
Abstract
Summary: We report an unusual case of a ruptured aneurysm from an infraoptic anterior cerebral artery in an 11-year-old child. To our knowledge, this is the second such case treated with Guglielmi detachable coils in the pediatric population that has been described in the literature, excluding that of a vein of Galen aneurysm that resulted in remarkable recovery. We conclude that the endovascular technique is a feasible treatment option for children with ruptured cerebral aneurysms, especially when more complex vascular anomalies are present.
The infraoptic anterior cerebral artery (ACA) is a rare congenital vascular anomaly that was first described by Robinson in 1959 (1). Many variations of this anomaly have subsequently been observed, and our search of the literature revealed a total of 21 reported cases. The origin and trajectory of the duplicated segment of the ACA are variable, and the infraoptic type has great significance because of its relationship with the optic nerve and frequent association with aneurysms.
This case illustrates an example of an infraoptic origin of a duplicated ACA associated with a ruptured aneurysm that was successfully treated with Guglielmi detachable coils (GDCs).
Case Report
A previously well 11-year-old boy was found by his mother unresponsive and gasping next to a playground slide. In the emergency room, the patient regained consciousness, vomited several times, and had several episodes of tonic clonic movements of the upper extremities.
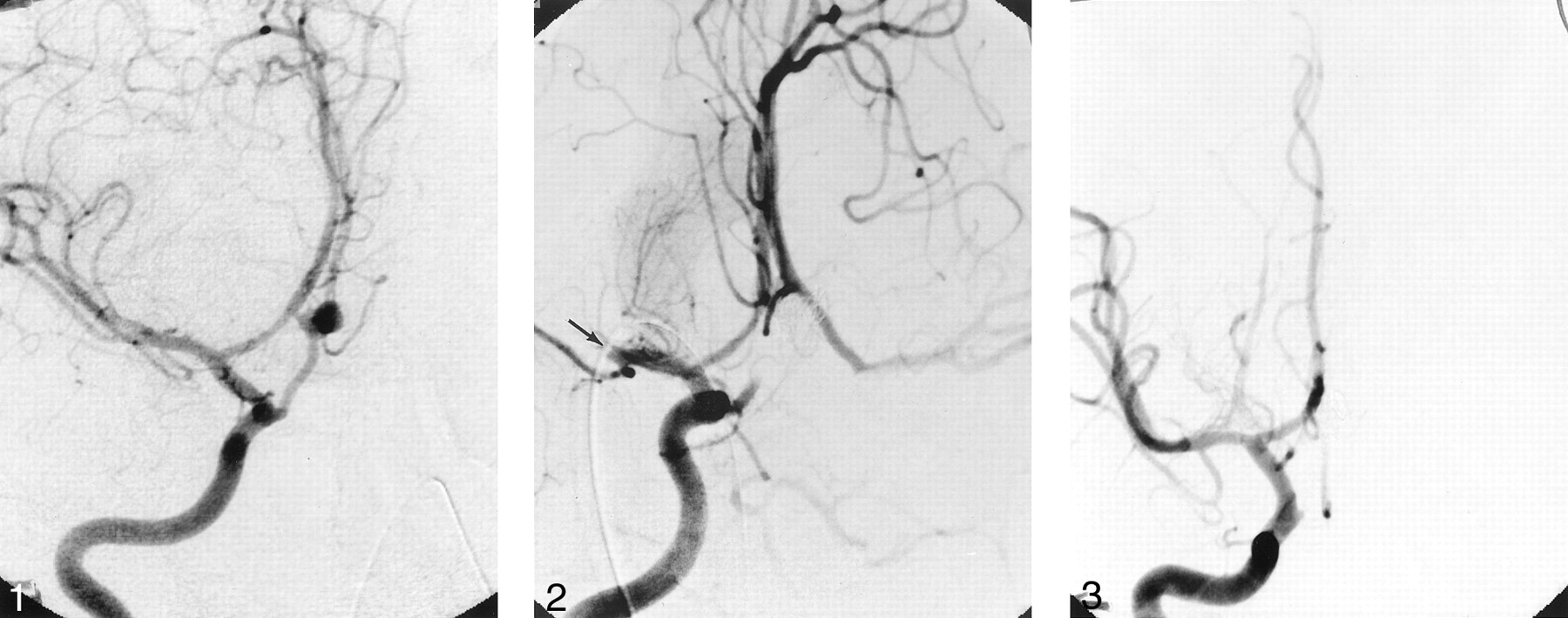
