
Abstract
Summary: We present the case of an infant with medulloblastoma with extensive nodularity, which had been called cerebellar neuroblastoma. MR imaging clearly revealed a nodular enhancement, which appeared as a grape-like lesion. Single photon emission CT revealed markedly high iodine-123 metaiodobenzylguanidine uptake in the enhancing tumor. Iodine-123 metaiodobenzylguanidine single photon emission CT may be useful in the diagnosis of medulloblastoma with extensive nodularity, which has been considered to be a subgroup of medulloblastoma with extensive neuronal differentiation.
Medulloblastoma with extensive nodularity is a rare brain tumor, which had been called cerebellar neuroblastoma. Recently, Giangaspero et al (1) reported 11 cases of this tumor type and adopted the descriptive term medulloblastoma with extensive nodularity instead of cerebellar neuroblastoma to avoid confusion with supratentorial primitive neuroectodermal tumor known as cerebral neuroblastoma. This distinct variant is associated with apparently more favorable outcomes than is classic medulloblastoma. Contrast-enhanced MR imaging revealed this tumor to have a nodular enhancing grape-like appearance and clearly depicted tumor extension (1, 2). Recently, it has been shown that newly developed radiopharmaceutical, iodine-123 metaiodobenzylguanidine, has an impact on the diagnosis of extracranial neural crest tumors, such as neuroblastomas. The accumulation of metaiodobenzylguanidine, a functional analog of neurotransmitter norepinephrine, in neuroblastomas is related to specific uptake and storage mechanisms (3). Abnormal high uptake of metaiodobenzylguanidine has been documented in 73% to 96% of cases of extracranial neuroblastomas, and the specificity has been extremely high (4). Although this radionuclide method for imaging brain tumors has not substantially advanced, we recently reported high uptake of iodine-123 metaiodobenzylguanidine related to olfactory neuroblastoma (5) and metastatic medulloblastoma in the frontal lobe (6), as revealed by single photon emission CT (SPECT). In the present study, we encountered a similar case of medulloblastoma with extensive nodularity, wherein the diagnosis of extensive neuronal differentiation was clearly confirmed by the use of iodine-123 metaiodobenzylguanidine-SPECT. This is the first clinical application of the findings of in vitro studies of uptake of iodine-123 metaiodobenzylguanidine in neuroblastoma cell lines (7).
Case Report
The female infant, a first-born and from an uncomplicated term pregnancy, experienced normal development until 14 months of age, when she presented with unsteady gait. Her familial medical history was unremarkable. Physiological and neurologic examinations performed at admission disclosed macrocrania, a tense anterior fontanelle, bilateral papilledema, and truncal ataxia. CT showed a slightly hyperattenuated mass in the cerebellum, resulting in obstructive hydrocephalus. The tumor appeared to be a striking nodularity with attenuated enhancement after the administration of contrast medium. MR imaging revealed the remarkably nodular mass as isointense to gray matter on T1- and T2-weighted images. Contrast-enhanced T1-weighted MR imaging showed a nodular enhancement, which appeared as a grape-like lesion. The nodular enhancing mass was surrounded by edematous lesions, which appeared hyperintense on T2-weighted MR images (Fig 1). Vertebral angiography revealed a tumor blush fed by bilateral posterior inferior cerebellar arteries and superior cerebellar arteries. SPECT scans obtained 30 minutes (early image) and 6 hours (delayed image) after IV administration of iodine-123 metaiodobenzylguanidine at a dose of 111 MBq (3 mCi) showed the extremely high accumulation of iodine-123 metaiodobenzylguanidine in the enhancing tumor. The ratios of tumor uptake (the highest uptake) to non-tumor uptake, as an indicator of selective uptake in the tumor, were 5.8 and 5.9 on early and delayed images, respectively. The bilateral temporal lobes were representative of non-tumor regions (Fig 2).

Axial view MR images show an equivocal nodularity with surrounding high T2-weighted signal intensity in the tumor.
A, T1-weighted image (380/10/2 [TR/TE/NEX]).
B, Contrast-enhanced T1-weighted image (380/10/2) reveals a grape-like enhancing tumor occupying the upper part of the posterior fossa.
