
Abstract
Summary: We report the case of a 57-year-old man with a known history of antineutrophil cytoplasmic antibody-positive Wegener granulomatosis with initial involvement of the upper and lower respiratory tract. MR imaging of the brain was performed because of new onset CNS symptoms (nausea, altered mental status). The images revealed a mass in the fourth ventricle. The mass diminished in size after systemic steroid treatment, as shown by follow-up MR imaging. The patient died in acute respiratory distress secondary to pneumonia. Histopathologic findings confirmed a Wegener granuloma of the fourth ventricle.
Wegener granulomatosis is a rare autoimmune vasculitis of unknown cause characterized by necrotizing granuloma of the respiratory tract, focal necrotizing glomerulonephritis, and systemic vasculitis (1–4). Wegener granulomatosis belongs to the small vessel vasculitides with association to antineutrophil cytoplasmic antibodies, which are usually specific for proteinase 3(5). Although the paranasal sinuses, lungs, skin, and kidneys are most commonly affected, many other organs can be involved. Neurologic involvement in Wegener granulomatosis was described in 25.7% to 54% of patients before the era of effective therapeutic agents, including prednisone and cyclophosphamide (6, 7) and in 22% to 33.6% of patients after the advent of more effective immunosuppressive regimens (2, 4).
Case Report
A 57-year-old man developed dyspnea, bloody rhinitis, and hoarseness 2 years before admission. Radiologic examination of the chest revealed suspicious right pulmonary infiltrates. Pathohistologic workup after right superior lobe resection confirmed the diagnosis of Wegener granulomatosis. An antineutrophil cytoplasmic antibody with specificity for proteinase 3 was detected in the patient’s sera, and immunosuppressive therapy with systemic steroids and oral cyclophosphamide was initiated. Secondary to ineffectiveness or side effects (lymphocytopenia leading to recurrent infections) of the immunosuppressive regimen, several changes of the therapy were necessary during the ensuing months. In addition to steroids that were orally and IV administered at different doses, the immunosuppressive regimens consisted of desoxyspergualin (subcutaneously administered), leflunomid (orally administered), and cyclophosphamide (IV and orally administered) for different intervals. Despite ongoing immunosuppressive therapy, the patient complained of nausea, vomiting, and headache and developed progressive neurologic deficits with skew deviation, slight upbeat nystagmus, and diplopia. MR imaging (Fig 1) showed a well-delineated mass in the inferior fourth ventricle, compressing and infiltrating the surrounding structures with extrusion through the left foramen of Luschka. Our differential diagnoses of the fourth ventricle mass included ependymoma and Wegener granuloma. Biopsy of the tumor was canceled because of the patient’s respiratory insufficiency and poor clinical condition. High doses of prednisone and cyclophospamide had to be administered in addition to antibiotics. Under this treatment, the neurologic symptoms improved. Follow-up MR imaging performed after 4 and 6 weeks showed tumor regression, whereas the nonocclusive hydrocephalus remained the same (Figs 2 and 3). Despite tumor regression, the pulmonary complications progressed. The patient died 4 months later.

Initial contrast-enhanced T1-weighted MR images obtained in three planes and coronal view diffusion-weighted image (lower right) show inhomogeneous contrast enhancement of a mass at the floor of the fourth ventricle. Compression and infiltration of the left dorsolateral medulla oblongata and the vermis can be seen, with extrusion through the left foramen of Luschka. Concomitant hydrocephalus is revealed, and high signal intensity on the diffusion-weighted image implies dense cellularity of the tumor. Note the thickening of the mucosa with contrast enhancement at the paranasal sinuses, whereas CT scans revealed intact bony structures.

Follow-up MR images obtained 4 weeks after initial imaging, during immunosuppressive therapy. Approximately 50% tumor regression is revealed. Remaining high signal intensity in the lesion can be seen on the diffusion-weighted image.