Patient history included long-standing intermittent headaches, always attributed to stress. On clinical examination, he was awake but agitated; his vital signs were normal, and his eyes were deviated to the left side. He had no sign of external injury. He had neck rigidity. Motor and sensory examination findings were normal. A non=contrast-enhanced CT scan of the head showed a diffuse subarachnoid hemorrhage, a small anterior interhemispheric hematoma, and mild hydrocephalus. The subarachnoid hemorrhage was grade III according to the Hunt and Hess classification system. Cerebral digital subtraction angiography (DSA) revealed an aneurysm located along an infraoptic ACA arising from the right internal carotid artery (ICA) near the origin of the ophthalmic artery (Fig 1); the origin of the left ACA was normal. In light of the location and morphology of the aneurysm, it was decided to proceed with endovascular treatment by using GDCs. During the embolization process, the patient received 2500 IU of heparin, and for the next 20 hours the patient received 500 IU/h. After placement of the third coil, during control DSA, a thrombus was noted in the distal M1 segment of the right middle cerebral artery (Fig 2). The clot was immediately dissolved by using 7 mg of intraarterial recombinant tissue plasminogen activator (Activase; Genetech, San Francisco, CA) injected locally, which achieved complete recanalization of the middle cerebral artery and its branches.

Right oblique ICA angiogram depicting the infraoptic ACA and associated aneurysm.
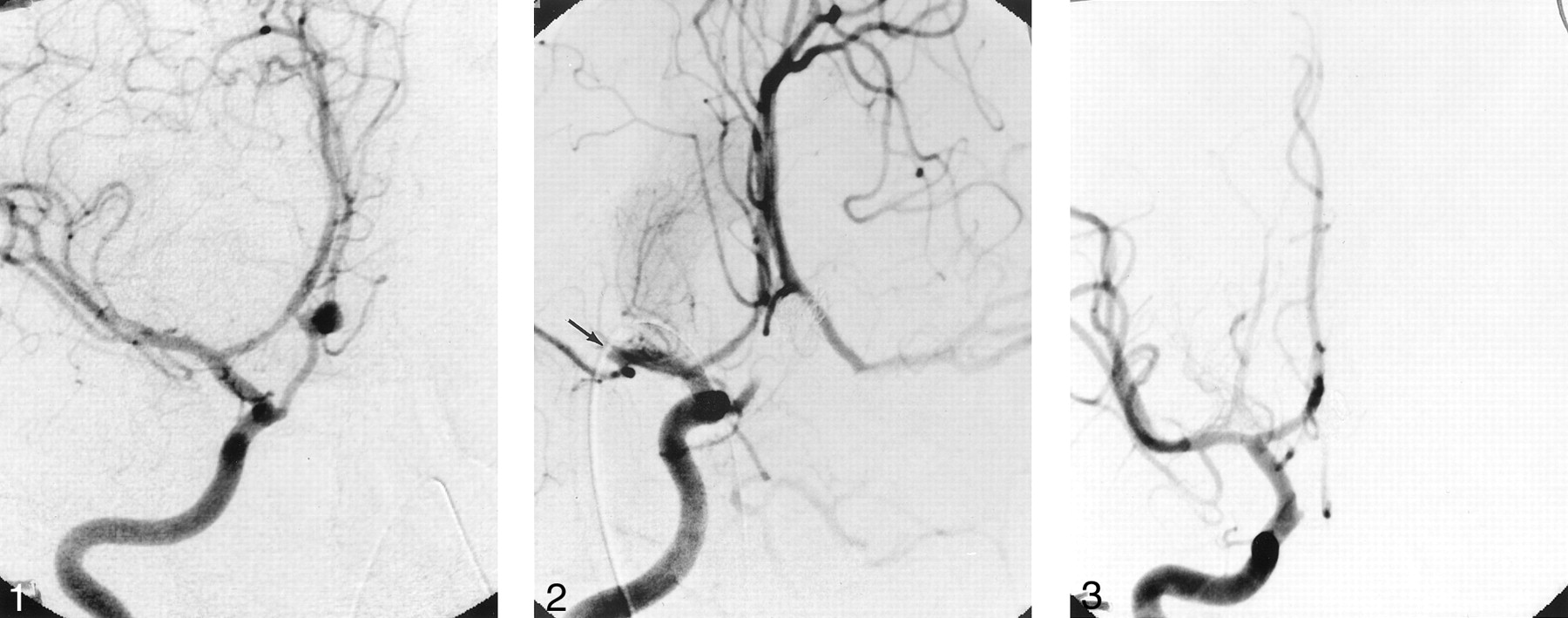
Frontal right ICA angiogram showing complete occlusion of the aneurysm and the infraoptic ACA. Note that the distal M1 segment of the right middle cerebral artery is occluded because of an acute thrombus (arrow).
