
Abstract
BACKGROUND AND PURPOSE: MR sialography has become an alternative imaging technique for ductal salivary gland diseases. We compared the diagnostic accuracies of MR sialography and digital subtraction sialography in patients with successful completion of both examinations and benign salivary gland disorders.
METHODS: In a prospective study, we attempted to examine salivary glands in 80 patients with clinically suspected diagnoses of sialadenitis and/or sialolithiasis. Each patient underwent digital subtraction sialography and MR sialography. MR sialography was obtained with a T2-weighted single-shot turbo spin-echo sequence (TR/TE 2800/1100 msec, acquisition time 7 seconds), with use of a quadrature head coil. Final diagnoses were confirmed by clinical follow-up and results of biopsy (n = 9) or surgery (n = 19).
RESULTS: Failure rate was 5% (four of 80) for MR sialography and 14% (11 of 80) for digital subtraction sialography. Eighty-one salivary glands (48 parotid, 33 submandibular) in 65 patients were successfully visualized with both modalities. MR sialography depicted the main ductal system and first- and second-order branches, whereas digital subtraction sialography was able to depict third-order branches. Sensitivity and specificity to diagnose chronic sialadenitis were 70% and 98% with MR and 96% and 100% with digital subtraction sialography. MR sialography enabled diagnosis of sialolithiasis with a sensitivity of 80% and a specificity of 98% versus 90% and 98% for each with digital subtraction sialography.
CONCLUSION: MR sialography with a heavily T2-weighted sequence is highly successful in the noninvasive visualization of the ductal system of major salivary glands. It is useful for diagnosing sialolithiasis and sialadenitis. Digital subtraction sialography, an invasive technique, had a substantial procedural failure rate, particularly for the submandibular duct. However, because of its higher spatial resolution, successfully completed digital subtraction sialography achieved superior diagnostic information compared with that of MR sialography.
Conventional or digital subtraction x-ray sialography has been used for investigating the ductal system of major salivary glands. Imaging is performed to delineate inflammatory or obstructive changes within the ductal system of parotid and/or submandibular glands. This technique requires cannulation of the duct, instillation of contrast material, and exposure to radiation (1, 2). However, this invasive technique also enables a therapeutic approach to remove sialiths and/or to dilate strictures (3). Improvement in cross-sectional imaging techniques (US, CT, and MR imaging) has reduced the indications for x-ray sialography in recent years (2, 4–6). However, sialectasis, radiopaque sialiths, and postinflammatory ductal strictures continue to be best visualized with digital subtraction sialography (7, 8). US, like CT and MR imaging, has the advantage of depicting the glandular parenchyma in addition to depicting sialolithiasis and changes of the ductal structure. Therefore, all three methods are standard procedures for the diagnosis of suspected salivary mass or the visualization of parenchymal lesions (4, 7, 9, 10).
MR imaging enables visualization of static liquids in tubular structures with use of heavily T2-weighted sequences. This technique has been largely applied for MR cholangiopancreaticography and MR urography (11, 12). Feasibility of visualizing ductal structures of major salivary glands by application of this technique has been demonstrated in recent studies (13, 14). Advantages of MR sialography are rapid acquisition times, noninvasiveness, and the possibility to visualize all major salivary glands without further positioning of the patient (15).
We sought to evaluate the accuracy of MR sialography with heavily T2-weighted sequences by comparing this technique with the standard procedure of digital subtraction sialography in patients suspected of having ductal changes of parotid or submandibular glands.
Methods
Study Population
Between July 1998 and November 1999, 80 consecutive patients were referred for salivary duct visualization from the department of otorhinolaryngology because of clinically suspected sialadenitis or sialolithiasis. Diagnosis was based on clinical symptoms and US findings since all patients underwent routine US examination in the department of otorhinolaryngology. All patients had swelling and/or pain of one or more salivary glands. Indication for digital subtraction sialography was to verify sialolithiasis or inflammatory ductal changes. Patients suspected of having sialadenitis were investigated only if all clinical signs of acute inflammation had disappeared. The institutional review board had approved the study protocol. Written informed consent was obtained from all patients.