C, T2-weighted image (4500/100/2).
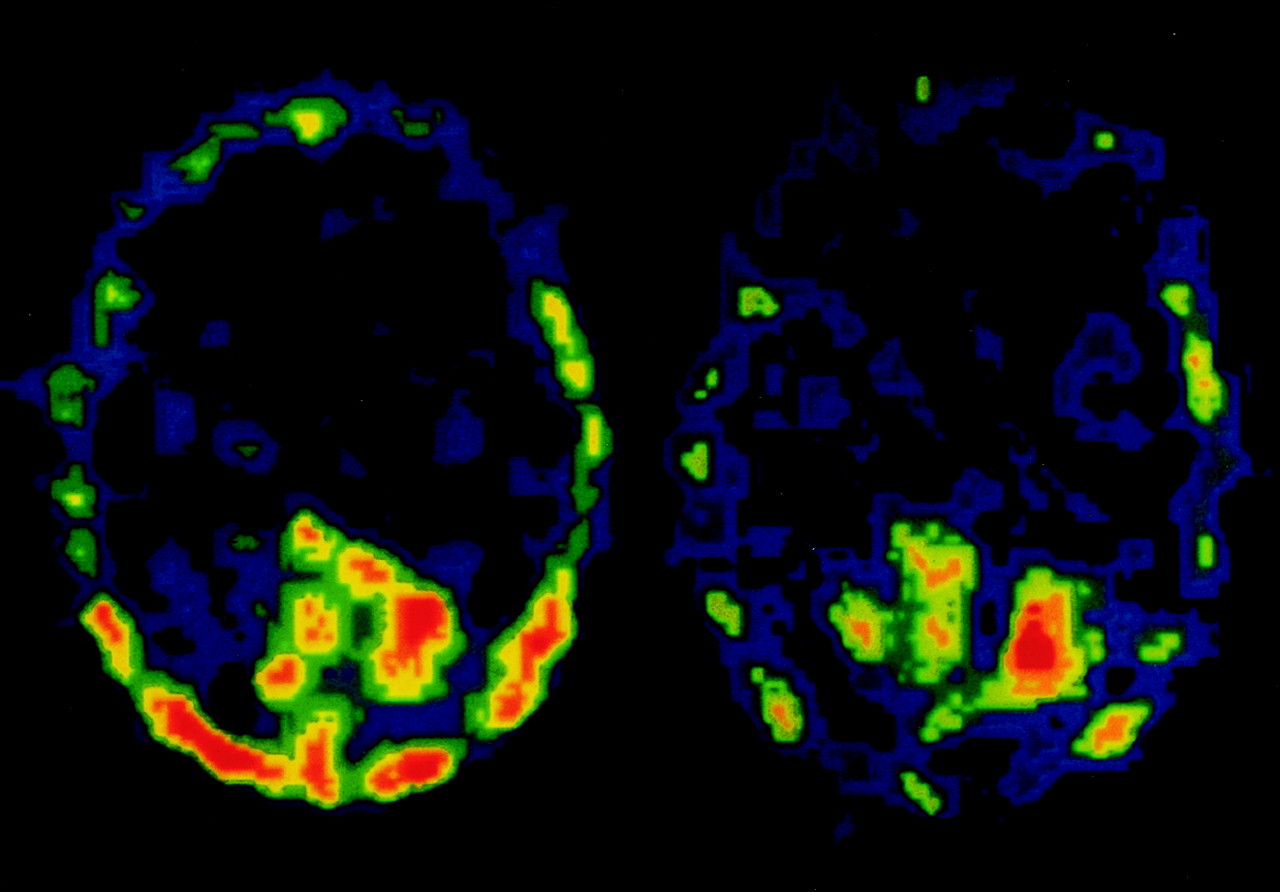
Axial view iodine-123 metaiodobenzylguanidine SPECT scans, obtained 30 minutes (left) and 6 hours (right) after an IV injection of iodine-123 metaiodobenzylguanidine at a dose of 111 MBq, shows extremely high uptake in the tumor.
