
Article Figures & Data
Figures
- Fig 1.
Patient 21, a 62-year-old man who was previously treated for squamous cell carcinoma of the floor of the mouth with primary and level I lymph node resection at an outside institution.
A, Coil-corrected axial view fast spin-echo T2-weighted image with fat saturation (4000/90/4) shows pathologically enlarged left neck nodes in level IIA and superficial to the sternocleidomastoid muscle (white arrows). The level IIA node shows internal areas of irregular low signal intensity (arrowheads), an appearance we would describe as nodal heterogeneity but not nodal necrosis. Note that it would be impossible to exclude these small, irregular areas from region of interest analysis. Also note the soft tissue deformity and absence of the ipsilateral submandibular gland due to previous resection.
B, Coil-corrected axial view contrast-enhanced T1-weighted image with fat saturation (600/20/2), obtained at the same level as that shown in A, shows slightly irregular enhancement of both nodes, with the irregularity clearly more pronounced in the level IIA node. Both nodes were pathologically confirmed to be tumor-involved.
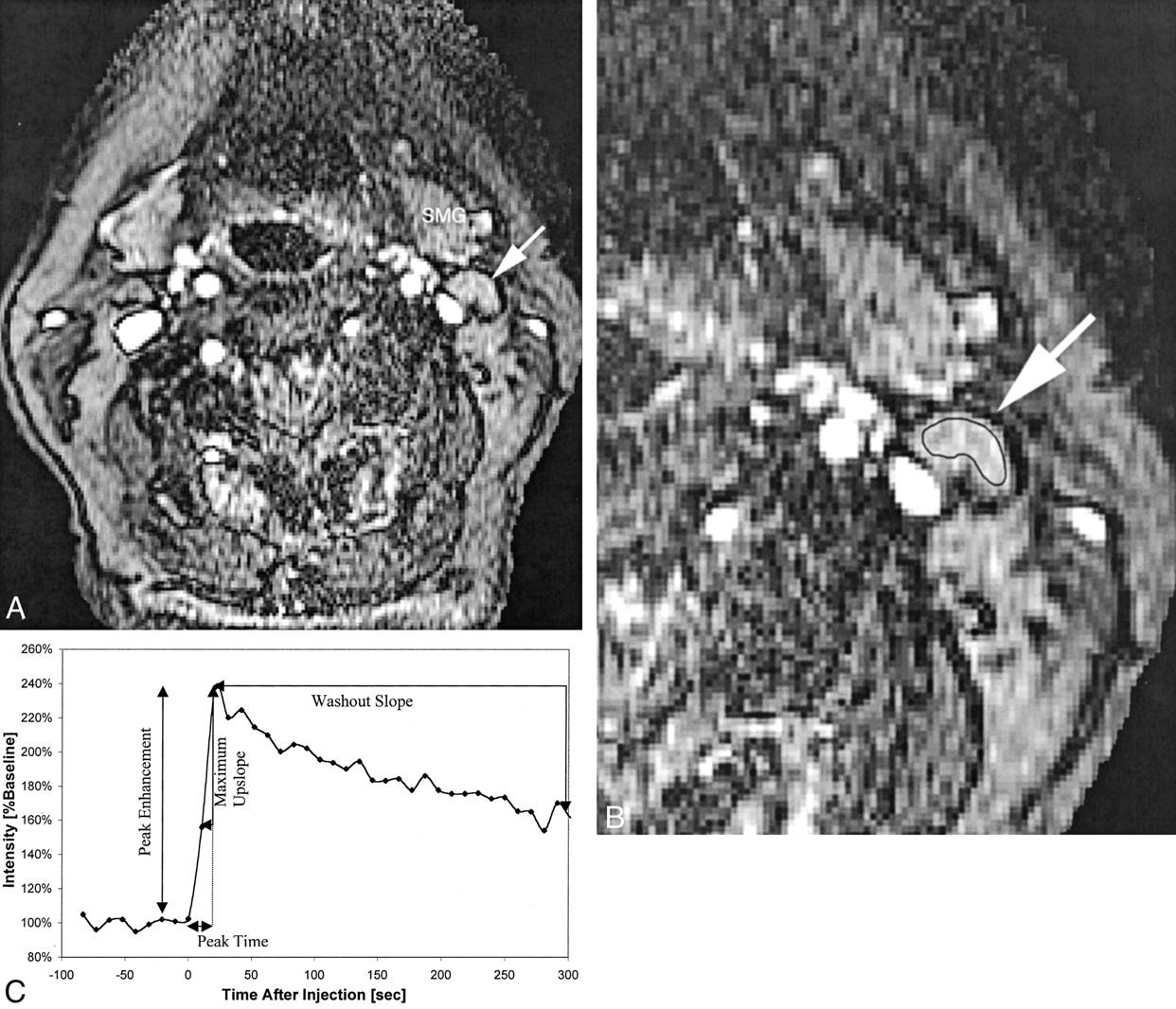
- Fig 2.