MR imaging of the salivary ductal system and digital subtraction sialography were attempted in all 80 referred patients. However, 15 patients had to be excluded from the study. In two patients, MR imaging could not performed because of severe claustrophobia (n = 1) or contraindication for MR imaging (pacemaker, n = 1). Another two patients were excluded because it was impossible to visualize the ductal system, although multiple attempts were made. Therefore, the failure rate for successful MR sialography on an intention-to-treat basis was 5% (four of 80). In eleven other patients, digital subtraction sialography was not possible because we failed to cannulate the orifice of the ductal system. This occurred more often in the attempted cannulation of the Wharton duct (n = 8) than in the attempted cannulation of the Stensen duct (n = 3). Therefore, the failure rate for attempted digital subtraction sialography was 14% (11 of 80). The remaining 65 patients (only those with successful digital subtraction and MR sialography) were enrolled in the prospective study and represent the study population.
All 65 patients underwent MR sialography and digital subtraction sialography on the same day at our institution. There were 34 male and 31 female patients with a mean age of 47 years (age range, 9–78 years). In the 65 patients undergoing both examinations, a total of 81 glands were examined (33 submandibular and 48 parotid glands). In 51 patients, the clinicians requested visualization of a single glandular duct (30 parotid and 21 submandibular ducts); in 13 patients, two ducts were examined (both parotid glands in seven, both submandibular glands in five, and a submandibular and a parotid gland in one patient); and in one patient, all four ducts were investigated. The final diagnosis in each patient was made by the referring physician from the department of otorhinolaryngology and was based on consensus of clinical follow-up and biopsy or surgery results. All patients underwent follow-up that consisted of clinical and US examinations in the department of otorhinolaryngology. Nineteen patients underwent open surgery with histopathologic evaluation of resected tissue, and nine additional patients underwent percutaneous needle aspiration biopsy with cytopathologic examination.
MR Sialography
First, patients were examined with MR sialography, which was carried out with a 1.0-T clinical MR imager (Magnetom Expert; Siemens, Erlangen, Germany) by using a quadrature head coil. Images were obtained with a manufacturer-provided single-shot turbo spin-echo sequence (TR/TE 2800/1100 ms, flip angle 150°, accquisition time 7 seconds, field of view 169 mm, matrix 240 × 256). This sequence obtains a single section with a thickness of 40 mm and in-plane resolution of 0.7 x 0.66 mm. In case of parotid disease, a transverse reference image covering the complete volume of the head was obtained. Sagittal oblique sections were planned on this reference image. For localization of the submandibular glands, a sagittal reference image was used. The final imaging plane for submandibular glands was transverse oblique. In all cases, the contralateral salivary gland was visualized and served as a control. To enhance the visualization of the ductal structures, we stimulated salivation by intraoral application of a lemon mouth swab (Appli-Lem; Applimed, Chatel-St.-denis, Switzerland). Because of the short acquisition time of 7 seconds, multiple (usually three to five) images were obtained before and after stimulation. No standard MR examination of the salivary glands (ie, regular spin-echo or gradient echo T1-weighted and T2-weighted imaging) was performed in this patient population. Immediately after MR sialography, patients were transferred to the angiography suite where digital subtraction sialography was carried out.
Digital Subtraction Sialography
This technique is described in detail elsewhere (16). Briefly, the patient is placed supine with the head in a headrest. After identification of the orifice of the Stensen or Wharton duct, the orifice is cannulated with an appropriate dilator (0.016 inches for the Wharton duct, 0.035 inches for the Stensen duct). In patients whose ducts were difficult to identify, salivation was stimulated by using a lemon mouth swab (especially for cannulation of the Wharton duct). After predilation, a Rabinov catheter (Cook Europe, Bjaeverskov, Denmark) was introduced (0.016 inches for the Wharton duct, 0.032 inches for the Stensen duct). Digital subtraction images were obtained during injection of 0.5–2 mL of nonionic iodinated contrast material (iopamidol 300 mg I/mL [Solutrast; Bracco-Byk Gulden, Konstanz, Germany]). Contrast material was injected until complete filling of intraglandular ductal structures was noted during the digital subtraction run.
Image Interpretation
Both digital subtraction and MR sialograms were independently interpretated by experienced investigators (M.K. for digital subtraction sialography, H.J.W. for MR sialography) without knowledge of the results of the other examination, US findings, and/or surgical results at the time of image interpretation. Sialoliths were diagnosed on MR images when round or irregularly shaped signal voids were identified within or immediately next to dilated or nondilated salivary ducts. Chronic sialadenitis, including duct stenoses and sialectasis, was diagnosed when an abrupt transition from dilated ducts to an area of signal void, a tapered salivary duct, or areas of considerable narrowing of ducts were seen. In the absence of ductal dilatation, failure of visualization of the entire length of the main salivary duct was not considered to reveal a stenosis but rather a tiny normal duct. Images were interpreted as normal if no sialiths, no ductal dilatation, no cystic structures, and no tumor were seen.
