
Abstract
Summary: A 9-year-old girl with osteogenesis imperfecta (OI) type 4 was admitted to the hospital because of choreatic movement. Cerebral angiography demonstrated bilateral symmetrical stenosis of the proximal cavernous segment of internal carotid artery, prethrombotic occlusion of the M1 segment of left middle cerebral artery, and moyamoya-like collateral vascular structure arising from the right lenticulostriate arteries. After a literature review, these findings were interpreted as vasculopathic changes secondary to vascular fragility caused by the collagen abnormality in OI.
Osteogenesis imperfecta (OI) is a heterogeneous group of heritable connective tissue disorders characterized by fragile and brittle bones, blue sclera, dental malformations, deafness, and hyperextensible ligaments (1–3). OI is associated with type 1 collagen abnormalities caused by a spectrum of mutations in the α-1 chains of procollagen and with decreased synthesis of normal type 1 collagen (4). Type 1 collagen is normally associated with large parenchymal and leptomeningeal vessels, but it is absent around capillaries in the CNS (3). Aortic dissections, carotid-cavernous fistulas, cervical artery dissections, and ulnar artery aneurysms associated with OI are reported in the literature (5–7). Little is known about the effects of the abnormal collagen on the CNS. We report a case of 9-year-old girl who had OI with cerebral arterial vasculopathy and present detailed imaging findings.
Case Report
A 9-year-old girl with OI type 4 was admitted to our hospital. She and her family complained about her choreatic movement. Her condition was diagnosed at birth after a dislocated ankle and bowed legs were detected. She weighted 2.5 kg. No family history of OI was present, and the patient had an unaffected brother. She had femoral and radial fractures at the ages of 16 and 20 months, with a total of about six fractures. When the patient was examined at our hospital, she was in the third percentile for height and weight. Her sclerae were blue. Her hearing and dentinogenesis were normal.
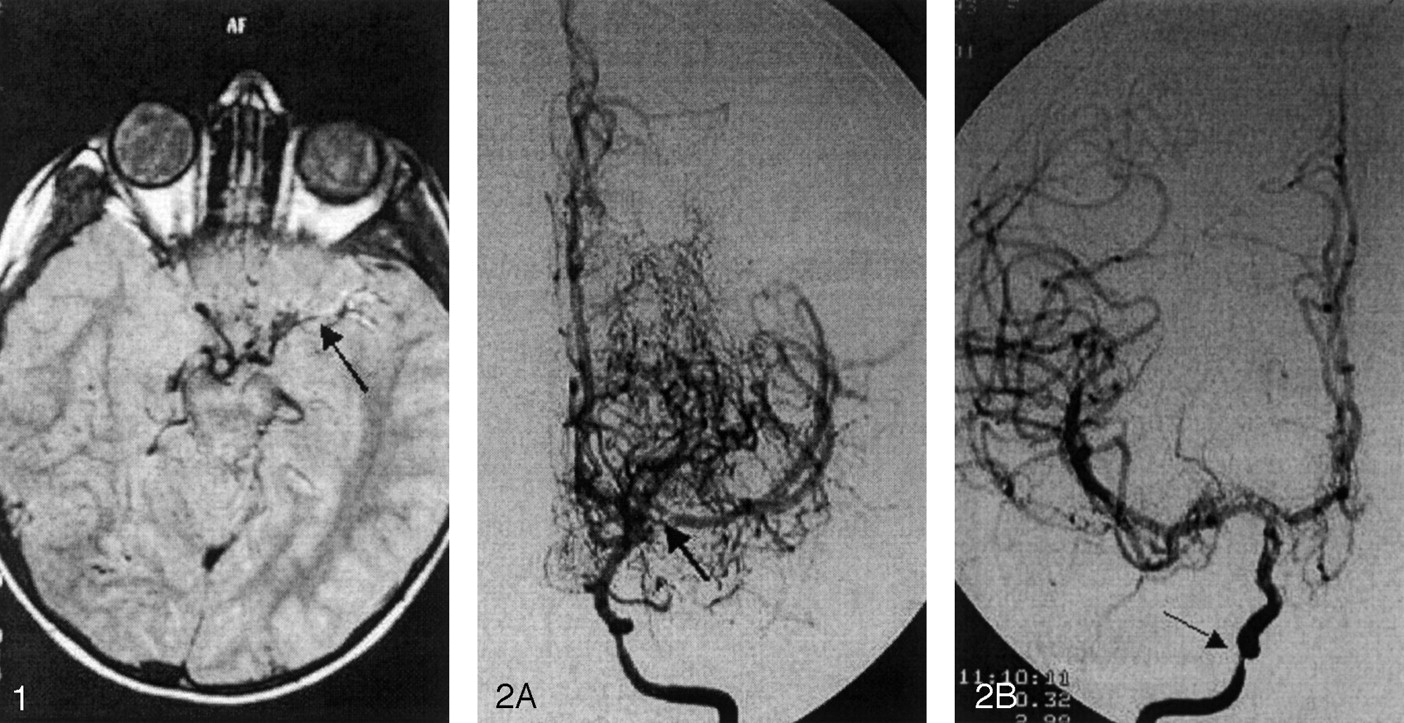