Patient 16, an 83-year-old woman with newly diagnosed squamous cell carcinoma of the lateral tongue.
A, Axial view fast spoiled gradient recalled image (10.4/2.3; flip angle, 30 degrees), obtained during bolus administration of contrast agent, shows a normal appearing left level IIA lymph node (arrow). SMG, submandibular gland.
B, Same image as that shown in A, magnified to emphasize the area of interest and with a region of interest indicator placed over the level IIA node. Pathologic analysis showed that this lymph node was not a tumor-involved node.
C, Plot of signal intensity versus time generated from the region of interest placed around the cervical lymph node shown in B. Derivation of peak time, peak enhancement, maximum up-slope, and washout slope are illustrated.
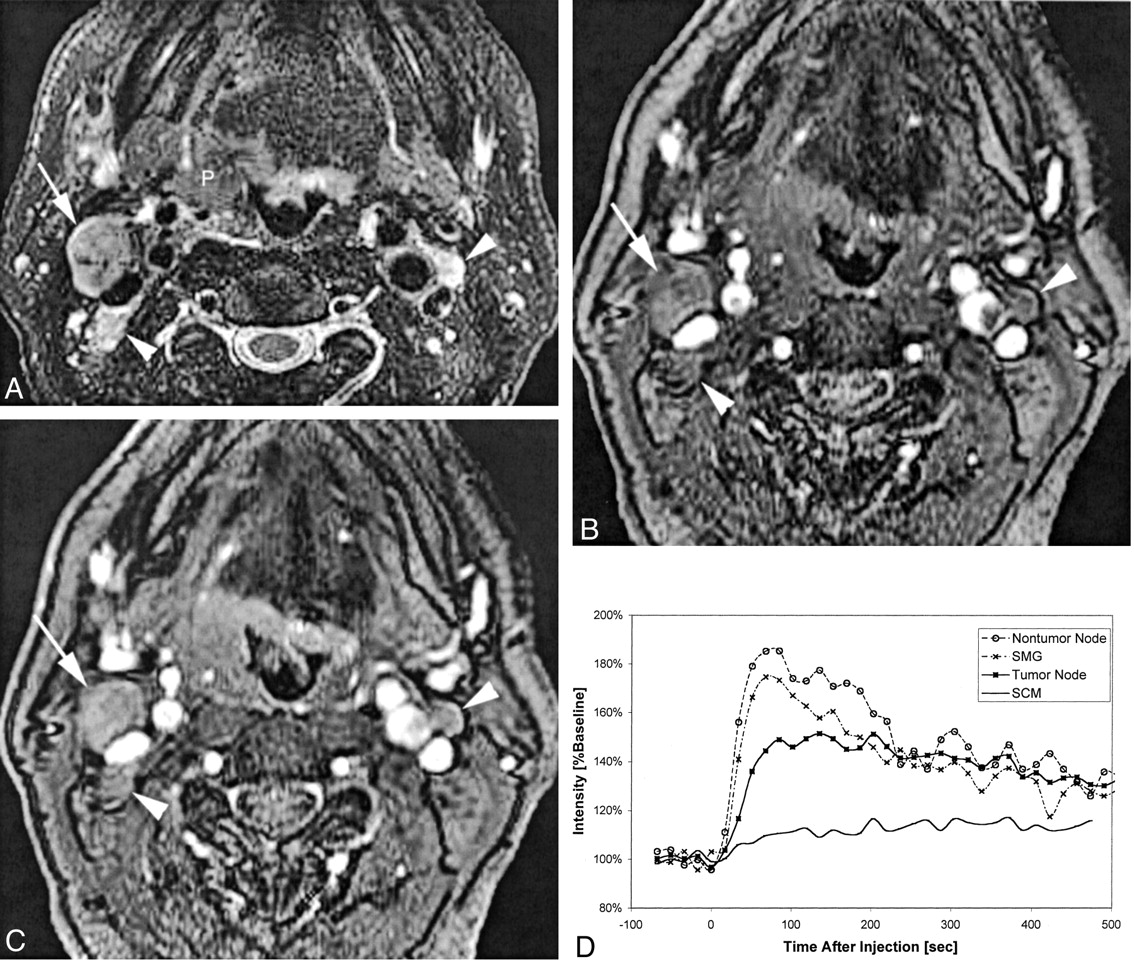
- Fig 3.
Patient 6, a 57-year-old man with right oropharyngeal cancer and multiple palpable nodes who underwent pharyngectomy, right modified radical neck dissection, and left supraomohyoid neck dissection.