Statistical Analysis
The MR and digital subtraction sialographic findings were compared with the final diagnoses. Sensitivity, specificity, and positive and negative predictive values for the detection of the three most frequent diagnoses (sialolithiasis, chronic sialadenitis, and status post acute sialadenitis) were calculated. All data were calculated for the number of investigated glands.
Results
Digital subtraction sialograms depicted the main salivary duct and intraglandular ducts up to tertiary branches. MR sialograms delineated the ductal structures much more clearly after stimulation of salivation with a lemon mouth swab (Fig 1). However, MR sialograms clearly demonstrated the main duct and primary branching ducts, but failed to demonstrate secondary branches in most, and tertiary branches in all cases owing to limited spatial resolution as opposed to digital subtraction sialograms (Fig 1).

A and B, Normal heavily T2-weighted turbo spin-echo (2800/1100 ms, flip angle 150°, acquisition time 7 seconds) MR sialograms obtained before (A) and after (B) salivation stimulation in a patient with status post acute parotiditis. Stensen duct (arrowheads in B) is better delineated after stimulation of salivation with a lemon mouth swab than before salivation stimulation.
The most frequent diagnosis in this patient population was chronic sialadenitis, which was present in 28 salivary glands (20 parotid glands and eight submandibular glands). Fig 2 demonstrates an example of chronic sialadenitis depicted on the digital subtraction sialograms as compared with the MR sialogram in the same patient. Twenty-four glands (17 parotid glands and seven submandibular glands) showed clinical signs of acute sialadenitis; these patients underwent antibiotic therapy and had an uneventful course thereafter. No abnormal findings were noted at follow-up US examination, and our MR and digital subtraction sialographic studies were unremarkable (Fig 3). Eleven glands (four parotid and seven submandibular) were finally found to have sialolithiasis (Fig 4). In seven patients with nonspecific pain and/or swelling of a salivary gland and without abnormal changes at MR sialography and digital subtraction sialography, the clinical follow-up after sialography showed no abnormal findings. In these patients, no therapy was undertaken. High-grade stenoses of the Stensen duct were diagnosed in three patients. All these strictures were treated with transluminal dilation. In eight further investigated glands, the final diagnosis was not attributable to the salivary duct system, but revealed parenchymal cystic lesions (n = 2), hyperplasia of the masseter muscle (n = 2), sarcoidosis (n = 2), lymphadenitis (n = 1), and cystadenolymphoma (n = 1).

59-year-old man with a history of chronic sialadenitis of the left parotid gland.
A, Lateral digital subtraction sialogram shows multiple strictures, sialectasis, and prestenotic dilatation of the Stensen duct (arrows) and also of secondary and tertiary branching intraglandular ducts (arrowheads).
B, Lateral MR sialogram shows the same abnormal findings but at lesser spatial resolution. Subtle strictures are more difficult to visualize and sialectasis is not as prominent (arrow). The enlargement of the ductal system is demonstrated up to secondary branching ducts.

61-year-old woman with status post acute sialadenitis.
A and B, Oblique sagittal-coronal MR sialogram (A) and lateral digital subtraction sialogram (B) reveal normal ductal anatomy without abnormal findings. However, due to higher spatial resolution, the digital subtraction sialogram shows better delineation of ductal morphology and enables visualization of peripheral intraglandular ductal branches. Because of its normal small size, the Stensen duct shows some focal signal voids in A (compare with the enlarged duct in Fig 2B).
64-year-old man with a large sialith in the main parotid duct.
A, Lateral digital subtraction sialogram depicts a solid calculus in the proximal portion of the Stensen duct (arrow) and a prestenotic dilatation of intraglandular ductal structures (arrowheads). However, because of the near total obstruction of the main duct, visualization of prestenotic intraglandular structures is limited.
B, MR sialogram (oblique sagittal to coronal view) compares favorably with the digital subtraction sialogram and shows a filling defect of the proximal main parotid duct (arrow) together with prestenotic dilatation of intraglandular ducts. However, because of surrounding fluid, the single calculus on the MR sialogram could be misinterpreted as two separate stones. This patient was successfully treated with extracorporal lithotripsy.
For the three most frequent diagnoses (chronic sialadenitis, post acute sialadenitis, and sialolithiasis) sensitivity, specificity, and positive and negative predictive values for MR sialography and digital subtraction sialography are tabulated in Table 1.