The patient underwent a suboccipital craniotomy, and partial removal of the tumor was achieved via a trans-vermian route. The tumor had a well-demarcated, gray nodular appearance and showed a macroscopic pattern formed by packed aggregates of compact structures arranged in a grape-like configuration. Those nodular tumors were surrounded by edematous lesions. Microscopic examination revealed the tumor to be composed of lobulated areas (“pale islands”). Within a typical pale island area, streaming of uniform and round cells could be seen, arranged in parallel rows. Abundant reticulin fibers and mitoses were absent in typical pale island areas. Neuronal differentiation was limited to the lobulated areas (Fig 3). Immunohistochemically, the tumor cells in the pale island were intensely positive for both synaptophysin and neuron-specific enolase. The percentage of MIB-1-positive tumor cells was 4% within the pale island. Ultrastructurally, dense-cored vesicles and spherical vesicle-like structures were present in some processes, whereas we had failed to find well-developed synapses (Fig 4). These histologic findings corresponded to those of a medulloblastoma with extensive nodularity. After the surgery, the patient’s neurologic symptoms and signs gradually improved. The patient was transferred to the department of pediatrics for high-dose chemotherapy using cisplatin and etoposide with peripheral blood stem-cell transplantation.

Photomicrograph shows lobulated areas (pale islands) in the tumor (upper, hematoxylin and eosin staining; original magnification, ×50). Within a typical “pale island” area, streaming of uniform and round cells can be seen, arranged in parallel rows (lower, hematoxylin and eosin staining; original magnification, ×200).

Electron micrograph from a typical “pale island” focus reveals dense-cored vesicles (black arrows) and a spherical vesicle-like structure (white arrows).
Discussion
Medulloblastoma with extensive nodularity is a rare tumor among mass lesions of the cerebellum in infants and very young children. This variant is characterized as nodular medulloblastomas with neuronal differentiation resembling central neurocytoma according to the World Health Organization classification (8). In our patient, histologically, the nodular tumor showed multilobulated pattern with reticulin-positive septa and characteristic cellular arrangements in parallel rows within the lobules representing the histologic manifestations of neuronal differentiation. The intralobular cells were immunoreactive for neuronal markers such as synaptophysin and neuron-specific enolase and, moreover, exhibited definitive ultrastructural evidence of neuronal differentiation, including the presence of dense core vesicles and spherical vesicle-like structures, whereas abortive or complete synaptic structures were not observed. Furthermore, our tumor showed mitotic figures rarely and a relatively low proliferative potential, as shown by a low percentage of MIB-1-positive tumor cells within the pale islands. On the basis of these histologic findings, we diagnosed this tumor as medulloblastoma with extensive nodularity.
The diagnosis of medulloblastomas has been dramatically simplified with the advent of MR imaging. Medulloblastomas usually arise in the inferior medullary velum and grow anteriorly into the fourth ventricle. Although the tumor is well visualized on CT scans, MR imaging is even more sensitive in the detection of the tumor itself and in the determination of the relationship between the tumor and adjacent CNS structures. Classic medulloblastomas are shown as iso- to hypointense masses on T1-weighted MR images and as iso- to hyperintense on T2-weighted MR images (9). More than 90% of tumors have some degree of contrast enhancement in predominantly homogeneous patterns. Occasionally, peritumoral white matter “edema” was present on T2-weighted MR images (9). Intratumoral cyst or necrosis is observed in fewer than 40% of cases. Desmoplastic medulloblastomas, which are histologically similar to medulloblastoma with extensive nodularity, tend to occur in older patients and are more often lateral in position with desmoplastic reaction evoked by prominent leptomeningeal involvement. On MR images, no difference in signal intensity characteristics was observed between classic and desmoplastic medulloblastomas (9). In contrast, previous reports of medulloblastomas with extensive nodularity revealed that this variant tended to develop in intraparenchymal vermis in children younger than 3 years old in most cases and that it is frequently (nine of 12 cases) represented as a nodular enhancing grape-like appearance on CT scans or MR images (1, 2). No difference in signal intensity characteristics was observed between this variant and other medulloblastomas. For our patient, contrast-enhanced MR imaging showed a nodular enhancing mass, consistent with previous reports (1, 2). Contrast-enhanced MR imaging was useful to distinguish this tumor type from other tumors and from pathologic processes in the cerebellum that are characterized by multinodular architecture, such as dysplastic gangliocytoma (Lhermitte-Duclos disease) (10), because most such nodular lesions of the cerebellum have not been enhanced by contrast medium. In addition, the nodular tumor was surrounded by focal edema, which has not been designated in previous reports. Interestingly, we intraoperatively confirmed that nodular tumor was well circumscribed and surrounded by edematous lesions.