A, Coil-corrected fast spin-echo T2-weighted image with fat saturation (4000/90/4) shows the primary tumor (P), a dominant tumor-involved right level IIA node (white arrow), and two smaller tumor-involved level IIA lymph nodes (white arrowheads) on the right and left sides of the neck.
B, Baseline image (10.4/2.3; flip angle, 30 degrees) from the dynamic sequence shows the same tumor-involved nodes 117 seconds after contrast medium injection.
C, Enhanced dynamic image (10.4/2.3; flip angle, 30 degrees) shows the same tumor-involved nodes.
D, Plot of signal intensity versus time after injection of contrast agent, generated from regions of interest placed on the right level IIA tumor-involved node, a left level III non-tumor-involved node (not included on these images), the submandibular gland (SMG), and the sternocleidomastoid muscle (SCM). The different curve morphologies generated from these different tissues can be appreciated as shown by this comparison plot.
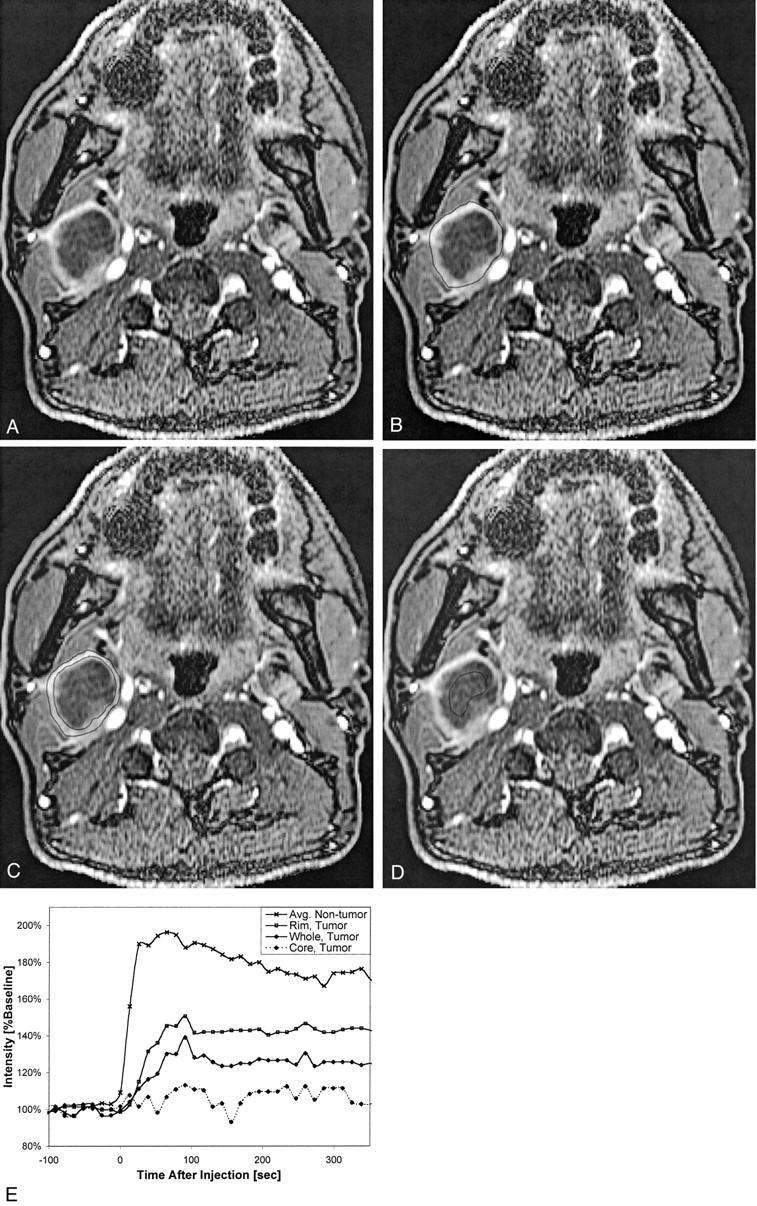
- Fig 4.
Patient 7, a 52-year-old man who had previously undergone partial glossectomy for squamous cell carcinoma of the tongue, received no additional therapy, and then presented with a palpable right neck mass. Fine needle aspiration confirmed recurrent squamous cell carcinoma in the neck, and MR imaging revealed right cervical necrotic lymphadenopathy. The patient then underwent re-excision of the primary site and a right radical neck dissection.
A, Coil-corrected axial view enhanced dynamic image (10.4/2.3; flip angle, 30 degrees), acquired 195 s into the acquisition, shows a large, centrally necrotic, right level IIA lymph node.
B, Same image as that shown in A, with the region of interest encompassing the whole node shown.
C, Same image as that shown in A, with the region of interest encompassing only the rim shown.
D, Same image as that shown in A, with the region of interest encompassing only the necrotic core shown.
E, Plot of signal intensity versus time from this node, with curves generated from regions of interest placed on the whole node, the rim only, and the necrotic core only. Note that the “rim” curve is very similar to the “whole” curve but appears reduced in magnitude by a scaling factor related to the necrotic core. All these curves appear very different from the average non-tumor curve that is shown for comparison, but a statistically significant comparison was not possible because of the small number of grossly necrotic nodes.