Diagnostic Discrimination for MR Sialography and Digital Subtraction Sialography for the Three Most Frequent Diagnoses
Sensitivity and specificity of MR sialography for diagnosing chronic sialadenitis were 70% and 98%, respectively. Eight false-negative results were noted owing to lower spatial resolution of MR sialography as opposed to that of digital subtraction sialography. Subtle changes in secondary and tertiary branching ducts were not depicted on MR sialograms, but were visible on the digital subtraction sialograms. Sensitivity and specificity of digital subtraction sialography for the diagnosis of chronic sialadenitis were 96% and 100% (no false-negative results). Positive and negative predictive values were 95% and 86%, respectively, for MR sialography, but 100% and 98% for digital subtraction sialography. However, one has to take into account that four of 80 MR examinations failed and 11 of 80 digital subtraction examinations failed.
Patients with acute sialadenitis underwent imaging after all clinical signs of acute inflammation had completely disappeared. MR and digital subtraction sialography uniformly showed a normal ductal system in all glands. Therefore, calculated sensitivity and specificity were each 100% for both imaging modalities.
Sensitivity and specificity of MR sialography for detection of sialolithiasis were 80% and 98%, whereas digital subtraction sialography achieved 90% and 98%, respectively. Positive and negative predictive values were 89% and 97% for MR sialography, but 90% and 98% for digital subtraction sialography. In two cases, MR sialography showed false-negative results due to small nonobstructing sialiths. In one patient, chronic sialadenitis in a parotid gland was misdiagnosed with both modalities. However, surgical removal of the gland revealed a proximal duct stone in the main parotid duct.
In a second approach, we calculated sensitivity, specificity, and positive and negative predictive values for the three most frequent diagnoses according to the investigated gland (parotid vs submandibular gland). The results are summarized in Table 2.
Diagnostic Discrimination for MR Sialography and Digital Subtraction Sialography for the Three Most Frequent Diagnoses Stratified for the Investigated Gland
Sensitivity and specificity of digital subtraction sialography for the diagnosis of chronic sialadenitis in the parotid gland were each 100%. Sensitivity and specificity of MR imaging for diagnosing chronic sialadenitis of the parotid glands were 79% and 96%, respectively (four false-negative and one false-positive results were noted in the parotid gland). Positive and negative predictive values for MR sialography were 79% and 88% as compared with 100% and 100% for digital subtraction sialography.
In the submandibular gland, sensitivity and specificity of digital subtraction sialography for the diagnosis of chronic sialadenitis were 88% and 100% compared with 50% and 100% for MR sialography. Positive and negative predictive values for digital subtraction and MR sialography were 100% and 96%, and 100% and 86%, respectively, (four false-negative results were obtained with MR sialography, one false-negative result with digital subtraction sialography). As stated above, MR and digital subtraction sialography enabled correct diagnosis in all cases of status post acute sialadenitis, revealing a uniform 100% sensitivity, specificity, and positive and negative predictive values for both modalities in both glandular ducts.
