
Abstract
Summary: Posttransplantation lymphoproliferative disorder (PTLD) is a challenging complication associated with organ transplantation and is usually fatal if untreated. We describe the case of a transplant recipient who presented with rapidly progressive cranial nerve palsies due to PTLD that originated in the sphenoid sinus. In this case, the clinical and radiologic presentation of PTLD mimicked invasive fungal disease. Because the management of PTLD and the management of invasive fungal infection are vastly different, prompt pathologic diagnosis is required.
The use of potent immunosuppressive regimens has greatly improved graft survival in organ transplant recipients. However, use of these agents has been associated with an increase in the incidence of lymphoproliferative disorders (1). Posttransplantation lymphoproliferative disorder (PTLD) is a serious complication of organ transplantation and chronic immunosuppression that represents unregulated B-cell proliferation ranging from benign polyclonal hyperplasia to non-Hodgkin lymphoma (2). It has a strong predilection for extranodal sites, most frequently involving the gastrointestinal tract, the CNS, and the allografted organ (1, 3). Head and neck involvement is relatively rare, presenting as focal submucosal masses involving Waldeyer’s ring or as cervical lymphadenopathy (4). PTLD arising from the paranasal sinuses has not been well reported. We describe the case of a patient who presented with multiple cranial nerve palsies due to PTLD that arose in the paranasal sinuses and spread to the skull base. Invasive fungal disease was initially suspected based on the patient’s clinical presentation and imaging findings. Because PTLD may mimic invasive fungal disease, prompt diagnosis is required to initiate appropriate therapy.
Case Report
A 53-year-old man presented with diplopia and left proptosis of 2 days’ duration and 20.5-kg weight loss during the 2 months before admission. His medical history was remarkable for a left lung transplant for emphysema 8 years previously. His chronic immunosuppressive regimen consisted of cyclosporine and prednisone until 6 months before admission, at which time it was changed to tacrolimus, mycophenolate, and prednisone because chronic rejection of his transplanted lung was suspected.
The results of a physical examination were remarkable for multiple cranial nerve palsies, including the left Vth (opthalmic and maxillary divisions) and VIth nerves, and a decreased left pupillary response. During the next 2 hospital days, the patient developed left IIIrd and IVth nerve palsies and decreased vision in his left eye. The remaining results if the neurologic examination were unremarkable. The patient was afebrile. Clinically, an invasive fungal infection was suspected. An emergent MR imaging study showed a peripherally enhancing mass involving the sphenoid sinus and the posterior ethmoid air cells, which was hypointense on T1- and T2-weighted MR images (Fig 1A–C). CT showed erosion of the skull base and an osseus defect in the left lateral sphenoid sinus wall (Fig 1D and E). The disease extended into the left infratemporal fossa/masticator space, multiple skull base foramina were observed, and intracranial spread could be seen along the dura of the left middle cranial fossa (Fig 1).

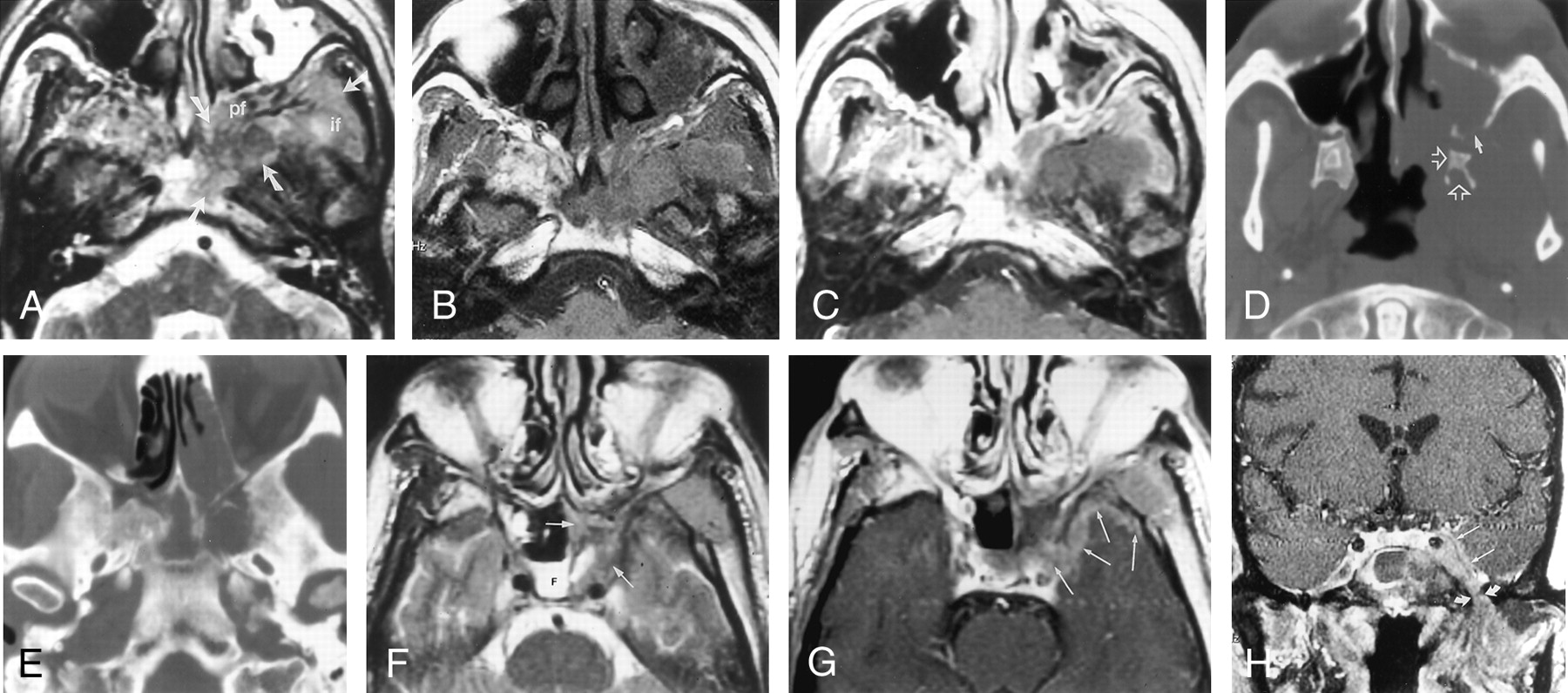
Images from the case of a 53-year-old man who developed B-cell lymphoma in the paranasal sinuses, with extension to the skull base after lung transplantation.