This is the first report of a medulloblastoma with extensive nodularity characterized by neuronal differentiation, visualized with iodine-123 metaiodobenzylguanidine SPECT. Metaiodobenzylguanidine, a physiological analog of norepinephrine, has been scintigraphically used for diagnosis of extracranial neural crest tumors, most notably neuroblastomas, pheochromocytomas, and paragangliomas, on the basis of its high sensitivity and specificity (4). Recently, we reported high uptake of iodine-123 metaiodobenzylguanidine related to olfactory neuroblastoma, as revealed by SPECT (5). In addition, we reported the use of iodine-123 metaiodobenzylguanidine SPECT to assist in the diagnosis of metastatic medulloblastoma in the frontal lobe (6) on the basis of the uptake capacity of human medulloblastoma cell lines for iodine-131 metaiodobenzylguanidine in vitro (11). On early SPECT images, the ratios of tumor uptake to non-tumor uptake for olfactory neuroblastoma and metastatic medulloblastoma were 2.3 and 2.6, respectively. In this case, we confirmed much higher uptake of iodine-123 metaiodobenzylguanidine, with the ratio of tumor uptake to non-tumor uptake being 5.8, than those of olfactory neuroblastoma and metastatic medulloblastoma. On the delayed image, the ratio of tumor uptake to non-tumor uptake remained high (5.9), which is likely suggestive of the specific uptake in the tumor. In neural crest tumor cells, such as pheochromocytomas and paragangliomas, metaiodobenzylguanidine is specifically taken up by uptake-one amine transport mechanism at the cell membrane and then transported into and stored within the neurosecretory granules in the cytoplasm. More than 90% of storage takes place in the granules, and a positive relationship between the amount of neurosecretory granules and radioiodinated metaiodobenzylguanidine uptake has been found. In neuroblastomas, however, the lack of a relationship between the amount of neurosecretory granules and radioiodinated iodine-123 metaiodobenzylguanidine uptake (3) and 60% of extragranular storage (12) have been documented, although metaiodobenzylguanidine is predominantly taken up by the uptake-one amine transport mechanism (12). Regarding the intracellular localization of metaiodobenzylguanidine in neuroblastoma cell, the minor role of neurosecretory granules has been mentioned in some studies by using electron spectroscopic imaging (13) and cryotechniques for fixation of metaiodobenzylguanidine (14). Moreover, the presence of varicosities along the neuritic processes induced by retinoic acid in human neuroblastoma cells had been associated with a concentrated aggregation of vesicles at the ultrastructural level (15). In recent studies, it was confirmed in vitro that the induction of neuronal differentiation with retinoic acid increased uptake and storage efficiency for metaiodobenzylguanidine in human neuroblastoma cell lines (7). In the present study, therefore, the extremely high uptake of iodine-123 metaiodobenzylguanidine in the tumor could indicate the evidence of neuronal differentiation in medulloblastomas. Iodine-123 metaiodobenzylguanidine SPECT may thus provide valuable information regarding differential diagnoses in cases of medulloblastomas. Although one case does not provide evidence of the general effectiveness of this technique, we hope it will encourage future study of iodine-123 metaiodobenzylguanidine SPECT in a large series of patients.
Conclusion
Preoperative diagnosis of medulloblastoma with extensive nodularity provides important information for selecting optimal therapeutic strategies for this tumor, because this variant has a better prognosis than does classical medulloblastoma. The potential value of iodine-123 metaiodobenzylguanidine SPECT would lie in the differential diagnosis of this variant tumor from other medulloblastomas and nodular lesions of the cerebellum.
Acknowledgments
The authors thank Professor Y. Nakazato, Department of Pathology, Gunma University School of Medicine, for neuropathologic diagnosis of surgical specimens.
References
- Received December 5, 2001.
- Accepted after revision May 1, 2002.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.