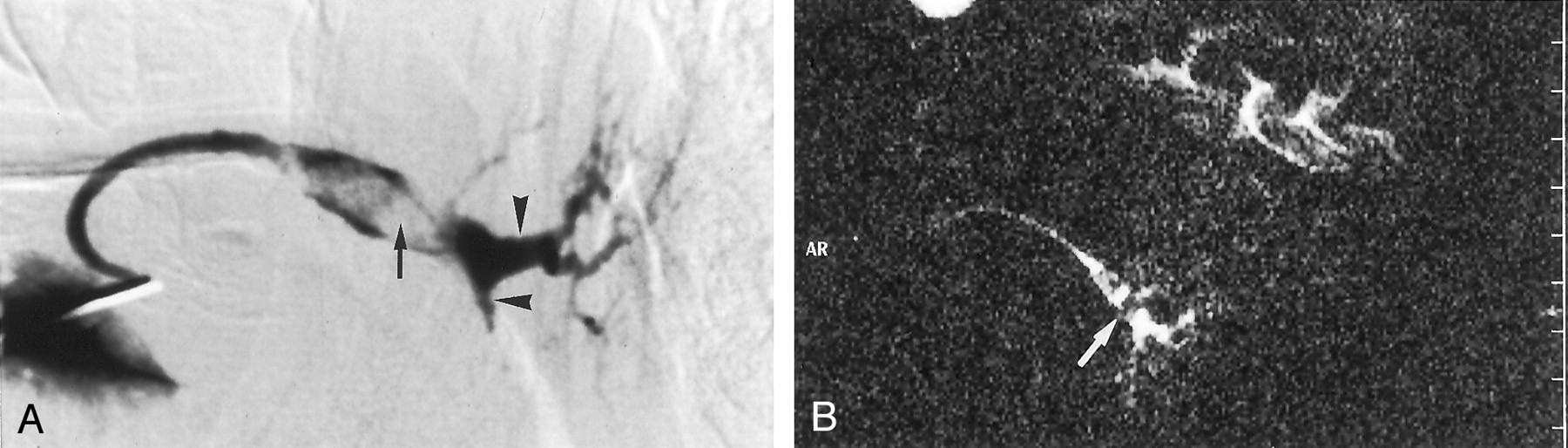
Sensitivity and specificity of MR sialography and digital subtraction sialography for the diagnosis of sialolithiasis in the parotid gland were 100% and 98% for both modalities. Positive and negative predictive values were also 75% and 100% for MR and digital subtraction sialography. Fig 5 shows an example of a false-negative digital subtraction study for parotid sialolithiasis. MR sialography demonstrated the calculus correctly. For the submandibular gland, sensitivity for sialolithiasis was 71% for MR sialography and 86% for digital subtraction sialography. MR sialography revealed two false-negative studies; digital subtraction dialography, one false-negative study. Therefore, the negative predictive value was 93% for MR sialography and 96% for digital subtraction sialography.
36-year-old patient suspected to have sialolithiasis.
A, Lateral digital subtraction sialogram shows a slightly dilated Wharton duct (arrow) and sialectasis in secondary duct branches (arrowhead). No filling defect in the main duct is seen.
B, Transverse MR sialogram shows a filling defect near the orifice of the left Wharton duct (arrow). Note also the markedly dilated left Wharton duct compared with the right side. Patient underwent surgery, and a sialith was confirmed. The false-negative digital subtraction sialographic result may be due to dental hardware or to the fact that the sialographic catheter already passed the distal stone.
In three patients, both modalities depicted high-grade stenoses of the main ductal system (Stensen duct) due to inflammation. All three strictures were successfully treated with peroral transluminal dilation. Two other patients had intraparenchymal cystic lesions. MR sialography enabled visualization of the cystic lesion in one case. Digital subtraction sialography showed a normal ductal anatomy and could help rule out connection of the cystic lesion with the ductal system but was not able to depict the lesion itself (Fig 6). This diagnosis was confirmed by histopathologic examination after surgical gland removal. Another patient had a hemorrhagic cystic mass lesion with a diameter of 15 mm, which was detected at US. Both MR and digital subtraction sialography showed no abnormal findings. In five other glands, MR and digital subtraction sialography showed no abnormal ductal changes. In these patients, the final diagnosis was hyperplastic masseter muscle (n = 2), enlarged cervical lymph nodes (n = 1), a cystadenolymphoma (n = 1), or sarcoidosis (n = 1). Another seven patients presented primarily with pain and a history of swelling in salivary gland regions. No definite diagnosis could be made during initial clinical examination. In all these patients, MR and digital subtraction sialography revealed no abnormal changes. These patients underwent no specific therapy and had a normal and uneventful clinical course during follow-up.