A, Axial view fast spin-echo T2-weighted (4000/80[TR/TE]) MR image, obtained at the base of the skull, shows abnormal hypointense tissue (arrows) involving the clivus, pterygopalatine fossa (pf), and infratemporal fossa (if).
B, Axial view unenhanced T1-weighted (500/9) MR image, obtained at same level as that shown in A, shows that the abnormal tissue is slightly hyperintense to muscle.
C, Corresponding contrast-enhanced axial view T1-weighted (600/20) MR image shows no central or solid enhancement of the lesion.
D, Axial view CT scan, obtained at the level of the pterygoid and superior maxillary sinus, shows osseous erosion of the posterior left maxillary sinus wall (solid arrow) and abnormality of the left pterygoid bone (open arrows).
E, Axial view CT scan, obtained at the level of the skull base, shows erosion of the inferior sphenoid sinus/basisphenoid.
F, Axial view fast spin-echo T2-weighted (2500/85) MR image shows fluid (F) in the right sphenoid sinus and hypointense tissue (arrows) in the left sphenoid sinus.
G, Axial view contrast-enhanced T1-weighted (600/20) MR image, obtained at the same level as that shown in F, shows peripheral enhancement of the tissue in the left sphenoid sinus and enhancing tissue in and along the lateral dural margin of the left cavernous sinus and the anterior aspect of the left middle cranial fossa (arrows).
H, Coronal view contrast-enhanced T1-weighted (700/14) MR image shows abnormal tissue along the ventral margin of the cavernous sinus (straight arrows), just anterior to Meckel’s cave and extending through the foramen ovale (curved arrows) into the masticator space.
Although invasive fungal sinusitis was strongly suspected, considering the patient’s transplant history, lymphoproliferative disorder was also considered. As a result, emergent endoscopic sinonasal surgery was performed and revealed a tan-white mass in the sphenoid sinus and posterior ethmoid air cells. Histology revealed a lymphoid infiltrate composed of highly atypical medium-to-large cells with prominent nucleoli. Flow cytometry was consistent with immunoblastic B-cell lymphoma with plasmacytic differentiation. In situ hybridization for EBER-1, an RNA sequence expressed during latent Epstein-Barr virus infection, was positive. The results of subsequent CT of the chest, abdomen, and pelvis were unremarkable.
Management consisted of emergent radiation therapy and a reduction in the patient’s immunosuppressive therapy (the tacrolimus was reduced and the mycophenolate discontinued). After 1 month, the patient’s proptosis was significantly reduced and there was some improvement in his trigeminal neuralgia and the vision in his left eye. The left IIIrd and VIth cranial nerve palsies were unchanged. However, follow-up MR imaging showed progression of the mass in the infratemporal fossa and extension of disease into the nasopharynx. There was increased tissue in the left cavernous sinus and orbit. The patient was also noted to have multiple subcutaneous thoracic and abdominal wall masses, in addition to a right lung nodule. Excisional biopsy of a subcutaneous nodule revealed non-Hodgkin lymphoma, identical to that in the patient’s paranasal sinuses. Because the patient had progressive disease despite reduction of his immunosuppressive regimen, he was treated with an experimental anti-B lymphocyte monoclonal antibody (rituximab) and experienced complete clinical response. Continued follow-up imaging revealed stable, nonprogressive disease. The cranial nerve palsies had resolved, with the exception of a persistent left VIth nerve palsy and mild left facial numbness.