Follow-up MR images obtained 6 weeks after initial imaging show slight additional regression of the tumor but evident reduction of the signal intensity on the diffusion-weighted image and remaining nonocclusive hydrocephalus.
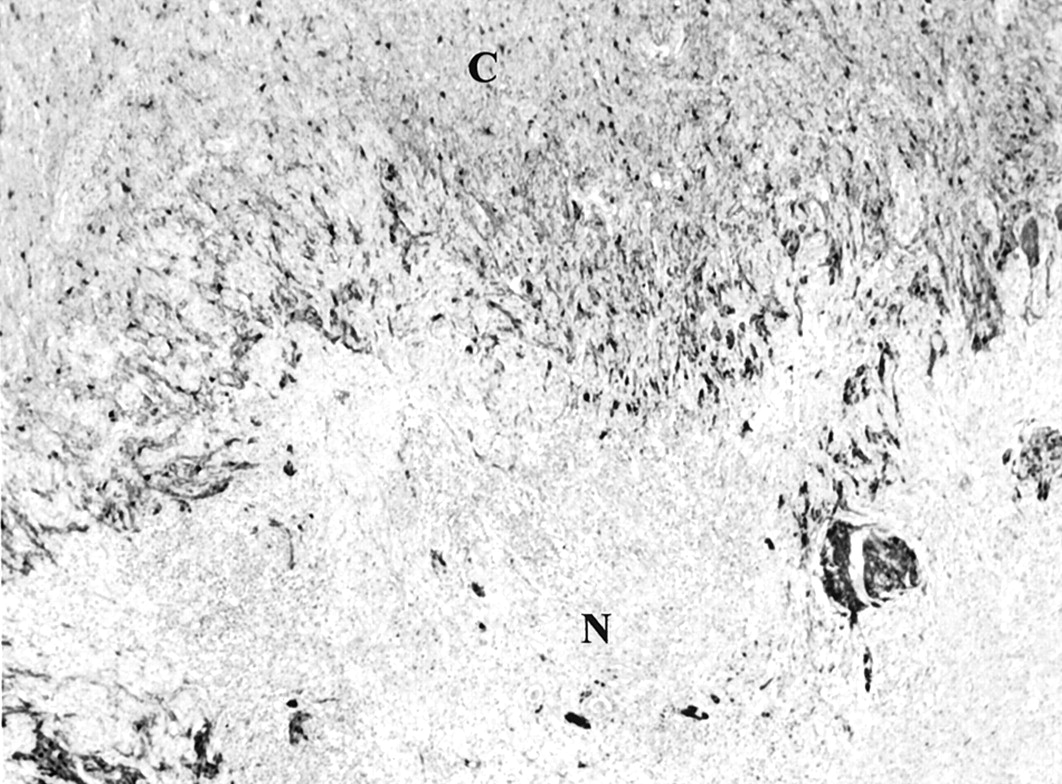
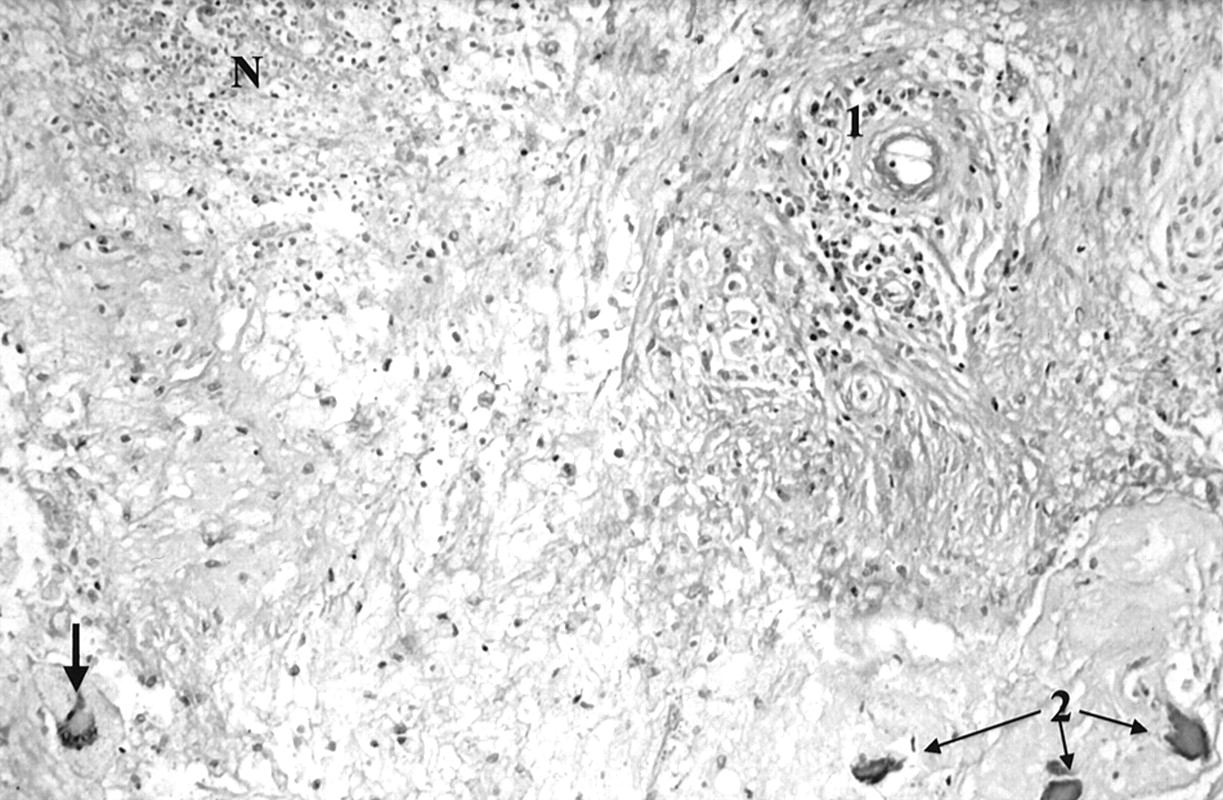
Histopathologic examination (Figs 4–6) showed that the immediate cause of death was pneumonia and cachexia. Slight obstructive hydrocephalus was seen, and a necrotic mass was found in the inferior fourth ventricle, containing infiltrates of lymphocytes, eosinophilic granulocytes, plasma cells, accumulations of macrophages, and typical multinucleated giant cells. Calcifications with surrounding scarred connective tissue were observed, as was necrotizing vasculitis leading to vessel occlusion. The mass originated in the vermis, and diffuse infiltration of the adjacent cerebellum and the medulla oblongata was observed. No signs of acute inflammatory processes, CNS neoplasia, or metastasis were seen. Additionally, pulmonary fibrosis secondary to Wegener granulomatosis was confirmed histologically.