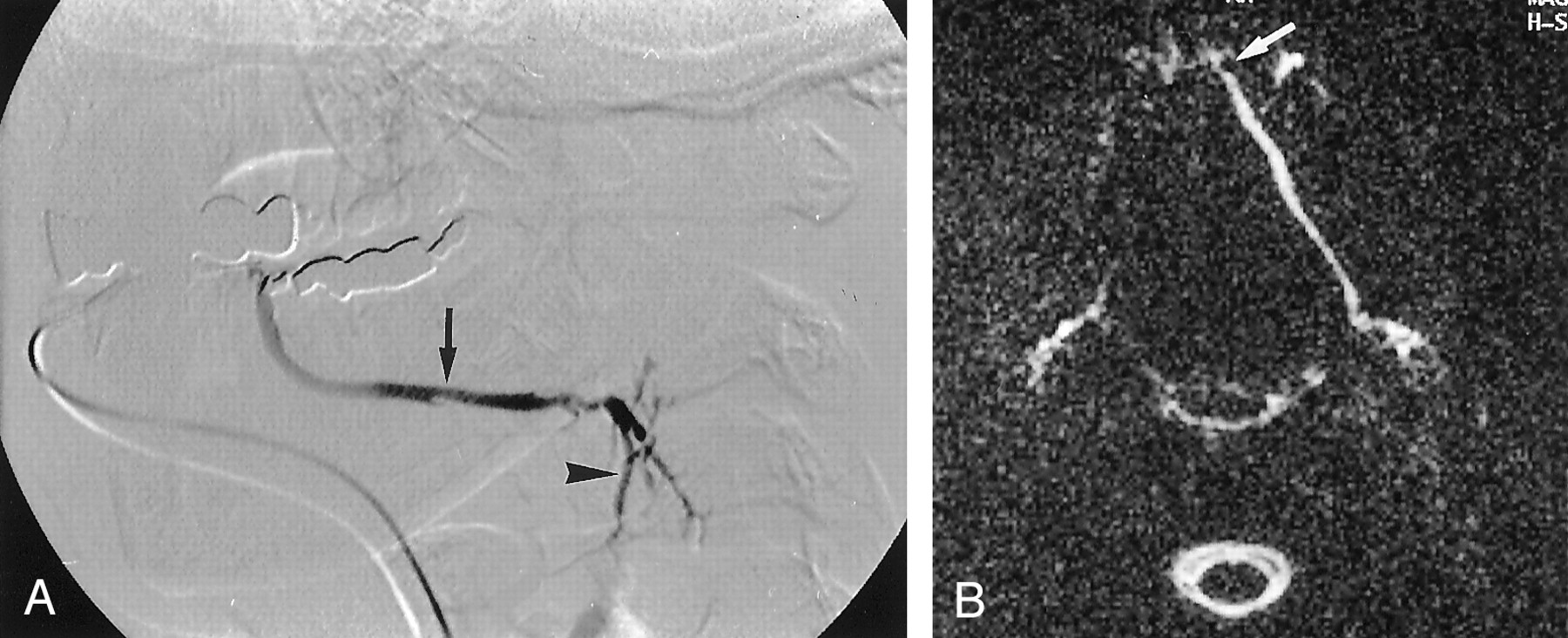
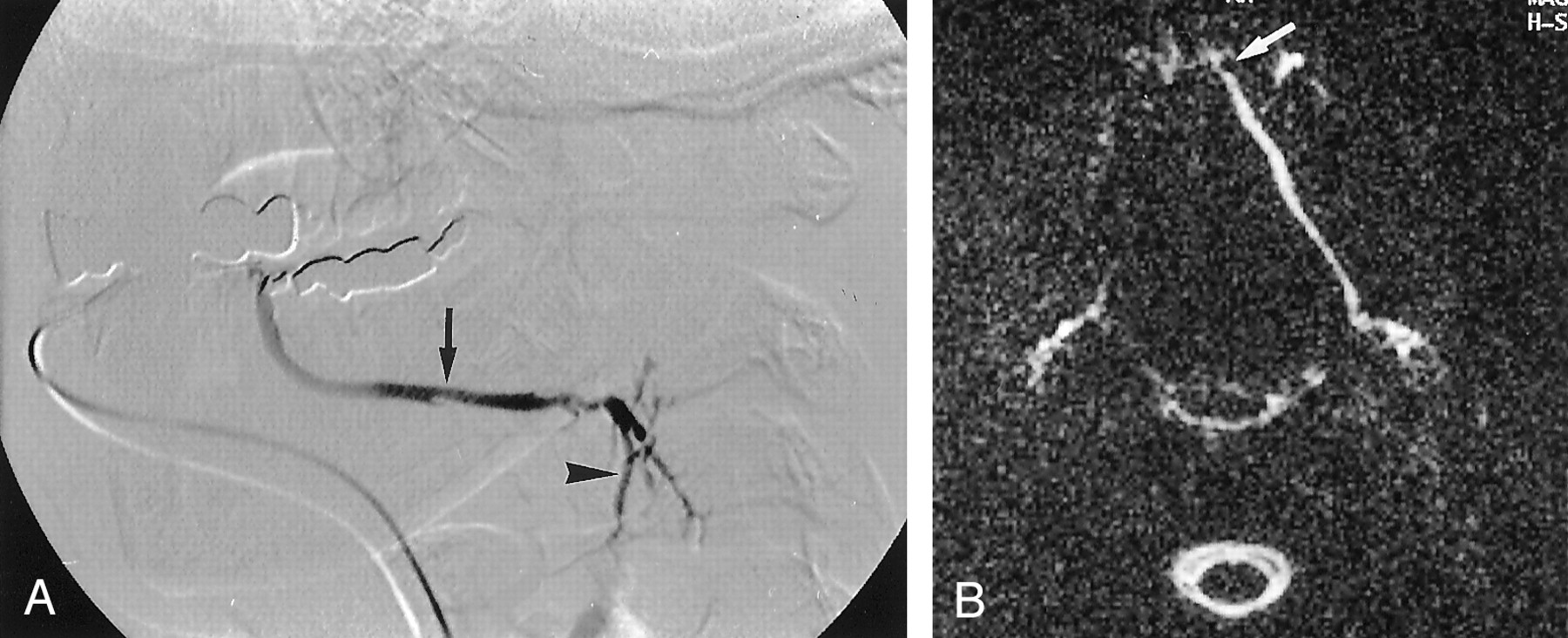
55-year-old patient suspected to have an intraparenchymal cyst.
