
Abstract
Summary: We report a case of cerebral fat embolism (CFE) that was imaged with T2- and T2*-weighted, fluid-attenuated inversion recovery, and contrast-enhanced T1-weighted images. Multiple white matter lesions demonstrated contrast enhancement, with little evidence of hemorrhage. The patient regained complete neurologic function. CFE can cause capillary inflammation and breakdown of the blood-brain barrier, without associated hemorrhage or permanent neurologic deficit. In this case, both contrast-enhanced T1-weighted and gradient-echo T2*-weighted images were important in diagnosing CFE and in determining the severity of the patient’s condition.
Fat embolism syndrome (FES) is generally associated with displaced long-bone fractures of the lower extremities, which occur in 0.5–3.5% of cases (1, 2). FES may also occur with nondisplaced fractures and fractures of smaller bones. Fat emboli may reach the brain through a right-to-left cardiac shunt or through an intact pulmonary circulation in patients without a shunt (3). The major clinical characteristics of FES include respiratory insufficiency, neurologic symptoms, and a petechial skin rash. Neurologic symptoms may vary considerably, ranging from a subclinical presentation to confusion to coma and seizures; in rare cases, death may result. The number of white matter lesions on MR images is correlated with the patient’s score on the Glasgow coma scale (4). In most cases, neurologic function is gradually recovered over days to months.
The pathologic hallmarks of cerebral fat embolism (CFE) include petechia or purpura distributed throughout the white matter of the cerebrum and cerebellum, with relative sparing of the gray matter (5, 6). Fat globules occlude the microvasculature, with necrosis and hemorrhage in the surrounding parenchyma (5). Infarcts may range from a few millimeters to 4 cm in diameter. The chronic sequela of CFE is extensive demyelination of the white matter; however, these descriptions may not accurately reflect the full spectrum of CFE, because they are primarily based on autopsy results, which are biased toward the most severe cases. Indeed, findings from recent animal model studies suggest that fat embolism can result in the breakdown of the capillary endothelium and the blood-brain barrier, causing focal vasogenic edema without infarction or hemorrhage (7, 8).
This case provides evidence that CFE in humans is associated with breakdown of the blood-brain-barrier as a predominant feature on contrast-enhanced T1-weighted images. The results of T2*-weighted gradient-echo imaging confirmed that focal parenchymal hemorrhage was not a predominant feature in the case presented here.
Case Report
A 28-year-old man who was the unrestrained driver of an automobile that struck a light pole at 40 mph presented to the emergency department with bilateral femoral fractures. Although he reported a loss of consciousness at the scene, he arrived at the emergency department with a Glasgow coma score of 15 and stable vital signs. Results of preoperative CT scanning of the head were negative. The patient was taken to the operating room for open reduction and internal fixation of the bilateral femoral fractures, after which the patient was transferred to the surgical intensive care unit because of his persistent somnolence. At that time, his Glasgow coma score was 9. Findings on CT and the MR images of the head obtained later that day were unremarkable; however, the MR images were slightly compromised by head motion effects.
The suspected diagnosis at that time was CFE, and the workup included transesophageal echocardiography, which demonstrated no patent foramen ovale. No pulmonary symptoms were present, and all laboratory data (including the results of arterial blood gas analyses) were normal. Findings from a nuclear medicine lung perfusion study were normal. Repeat cerebral MR imaging was performed 9 days after the initial MR imaging examination. The T1-weighted imaging findings were unremarkable; however T2-weighted and fluid-attenuated inversion recovery images (Fig 1) demonstrated multiple new hyperintense foci in the periventricular, deep, and subcortical cerebral white matter. A lesion was also present in the splenium of the corpus callosum, mimicking axonal shear injury. On contrast-enhanced T1-weighted images, many of these lesions demonstrated distinct enhancement (Fig 2). A single punctate area of decreased signal intensity was identified on gradient-echo T2*-weighted images in frontal subcortical white matter (Fig 3); this was thought to likely represent blood products associated with CFE, focal axonal shear injury, or a prior unrelated insult. Otherwise, the multitude of white matter lesions showed no evidence of associated hemorrhage. The MR imaging findings were consistent with CFE, which causes breakdown of the blood-brain barrier with vasogenic edema or cytotoxic edema or both. The patient completely recovered his neurologic function; this occurrence indicated that infarction was not a predominant feature of his condition. The patient was discharged from the hospital 15 days after his admission.
Discussion
Subclinical fat embolism is present after nearly 100% of long-bone fractures, although the FES is present in only 0.5–3.5% of cases (1, 2). Typical clinical manifestations occur within several hours of trauma and may appear as a triad of pulmonary, central nervous system, and cutaneous manifestations. CFE can occur at the scene of a major trauma (9), mimicking severe head injury. The condition occurs predominantly in patients with long-bone fractures or in those who have undergone orthopedic manipulation (2). FES can occur with a wide range of severity, and its classification entails subclinical, nonfulminant, and fulminant forms (10). Reported mortality rates range from 13% to 87%, although partial or complete recovery is not uncommon. This case represents nonfulminant FES in which only neurologic symptoms were present and complete recovery occurred.