Histologic specimen (glial fibrillary acidic protein stained) with necrotizing mass (N) shows diffuse infiltration of the cerebellum (C).

Discussion
The estimated incidence of Wegener granulomatosis is 1:100,000 per year (8). In former times, the outcome almost invariably was fatal. The prognosis dramatically improved once sufficient immunosuppressive regimens became available (5). Mahr et al (9) currently report a mortality rate of 37% during a mean follow-up period of 1.9 years.
Neurologic involvement in Wegener granulomatosis has been reported in ≤54% of the cases (2, 6, 7). After the advent of therapeutic agents, including prednisone and cyclophosphamide, neurologic involvement decreased to 22% (4). According to Drachmann (6), there are three different types of CNS involvement: direct granulomatous infiltration from contiguous lesions in the nose and paranasal sinuses, remote lesions from the nose and paranasal sinuses, and vasculitis of the nervous system itself. Peripheral nervous system involvement is present in approximately 10% to 16% of the cases (2, 4), and cerebral and meningeal involvement is rare (reported in 2% to 8% of cases of Wegener granulomatosis) (2, 4, 6, 10). On CT scans and MR images, white matter lesions with or without contrast enhancement, infarcts due to primary manifestations of the disease (eg, vasculitis or arterial occlusion caused by granulomatous vasculitis), and thickening of the dura with contrast enhancement may be found (2, 4, 11–18). Diffuse, symmetric thickening of the entire dura was seen, as was focal, nodular, and plaquelike thickening with mass effect (4, 12–15). Two patients were described as having thickening and contrast enhancement of the dura overlying the thoracic spinal cord (4, 13). The pituitary gland and infundibulum may be involved by means of distant granulomas or direct spread (6, 13, 19, 20). Only a few reports have been published showing subarachnoid hemorrhage (6, 21), intracerebral hemorrhage (6), and arterial occlusion (6, 22). Histologically or radiologically confirmed vasculitis of the CNS in Wegener granulomatosis is very rare (4, 23). Typically, small vessels (50–300 μm) are affected in cases of Wegener granulomatosis (4). In our case, necrotizing vasculitis with vessel occlusions could be detected only within the tumorlike mass whereas generalized or distant focal vasculitis was absent.
The external ophthalmoplegia associated with Wegener granulomatosis is probably related to granulomatous infiltration of the orbit or the cavernous sinus (4, 24). Drachmann (6) found cranial nerve involvement due to remote granulomatous lesions in 2% of his patients. Anderson et al (7) found 65 cases presenting with affection of the cranial nerves. It was assumed that cranial neuropathy occurred secondary to either direct or remote extension of the granulomatous lesion. Cranial nerve involvement has been described in 6.5% (21 of 324 cases) (4) to 9.4% (eight of 85 cases) (2) of the cases.
Remote granulomatous lesions in association with brain parenchyma are the least common form of CNS involvement in cases of Wegener granulomatosis. With respect to the classification of Drachmann (4), our patient presented with a remote granuloma of the fourth ventricle and additional affection of the upper respiratory tract (nose and paranasal sinuses). Because there is no need to declare the nose or paranasal sinuses as a source for a remote lesion, even if the involvement of another classically related organ is known and the contiguity is excluded, the above-mentioned classification is questionable today. In addition to exclusion of a contiguous granuloma by CT findings that showed intact bony structures of the paranasal sinuses, the surrounding leptomeningeal structures were not affected.
Acknowledgments
The authors thank Paul S. Jackson, MD, PhD, and Bill Perry for reviewing the manuscript. We thank Albrecht Hochmuth, MD, Ulrich Pechstein, MD, Hans-Hartmut Peter, MD, Joachim Klisch, MD, and Martin Schumacher, MD, for thoughtful contributions to the manuscript.
References
- Received July 24, 2002.
- Accepted after revision August 19, 2002.
- Accepted after revision August 19, 2002.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.