A, Oblique sagittal-coronal MR sialogram shows a fluid-filled cystic mass lesion (arrows) in the lower parotid parenchyma.
B, Lateral digital subtraction sialogram shows no connection between the ductal structures and the cyst. However, displacement of the lower pole ducts is depicted (arrow).
Discussion
Our study revealed good performance of MR sialography in the diagnosis of chronic sialadenitis and sialolithiasis. However, results were superior for digital subtraction sialography in those with evaluable studies. One has to take into account that four of 11 attempted MR sialographic examinations failed (two patients presented contraindications to MR imaging, and in two patients there was not enough fluid in the ductal system to enable sufficient visualization), whereas 11 of 80 digital subtraction sialographic examinations failed for technical reasons regarding cannulation of the duct. With regard to the investigated gland, delineation of the ductal structures of the parotid gland achieved higher sensitivity and specificity rates for chronic sialadenitis and sialolithiasis with both imaging modalities than for the submandibular gland.
The indication for conventional or digital subtraction sialography is the diagnosis of chronic inflammation that results in duct strictures, sialectasia, and sialolithiasis. X-ray sialography, one of the standard imaging procedures, provides a high spatial resolution and is the only imaging technique to examine subtle salivary duct abnormalities, but it also has major disadvantages, including radiation exposure and requirement for injection of iodinated contrast material. Adverse reactions to iodinated contrast material after sialography have been reported (17). Duct cannulation requires a skill, especially in patients with duct strictures or stones close to the orifice. However, technical success rates exceed 90% in some series (18), but in our trial the failure rate was substantial (14% [11 of 80]), especially for the submandibular duct. Even experienced investigators may find it impossible to cannulate orifices, and cannulation may result in duct damage. Furthermore, because of the necessity to cannulate the duct to enable filling of the more distal ductal structures, strictures close to the orifice can be hidden. Overfilling can cause pain and damage to parenchymal structures. In addition, retrograde injection of microorganisms may result in a gland infection or displacement of an anteriorly placed ductal stone into a position in which retrieval by means of endoscopy or intraoral surgery becomes more difficult.
US, used as a first-line examination in many institutions, has high accuracy for detecting sialiths and ductal dilatation (19), but is less accurate than nonenhanced thin-section CT in the differentiation of multiple intraparenchymal duct stones from large single stones (8). Typically, CT should be performed without administration of contrast material, since small opacified blood vessels may simulate small sialoliths. However, adding contrast material may be helpful to detect suspected abscesses or inflammatory changes (8). In some cases, sialiths are nonradiopaque at CT and may be missed during examination (1). Another disadvantage of CT is the necessity of ionizing radiation and resultant artifacts due to dental hardware, especially for submandibular gland examinations.
The MR sialographic technique with heavily T2-weighted images for depiction of static or nearly static fluids obtains a two-dimensional projection image of ductal structures similar to that of digital subtraction sialography. Several publications have reported the use of MR sialography in the examination of healthy volunteers and small patient populations (13, 14, 20–22). Lomas et al (20) investigated three patients with a rapid acquisition with repeated echoes, or RARE, sequence by using a quadrature head coil. However, the reported experience for pathologic conditions were limited in this study. In our study, sensitivity for diagnosing sialolithiasis by using MR sialography was 80%, whereas digital subtraction sialography achieved a rate of 90%. These findings are in accordance with the results of Varghese et al (23), who found that MR sialography alone was not sensitive in the diagnosis of sialolithiasis in their patient population. In MR imaging, the diagnosis of sialolithiasis is based on indirect signs (ie, areas of complete obstruction with signal void and prestenotic dilatation). Therefore, small nonobstructing duct stones will be missed in most cases. Specially, sialiths close to the orifice or located in smaller intraglandular ducts are difficult to diagnose with MR sialography. However, it is questionable whether nonobstructing stones cause clinical symptoms. The major drawback of MR imaging is its insensitivity to calcium detection. However, contrary to CT imaging, artifacts due to dental hardware or other prostheses have not been noted with the used MR sialographic technique.