CFE need not coexist with respiratory failure (3, 11, 12). Although the emboli may reach the systemic circulation via a patent foramen ovale or other arteriovenous communication, fat emboli may traverse the pulmonary capillaries to enter the systemic vasculature, most often embolizing to the brain or kidneys. Fat emboli are deformable and can penetrate capillaries. The narrow capillary lumen causes transient stasis of fat emboli, which results in the breakup of the fat globules into smaller sizes. These then recycle through the pulmonary circulation. As a result, systemic and pulmonary vascular occlusion is temporary (7, 10). In the case presented here, the patient had no pulmonary symptoms, and no patent foramen ovale was identified; this observation suggested direct passage through the pulmonary circulation. Absence of pulmonary symptoms may be related to a sufficient pulmonary reserve in young, previously healthy individuals (3). In addition, the absence of pulmonary findings further supports the conclusion of Bardana et al that fat emboli, and not global hypoxemia or cerebral edema, cause the neurologic dysfunction in FES (3).
CT findings in CFE have been previously described (9, 13–16). Most often, the brain CT results are normal, as in this patient. CT may show diffuse edema with scattered low-attenuating areas and hemorrhage in some cases. CT findings may be normal despite encephalopathy or focal neurologic deficits (16). The MR findings of CFE have also been previously described (3, 4, 13, 17, 18, 11, 19, 20, 12). Findings include small, scattered, hyperintense lesions on long-TR images. These appear predominantly in periventricular, subcortical, and deep white matter. White matter lesions may or may not be associated with focal hemorrhage (20). A recent publication described the scattered hyperintense findings on diffusion-weighted images; these presumably representing CFE-induced ischemic foci (21). Laboratory studies in animals have recently revealed distinct contrast enhancement in CFE lesions on T1-weighted images (7, 8); our case demonstrates this phenomenon in human CFE. The initial CT and MR images in our case showed no evidence of CFE, although the MR images were somewhat limited because of motion artifact. The typically small, scattered, hyperintense lesions on long-TR images were identified on follow-up MR images obtained 9 days later, which showed a predominantly white-matter distribution. Many of the lesions enhanced with the administration of contrast material; these results correlated with animal data suggesting breakdown of the blood-brain barrier. In addition, the gradient-echo images showed little evidence of hemorrhage, which, along with the clinical history, differentiates this entity from diffuse axonal injury. Other imaging differential diagnoses included common white-matter etiologies of this age group that may have been preexisting; examples are multiple sclerosis and acute disseminated encephalomyelitis. These are less likely because of the temporal relationship of the symptoms with the injury. The most reasonable imaging diagnosis in this case was CFE.
The pathogenesis of the cerebral lesions in CFE remains largely unexplained. Kamenar et al (5) described the gross pathologic findings in the brain, which include both hemorrhagic and anemic lesions with classic findings of perivascular hemorrhages. The microscopic demonstration of globules of neutral fat in microvessels with surrounding extravasated blood confirms the diagnosis. Infarcts may be seen; these can range from a few millimeters to 4 cm in diameter. Fat globules are actually more common in the blood vessels of the gray matter than in those of the white matter. Some have suggested that the white matter lesions are indirectly produced by cortical emboli, causing venous sludging and white matter edema (5). Some have also suggested that the focal abnormalities on MR images represent ischemic insults due to direct occlusion of microvasculature by fat emboli (20). This suggestion implies that the lesions represent cytotoxic edema resulting from direct hypoxic-ischemic insult. Anegawa and associates (20) and Erdem and associates (22) have suggested that the MR findings represent small infarcts seen in pathologic studies. Given the present case and other reported cases of reversible CFE lesions in the literature, we might reasonably suggest that the likelihood of infarction and hemorrhage depends on the size of the fat globules, which depends on the presence or absence of a cardiac shunt and the overall embolism load. Our case showed little evidence of hemorrhage on T2*-weighted images and no permanent sequelae to indicate such destructive ischemic effects.