After total coil placement in the aneurysm, the patient had an uneventful recovery and was discharged 10 days after the procedure. Control DSA was repeated after 3 months (Fig 3), and the examination showed complete obliteration of the aneurysm and the infraoptic ACA and normal middle cerebral artery circulation. The boy resumed his regular school and sports activities within a month of the procedure, and he successfully completed his school year. The 20-month clinical follow-up confirmed complete recovery.

Right ICA angiogram, demonstrating normal anterior cerebral circulation and complete obliteration of the aneurysm and the infraoptic ACA.
Discussion
Infraoptic ACA is a rare vascular anomaly, but it should be recognized by its unique angiographic appearance. This anomalous vessel usually arises from the intradural ICA at or near the origin of the ophthalmic artery and is rarely extradural in origin, according to Curtis (2). The artery then passes beneath the ipsilateral optic nerve and turns, ascending on the midline in front of the optic chiasma. Finally, the infraoptic ACA joins the distal A1 segment of the normal ACA or the anterior communicating artery (3). Twenty-one cases have been reported in the literature (1, 4–10). In 48% of the cases, there was an association with aneurysms: 10 patients presented with subarachnoid hemorrhage secondary to the associated aneurysm (10), and in one case, the subarachnoid hemorrhage was due to unknown cause (5).
In the cases described in the literature (1, 4–9), this anomaly occurs 75% of the time on the right side, 15% on the left side, and 10% bilaterally. Diagnosis was based on autopsy findings in four cases (1, 4), on angiographic and operative findings in nine cases (6, 9), on angiographic studies in seven cases (7, 8), and on angiographic, operative, and autopsy findings in one case (7).
The exact embryogenesis of this vascular anomaly is unclear, but the most logical explanation seems to be related to the persistence of the anatomic loop around the optic nerve of the primitive dorsal ophthalmic artery that, according to Robinson (1), normally disappears as the ophthalmic artery is formed. According to Bosma (7), the anomaly might represent the persistence of the primitive maxillary artery that supplies the optic stalk and cup and terminates at the prosencephalon during the early embryonic stage.
The aneurysms, which have a more proximal origin from the infraoptic ACA, are more difficult to treat surgically, because they are embedded within the cavernous sinus and are very close to several cranial nerves. According to Nutik and Dilenge (10), these aneurysms are difficult to treat surgically because of the inherent nature of the vessel and the aneurysm, which appear to have a thinner wall than normal.
Intracranial aneurysms in children are rare, comprising 0.5–2% of a large aneurysm series (11). Coil embolization of aneurysms in the pediatric population has been reported in only two cases; one by Cekirge et al (11), who reported a treatment of bilateral cavernous carotid artery aneurysms with mechanically detachable coils in a 4-year-old girl, and one by Firat et al (12), who reported a case in which GDCs were used to treat a partially thrombosed giant basilar artery aneurysm in an 11-year-old child who showed remarkable clinical improvement.
Conclusion
Vascular anomalies associated with intracranial aneurysms, even if rare, must be recognized to plan for appropriate treatment. Endovascular technique by using GDCs is a feasible treatment option in pediatric cerebral aneurysms, especially when an unusual vascular anomaly is coexisting, as in the case illustrated here.
- Received May 13, 2002.
- Accepted after revision October 3, 2002.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.