Levels of antistreptolysin-O, fluorescent antinuclear antibodies, and anti-DNA antibodies; seruloplasmine levels; and the erythrocyte sedimentation rate were normal. CT was performed first, and scans showed no abnormality. MR imaging was performed as a further examination because she and her family were still concerned about her involuntary movements. MR imaging revealed some linear, signal-void structures in the right basal ganglial areas and contour irregularities in the left middle cerebral artery (MCA) (Fig 1). Chronic subcortical ischemic changes in the left parietal lobe and prominent perivascular spaces in the bilateral centra semiovale were also noted. A possible vascular abnormality was suspected, and we decided to perform a four-vessel angiographic examination. Cerebral angiography demonstrated bilateral symmetrical stenosis of the proximal cavernous segment of internal carotid artery (ICA), prethrombotic occlusion of the M1 segment of the left MCA, and a moyamoya-like collateral vascular structure arising from the right lenticulostriate arteries (Fig 2). The bone involvement of OI and the secondary carotid canal stenosis were thought to be responsible for the bilateral symmetrical stenosis of the proximal cavernous segment of the ICA. However, high-resolution CT revealed a normal appearance of both carotid canals and other neural foramina. We also detected vasculopathic changes in some distal branches of the MCA and posterior cerebral artery (PCA) and nonperfused areas in the PCA and MCA territories. The blood flow in left MCA territories was supplied by moyamoya-like collateral vascular structure around the left MCA arteries and by the posterior circulation via the PCA. Other causes of cranial vascular diseases were excluded after the clinical and laboratory workup. As a result, these findings were interpreted as vasculopathic changes secondary to vascular fragility caused by the collagen abnormality in OI.

Axial proton density—weighted MR image shows linear, signal-void structures in the right basal ganglial areas and contour irregularities in the left MCA (arrow).
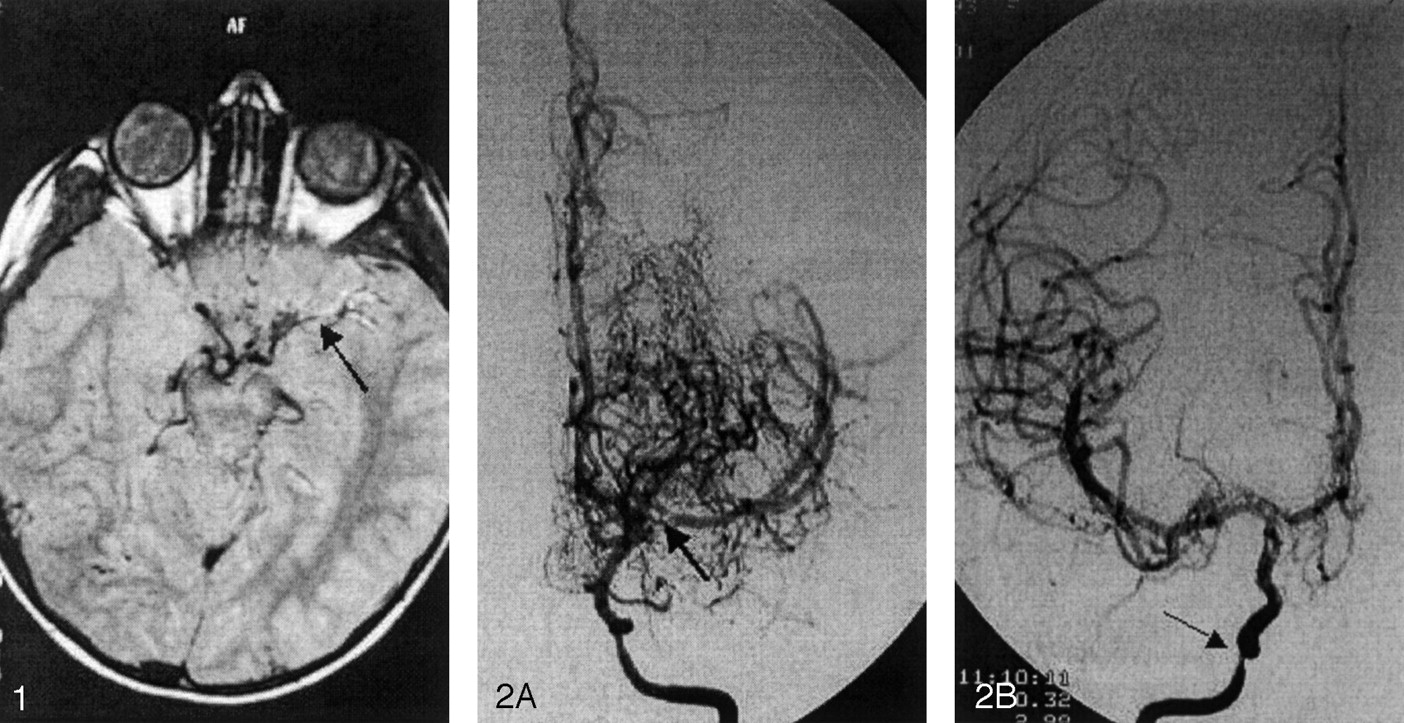
Left ICA angiograms.