Peltier (23) identified the toxic effects of neutral fat in the lung, introducing the concept of local alteration of chemical physiology. Studies of pulmonary fat embolism have revealed similarities to adult respiratory distress syndrome. The results suggest that fat globules activate chemical mediators that alter capillary permeability. The free fatty acids potentiate the release of prostaglandins, leukotrienes, and thromboxanes, which enhance the permeability of capillaries and exacerbate tissue edema. In recent animal studies of CFE, MR findings were correlated with electron microscopic findings (7, 8). The results showed scattered, predominantly white matter lesions that demonstrated marked enhancement at contrast-enhanced T1-weighted imaging, high-signal-intensity lesions at long-TR imaging, and disruption of the endothelial walls with interstitial edema at electron microscopy. These findings suggest early breakdown of the blood-brain barrier with vasogenic edema as one cause for the MR findings. The enhancement pattern substantially differed from that of the ischemic control group. Cytotoxic edema was also an early finding in both the fat emboli group and ischemic control group, with electron microscopy showing neuronal and glial cell swelling. The authors also suggest that the conspicuity of the enhancing lesions on the contrast-enhanced T1-weighted images was greater than that of the lesions on diffusion-weighted or long-TR images. This observation signifies early breakdown of the blood-brain barrier associated with vasogenic and cytotoxic edema.
The findings of enhancement on contrast-enhanced T1-weighted imaging, disrupted endothelial walls, and extravasated fat globules in animal models (7), as well as the diffuse lesion enhancement in our case, support the hypothesis that the white matter lesions are, in part, due to direct chemical effects of fatty acids. However, actual ischemic white matter lesions can occur with CFE, despite the fact that most of the emboli are present in the gray matter. A potential hypothesis to explain this observation implicates the protective anastomotic vascular potential of gray matter. Regardless of the mechanism, infarction can be observed with MR imaging. Restricted diffusion in some lesions, as suggested on diffusion-weighted images (21), may be correlated with the recent animal findings that demonstrate neuronal and glial cell swelling at electron microscopy (7, 8).
Conclusion
MR imaging is the most sensitive technique to evaluate less severe cases of CFE and contrast-enhanced T1-weighted imaging is useful to demonstrate breakdown of the blood-brain barrier that is characteristic of this condition. Long-TR sequences can show foci of vasogenic edema, and results on diffusion-weighted images can confirm the presence of embolic cytotoxic edema. In addition, gradient-echo imaging can be helpful in determining the presence of focal hemorrhage, which may be useful in making the differential diagnosis and in defining the severity of the cerebral FES. More research is needed to determine if the full spectrum of MR imaging characteristics described here and if those reported by others have prognostic importance.

Fluid-attenuated inversion recovery MR images of the brain acquired 9 days after a repair of long-bone fractures show multiple focal lesions in the periventricular, deep, and subcortical white matter. These are characteristic of CFE.
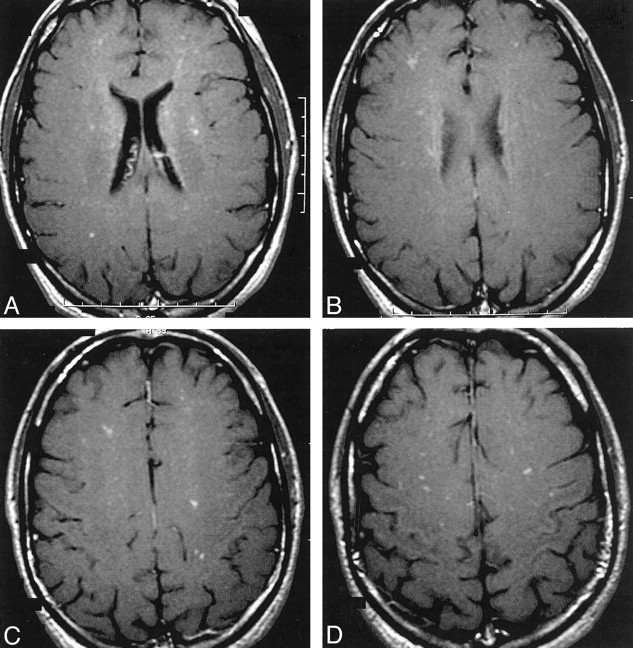
Contrast-enhanced MR images of the brain show focal enhancement in many of the white matter lesions.

T2*-weighted gradient-echo MR images of the brain show a single focus of susceptibility (arrow in C) in the left frontal white matter. This finding suggests a preexisting focus of hemorrhage from axonal shear injury or CFE or both. However, hemorrhage was not a predominant feature of the multiple white-matter lesions arising from CFE in this case.
References
- Received June 10, 2002.
- Accepted after revision July 12, 2002.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Woman with acute onset involuntary limb movements
- Use of the Reamer/Irrigator/Aspirator Decreases Carotid and Cranial Embolic Events in a Canine Model
- Role of susceptibility-weighted imaging in demonstration of cerebral fat embolism
- Dynamic MR Imaging Patterns of Cerebral Fat Embolism: A Systematic Review with Illustrative Cases
- Intracranial transthecal subarachnoid fat emboli and subarachnoid haemorrhage arising from a sacral fracture and dural tear