum and the other in relation to the junction of body and splenium of corpus callosum; these measured 0.8 and 1.5 cm in maximum diameter on the axial plane (Fig 2). The corpus callosum was well developed.
Discussion
FND is a rare midline anomaly. The main features are true ocular hypertelorism; broadening of the nasal root; a median facial cleft affecting the nose, upper lip, and palate; uni- or bilateral clefting of the alae nasi; lack of formation of the nasal tip; anterior cranium bifidum occultum; and a V-shaped prolongation of the hair onto the forehead (1). This condition is usually sporadic, but a few familial cases have been reported (4, 5). Some reports are consistent with either autosmal or x-linked dominant inheritance (5). Beacause of the rarity of FND, the frequency of the association between FND and pericallosal lipoma is difficult to determine precisely. However, in 21 patients with FND, Guion-Almeida et al (4) found four cases (19%) of pericallosal lipomas. FND may be associated with congenital heart abnormalities, in particular, tetralogy of Fallot (3–5), vertebral anomalies, agenesis of the cropus callosum, Dandy-Walker malformation, a short neck, short limbs, polydactyly of the hands and feet, and cryptochidism (5).
Although the mother and father were relatively old when the first affected child was conceived, this finding may not be relevant. That two affected siblings of different sexes were born to healthy consanguinous parents is highly suggestive of an autosomal recessive pattern of inheritance. Because FND is pathologically heterogenous with a wide variability of anomalies in the reported cases, the identical location of the lipomas in the corpus callosum in the two siblings suggests the autosomal recessive mode of inheritance. This pattern may be distinct for the autosomal recessive subset of this malformation, and its appearance may warrant screening for such anomalies in FND.
Lipomas account for approximately 0.34% of all intracranial tumors. Pericalosal lipomas accounting for 47% of these (6) and have a frequency of 1 in 2500 to 1 in 25000, as reported in an autopsy series (7). Intracranial lipomas have traditionally been classified as hamartomas or tumors, while, in fact, they are congenital malformations (8). Because the corpus callosum may be entirely absent, the term interhemispheric lipoma is preferred to corpus callosum lipoma or pericallosal lipoma (7, 8), particularly true in cases of the tubulonodular type. Because of its popularity, the term pericallosal lipoma is used in this article. The origin of intracranial lipomas is believed to be due to the lack of resorption and the abnormal differentiation of the primitive meninx to mature adipose tissue during the development of the subarachnoid space. Verga originally suggested this embryologic theory in 1929 (9) and subsequentley modified by others (8), and it is still considered the most acceptable one (7, 8). Truwit and Barkovich (8) described two subgroups of pericallosal lipomas: curvilinear and tubulonodular. They indicated that the latter is a result of a more severe insult that occurs at an earlier embryonic stage and therefore interferes with the normal development of the corpus callosum. Commonly, the tubulonodular type is located anteriorly (with the epicenter at the genu in 83% of cases), and it is associated with a high incidence of facial defects, frontal masses, and/or encephaloceles (10). Curvilinear lipomas are thin and located posteriorly around the splenium. This type is generally associated with a normal corpus callosum, and it has low incidence of associated anomalies (7, 10).
In previous reports, pericallosal lipomas associated with2 FND were always of the tubulonodular type and located anteriorly (2–5). This finding is explained by the fact that tubulonodular lipomas, compared with curvilinear lipomas, are formed at an earlier embryonic stage before the anterior neuropore closes; thus, the tubulonodular lipomas interfere with the devolepment of the brain and calvarium (7, 8, 10). The region of the lamina terminalis is the most common site for intracranial lipomas because the meninx in this region is the last to be resorbed (8). The presence of another lipoma around the splenium and posterior body of the corpus callosum in our patients suggests that the disappearance of the meninx from this region also occurs late. To our knowledge, multiplicity of pericallosal lipomas has not been described before.
References
- Received February 28, 2001.
- Accepted after revision October 22, 2001.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.