A recent study with a 3D extended phase conjugate symmetry rapid spin-echo, or EXPRESS, MR imaging sequence yielded excellent results for the diagnosis of sialolithiasis and salivary ductal stenosis (24). The use of this single-shot fast spin-echo sequence with half-Fourier analysis (acquisition time 5–6 minutes) achieved sensitivity and specificity of 91% and 94%, respectively, for sialolithiasis, and of 100% and 93%, respectively, for detection of ductal strictures. The results of this trial are superior to the results obtained in our study for MR sialography. A reason for the different results may be the sequence used for MR sialography in the study by Becker et al (24), which achieves a higher spatial resolution, but requires longer acquisition times. However, we tried longer sequences in the first patients that underwent MR sialography at our institution and encountered problems due to motion artifacts. An advantage of the single-shot turbo spin-echo sequence used in our study is the extremely short acquisition time of 7 seconds. Further trials will define which sequence provides the best diagnostic results in a nonselected patient population with salivary gland disorders.
Although our experience with pathologic findings is still limited to small patient populations, MR sialography seems to be a promising noninvasive technique for the detection of ductal abnormalities in major salivary glands. The most obvious advantage of this technique is the fact that images can be obtained without use of ionizing radiation, as well as its noninvasiveness. No contrast material has to be injected, and images can be obtained with short acquisition times of less than 10 seconds. Contralateral salivary glands can be easily visualized without further positioning of the patient and can serve as controls. Images can be obtained with use of standard protocols and do not require an experienced examiner. Contraindications for digital subtraction sialography such as acute sialadenitis are not contraindications for MR sialography. Ductal structures can also be visualized in cases of complete obstruction of the ductal system. Also, additional cross-sectional images of the glandular parenchyma can be obtained by using conventional T1- and T2-weighted sequences. Furthermore, MR sialography has an excellent sensitivity for visualization of edema in the salivary parenchyma, which is more difficult to diagnose with CT.
Limitations of the MR sialographic technique include low spatial resolution due to the extremely short acquisition time, which prevents detection of subtle and moderate changes in secondary and tertiary branching ducts in chronic sialadenitis. MR sialography is also inferior to digital subtraction sialography in the diagnosis of chronic inflammatory changes. The limited spatial resolution of static images makes it very difficult to distinguish between complete and partial obstructions of the ductal system. Therefore, in cases of suspected ductal obstructions, additional thin cross-sectional images through the Stensen or Wharton duct are indicated.
In conclusion, our results show that MR sialography with a heavily T2-weighted sequence is a promising diagnostic tool and carries the potential to replace invasive imaging methods like x-ray sialography in patients suspected of having sialadenitis and/or sialolithiasis. However, the lower spatial resolution of MR sialography requires further technical developments and refinements to achieve similar sensitivity and specificity to that of conventional x-ray sialography. At this time, depiction of subtle anomalies like early stage sialadenosis and small, nonobstructing sialiths is limited.
Overall, digital subtraction sialography continues to be the standard technique for imaging the extra- and intraglandular duct system. If acute sialadenitis is present or insertion of a cannula is not successful, an alternative imaging method is needed. In such cases, noninvasive MR sialography provides an excellent alternative. However, in the case of a subacute manifestation of a painful, noninflammatory mass, in which there is a high degree of suspicion for neoplasm, additional contrast-enhanced MR imaging will best demonstrate the extent of disease.
References
- Received May 17, 2001.
- Accepted after revision April 24, 2002.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- MR Imaging of the Extracranial Facial Nerve with the CISS Sequence
- Salivary gland swellings
- Radiation-Induced Xerostomia: Objective Evaluation of Salivary Gland Injury Using MR Sialography
- MR sialography: the effect of a sialogogue and ductal occlusion in volunteers
- Lipiodol ultra-fluid - foreign body in the cheek
- Salivary duct strictures: nature and incidence in benign salivary obstruction