Tables
Patient No. Age (y)/Sex Diagnosis Preoperative Staging* Nodal Status on Conventional Images (CT Scan or MR Image) Postoperative Staging 1 44/F SCC tongue T3N1 CT: negative (N1 based on palpation) T3N2c 2 59/M SCC floor of mouth T2N0 MR: negative T2N0 3 56/M SCC buccal mucosa T2N0 MR: negative T1N0 4 64/F SCC oropharynx T3N0 CT:negative T2N0 5 53/M SCC oropharynx T3N2a MR: multiple abnormal nodes T3N2a 6 57/M SCC oropharynx T4N2c MR: multiple abnormal nodes T4N2c 7 52/M SCC tongue TxN2b† MR: multiple abnormal nodes TxN2b 8 72/M SCC retromolar trigone T2N2b MR: multiple abnormal nodes T1N2b 9 72/F SCC nasal cavity TxN1† CT: single necrotic node TxN1 10 63/M SCC tongue T3N0 MR: negative T2N0 11 71/M SCC tongue T3N0 MR: negative (but N1 based on PET) T3N1‡ 12 79/F SCC alveolar ridge T3N2b MR: multiple abnormal nodes T4N2b 13 74/M SCC retromolar trigone T2N0 MR: negative T2N1‡ 14 65/F SCC alveolar ridge T4N0 MR: negative T4N0 15 47/M SCC tongue TxN2b† CT: multiple abnormal nodes TxN2b 16 83/F SCC tongue T1N0 MR: negative T1N0 17 52/M SCC tongue T1N0 MR: negative T1N0 18 44/F SCC tongue T1N0 MR: negative T1N0 19 66/M SCC alveolar ridge T4N0 MR: negative T4N0 20 85/F SCC buccal mucosa T4N0 CT: negative T4N1‡ 21 62/M SCC floor of mouth TxN2b† CT: multiple abnormal nodes TxN2b Note.—F indicates female; M, male; SCC, squamous cell carcinoma; PET, positron emission tomography.
* All patients were staged as M0. Preoperative staging was based on clinical palpation and conventional anatomic imaging with CT and/or MR imaging, not high resolution MR imaging.
† Primary site previously excised (hence, the “Tx” designation), but no radiation or other therapy to the neck previously received. Patient evaluated and treated for neck disease.
‡ Three patients preoperatively staged as N0 were upstaged to N1 based on pathologic findings.
- TABLE 2:
Dynamic contrast-enhanced MR imaging features of tumor involved versus non-tumor-involved nodes
No. Peak Time (s) Peak Enhancement (%baseline) Maximum Slope (%baseline/min) Washout Slope (%baseline/min) Tumor-involved 25 111 (68) 176 (30) 193 (123) −7.6 (5.3) Non-tumor-involved 43 46 (29) 198 (46) 324 (224) −12.2 (8.1) P value <.001 <.05 <.01 <.05 Note.—Number in parentheses indicates SD. Also note that the washout slope for non-tumor-involved nodes is based on N = 40 rather than 43 because late data points were not acquired for three nodes.
- TABLE 3:
Dynamic contrast-enhanced MR imaging characterization of submandibular gland and sternocleidomastoid muscle
Tissue Peak Time (s) Peak Enhancement (%baseline) Maximum Slope (%baseline/min) Washout Slope (%baseline/min) SMG 50 (41) 206 (67) 333 (186) −11.4 (6.6) SCM 264 (102) 125 (10) 49 (36) −3.0 (10.9) Note.—Number in parentheses indicates SD. SMG, submandibular gland; SCM, sternocleidomastoid muscle.
Tissue Peak Time (s) Peak Enhancement (%baseline) Maximum Slope (%baseline/min) Washout Slope (%baseline/min) Whole necrotic node 114 (22) 131 (14) 57 (12) −0.1 (0.001) Peripheral rim only 136 (48) 180 (49) 171 (132) −0.2 (0.05) Normal node 46 (29) 198 (46) 324 (224) −12.2 (8.1) Note.—P values cannot be calculated because of the small number of necrotic nodes.
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Dynamic Contrast-Enhanced MR Imaging in Head and Neck Cancer: Techniques and Clinical Applications
- Optimization of Ultrasmall Superparamagnetic Iron Oxide (P904)-enhanced Magnetic Resonance Imaging of Lymph Nodes: Initial Experience in a Mouse Model
- Multiparametric MR Imaging of Sinonasal Diseases: Time-Signal Intensity Curve- and Apparent Diffusion Coefficient-Based Differentiation between Benign and Malignant Lesions
- Current Concepts in Lymph Node Imaging