Discussion
Rapidly progressive cranial nerve palsies in an immunocompromised patient necessitate prompt medical attention. Cross-sectional imaging is required to characterize the lesion and document the extent of disease. The presence of hypointense tissue in the paranasal sinuses in this situation is highly suspicious for invasive fungal sinusitis. The clinical presentation of fungal disease is dependent on the sinus(es) involved and the presence of disease extension outside the sinuses into adjacent structures. The decreased signal intensity on T2-weighted MR images (which may mimic an aerated sinus) is due to the presence of ferromagnetic compounds within fungal concretions, including iron, manganese, and calcium (5). Fulminant invasive fungal sinusitis is characterized by osseous necrosis and rapid spread to the skull base and orbits, often leading to visual disturbances and cranial nerve palsies (5). Intracranial extension may result from direct extension from the paranasal sinuses, perineural spread, or hematogenous dissemination. Invasive mucormycosis and aspergillosis have an affinity for invading blood vessels and spreading along the internal elastic lamina of these vessels, often inducing thrombosis (6). Definitive diagnosis requires endoscopy and demonstration of fungal elements within the mucosa, submucosa, or bone of the sinonasal cavity. Because the infection can be fatal in a matter of hours to days, early diagnosis and treatment, including systemic antifungal antibiotics and radical surgical debridement, are critical.
In addition to invasive fungal disease, our case illustrates that PTLD may also present as an aggressive mass that is hypointense on MR images (Fig 1A and F). A high index of suspicion is required to establish the diagnosis of PTLD, which should be considered when organ rejection or opportunistic infection is suspected in a transplant recipient (3). PTLD has been reported to affect 1% to 10% of organ transplant recipients, the incidence dependent on both the type of organ transplanted and the immunosuppressive regimen (1, 7, 8). The prevalence of PTLD is highest in patients after lung transplant, followed in decreasing order of frequency by kidney-pancreas, heart, and liver transplants (8). Clinical presentation may occur as early as 1 month or as late as 10 years or more after transplantation (1). Patients may be asymptomatic or may present with a mononucleosis-type illness, widely disseminated disease, or sepsis (3).
Epstein-Barr virus is frequently associated with the pathogenesis of PTLD, as was the case with our patient (9). Epstein-Barr virus infection may represent reactivation of latent virus or primary infection in patients who are seronegative before transplantation (which has been associated with an increased risk of developing PTLD) (8). The virus infects B-lymphocytes and epithelial cells in the aerodigestive tract. Cytotoxic T cells are targeted to Epstein-Barr virus antigens, thereby serving as the immunosurveillance in controlling the proliferation of Epstein-Barr virus-infected cells (10). Immunosuppressed transplant recipients have impaired T-cell immunity and therefore may be unable to prevent virus-induced B-cell proliferation.
On MR images, lymphoid proliferations are frequently iso- to hypointense to brain on T1- and T2-weighted MR imaging sequences because of dense cellularity. Cross-sectional imaging of aggressive sinonasal pathologic abnormality is critical in assessing the extent of disease. The multiplanar capabilities and improved tissue resolution inherent to MR imaging make it the choice imaging modality in distinguishing abnormal tissue and neoplasm from sinonasal secretions and coexistent inflammatory disease (11) and in identifying skull base invasion and intracranial extension (Fig 1). CT allows superior delineation of the bone structures comprising the paranasal sinuses, orbits, and skull base (12).
Definitive diagnosis of PTLD requires histopathologic examination of tissue (1, 3). Management almost always includes a reduction in immunosuppressive therapy. Usually chemotherapy or irradiation is also necessary for disseminated or locally advanced disease, respectively. Antiviral agents such as acyclovir and gancyclovir have had limited usefulness in the treatment of PTLD and may have more impact as prophylaxis (1, 3, 9). Even with treatment, the mortality rate from PTLD is >50% (1, 3, 13). Considering this, the focus of new treatments has been on immunomodulation with the use of anti-B lymphocyte monoclonal antibodies (rituximab), alpha-interferon, and the transfusion of cytotoxic T-cells (1, 13). Benkerrou et al (13) reported complete remissions in 64% of patients treated with anti-B lymphocyte monoclonal antibodies. At the time of this writing, our patient, too, had experienced complete response.
This case illustrates that in addition to invasive fungal sinusitis, PTLD must be considered in the differential diagnosis of a transplant recipient who is receiving chronic immunosuppressive therapy and who presents with aggressive sinonasal disease. Prompt clinical evaluation is required because the emergent management of these two entities is vastly different and because there is a high mortality rate associated with both of these diseases.
Footnotes
This work was supported by the Radiological Society of North America Scholars Grant.
References
- Received October 11, 2001.
- Accepted after revision November 9, 2001.
- Copyright © American Society of Neuroradiology





{kind=link}