A, Anteroposterior projection reveals severe stenosis of the proximal cavernous segment of the left ICA and prethrombotic stenosis (arrow) in the M1 segment of the left MCA. Note the moyamoya-like collateral vascular structure around the proximal portion of the left MCA.
B, Right anteroposterior arteriogram also shows severe stenosis (arrow) of the proximal cavernous segment of the right ICA.
Discussion
OI represents a group of connective tissue defects characterized by bone fragility, and it is known to involve mutations in the genes coding for type 1 collagen (1–3, 8). The disease involves a specific subset of signs and symptoms that depending on the mutation present. According to Sillence (1), four types of OI exist, and each type can be subdivided on the basis of their salient characteristics. OI is associated with type 1 collagen abnormalities caused by a spectrum of mutations in the α-1 chains of procollagen and with decreased synthesis of normal type 1 collagen (4). In OI, histologic findings in bone tissue resemble those of normal fetal osteogenesis, indicating the immature nature of bone affected by OI (9).
Type 1 collagen is normally widely distributed throughout the body, including the perivascular space and the cardiac valves (2). Wheeler et al (2) confirmed the presence of cardiovascular disease in two fetuses with OI by using morphometry and light and electron microscopy. They observed a marked decrease in the adventitial and intramural levels of collagen in the intramyocardial arteries and great vessels. In association with OI, increased aortic root stiffness (10), type I aortic dissection (5), and ulnar artery aneurysm (7) are also reported in the clinical literature. The increased stiffness of the aortic root in the circumferential direction is thought to be consistent with an increased accumulation and cross-linking of collagen within the aortic wall, and this stiffness may reflect premature aging in patients with OI (10). Some authors (7) have suggested a possible association between defective collagen maturation and the pathophysiology of ulnar artery aneurysms in OI.
OI is anecdotally associated with macrocephaly, hydrocephalus, basilar invagination, trigeminal neuralgia, and cerebral atrophy, among other conditions, but little is known about the effects of the abnormal collagen on the vasculature in the CNS (3, 11). In normal cases, type 1 collagen is only sparsely distributed in the fully developed brain. The immunocytochemical localization of type 1 collagen in the normal brain parenchyma shows small amounts near the larger vessels and trace amounts around smaller vessels, with no detectable amounts in the capillaries (3, 8). Among disease of the connective tissue, OI causes complications in the cerebrovascular system less frequently than connective tissue diseases such as Marfan syndrome, Ehlers-Danlos syndrome, or pseudoxanthoma elasticum. However, ruptured cerebral aneurysms associated with fenestrated vertebral arteries, vertebral artery dissections, carotid-cavernous fistulas, and moyamoya-like diseases have been reported in OI (6).
Despite the detailed information about skeletal abnormalities, data about the neurovascular-pathologic involvement of vascular structures in OI are not reported in the literature, at least to our knowledge. Only two recent groups have observed associated CNS alterations. In their reports, Verkh et al (3) and Emery et al (8) reported perivenous microcalcifications associated with proteoglycan-collagen deposits and perivenous calcifications, respectively. We suspect that the bilateral, dilated perivascular spaces on the MR images in our case and the perivenous calcifications in the pathologic material might originate from the same process in OI.
In our case, angiography revealed bilateral and symmetrical stenosis of the proximal cavernous segment of the ICA, severe stenosis of the M1 segment of the left MCA, and a moyamoya-like collateral vascular structure around the left MCA. Bone involvement in OI and secondary carotid canal stenosis (as a cause of the bilateral symmetrical stenosis of the proximal cavernous segment of the ICA) was excluded by means of high-resolution CT. The bilateral carotid canals had a normal appearance on the CT scans. In addition, involvement of the left MCA M1 segment and some distal branches of the MCA and PCA was shown. These findings suggest a general cause of vasculopathy rather than the compression effects due to local changes in the bone at the base of the calvaria. In our case, the moyamoya-like collateral vascular structure around the left MCA might be an interesting finding, one useful in predicting the natural course of this vasculopathy. If vascular disease progresses, especially to distal portion of bilateral ICA, the moyamoya-type vasculopathy will certainly appear in time. We have not found any reports of moyamoya-like changes in the course of OI in the English-language literature. However, in their case report in the Japanese literature, Okamura et al (6) mentioned moyamoya disease occurring as a result of OI.
Results from the clinical studies of the cardiovascular-neurovascular areas mentioned previously, data from the two neuropathologic reports, and the imaging findings in our case suggest that vascular fragility caused by collagen abnormality might affect the cerebral vasculature in patients with OI. However, further study of the exact pathogenesis in the involvement of cerebral vascular structures in OI is needed, especially in the neuropathologic area.
References
- Received May 29, 2002.
- Accepted after revision July 26, 2002.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.