
Abstract
Summary: Giant and fusiform aneurysms of the basilar artery (BA) are difficult to manage surgically, and they still present a challenge for the neurosurgeon despite progress in posterior fossa surgery. Guglielmi detachable coils have provided an alternative approach to treatment, but they have their own difficulties. We present a series of three patients with BA aneurysms treated with endovascular occlusion of the aneurysm and basilar trunk. Our experience suggests that, in select cases, BA occlusion may be not only safe but also necessary for the effective treatment of these aneurysms.
Posterior circulation aneurysms present unique problems for both the neurosurgeon and the interventionist. Challenges include difficulty with the surgical approach; the frequent occurrence of broad-necked, fusiform or giant aneurysms; and the incorporation of the branches of the basilar artery (BA). Approximately 8% of giant aneurysms occur in the posterior circulation. These aneurysms have a poorer prognosis than that of typical saccular aneurysms. One group (1) documented a 5-year incidence of severe morbidity and mortality of 80%.
Reports of complete surgical and/or endovascular occlusion of these aneurysms with BA occlusion are few. We believe that, in certain cases, endovascular occlusion of the aneurysm sac and BA trunk can offer a lasting cure for patients with these aneurysms.
Case Reports
Case 1
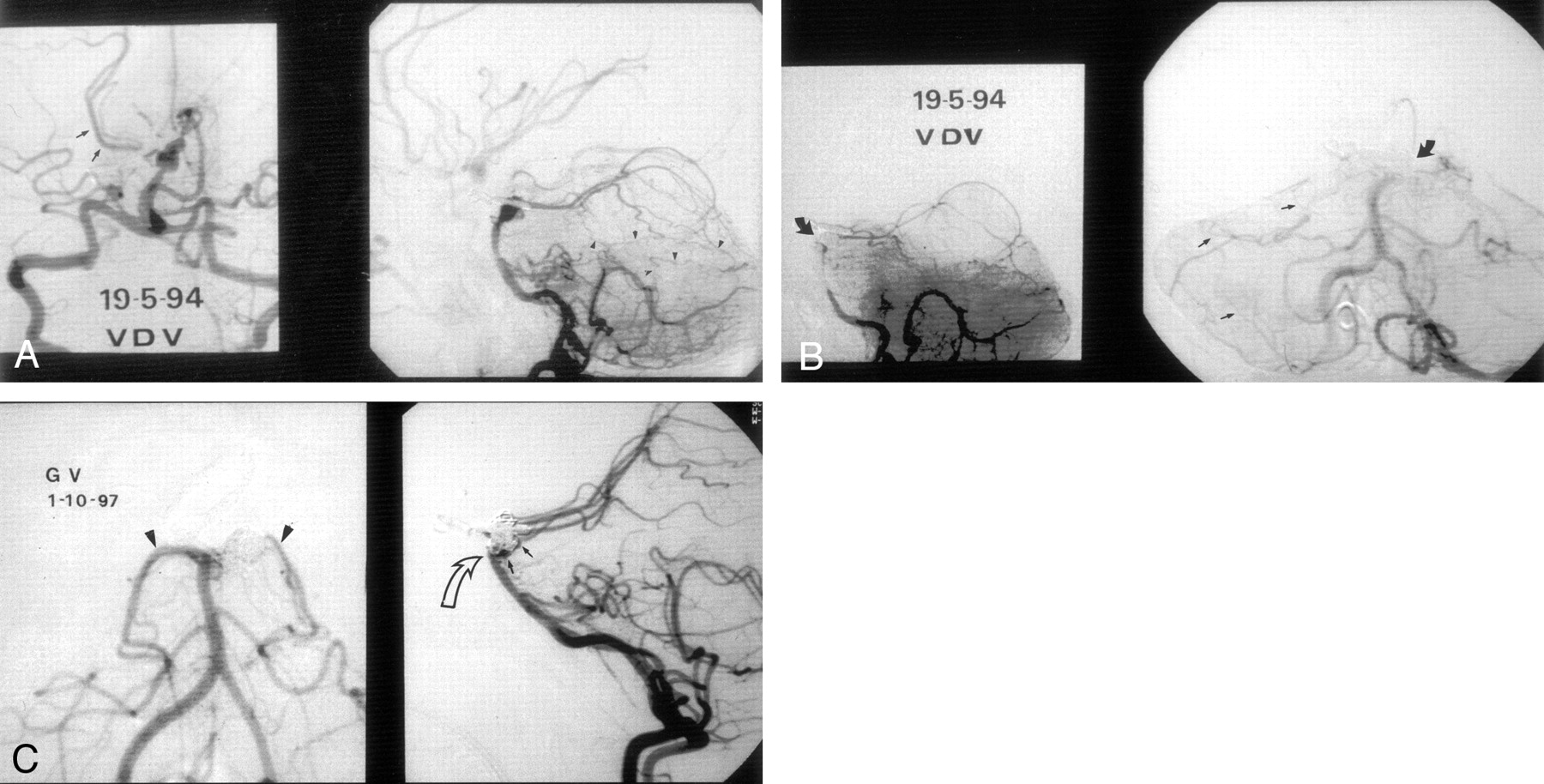
A female patient aged 18 months presented to another institution with subarachnoid hemorrhage (SAH) due to rupture of a large aneurysm of the distal BA. Emergency clip placement was performed, and the patient recovered uneventfully. However, 10 months later, recanalization of previously occult aneurysmal loculi had occurred, and further attempts at surgical treatment were unsuccessful. One year after the initial presentation, the patient was referred to our institution for an opinion with a view to endovascular therapy. An initial angiogram showed no filling of the posterior cerebral arteries from the BA and an occlusion of the left superior cerebellar artery (SCA) at its origin, with good collateralization of its territory from the left anterior inferior cerebellar artery (AICA) and the posterior inferior cerebellar arteries (Fig 1A). The aneurysm was then occluded with two coils. This procedure resulted in occlusion of the right SCA, but substantial collateralization of its territory was already present (Fig 1B). A heparin infusion was continued for 36 hours, after which the patient was awakened. She showed no signs of posterior circulation ischemia and remained well after her discharge from the hospital. Angiography preformed 6 months later showed recanalization of additional previously occult aneurysmal loculi and the right SCA. These loculi were also occluded with coils, resulting in reocclusion of the right SCA and thrombosis of the BA trunk to a point 1–2 mm below the coil mass. Carotid angiographic results confirmed filling of both PCAs via large posterior communicating arteries (PCoAs). She awoke with no new neurologic deficits. Angiograms obtained 4 years after her last treatment showed a miniscule aneurysm remnant, with no change in configuration of the coil mass (Fig 1C). Both SCAs filled normally from the BA, but the distal BA remained occluded. She has remained well as of this writing.
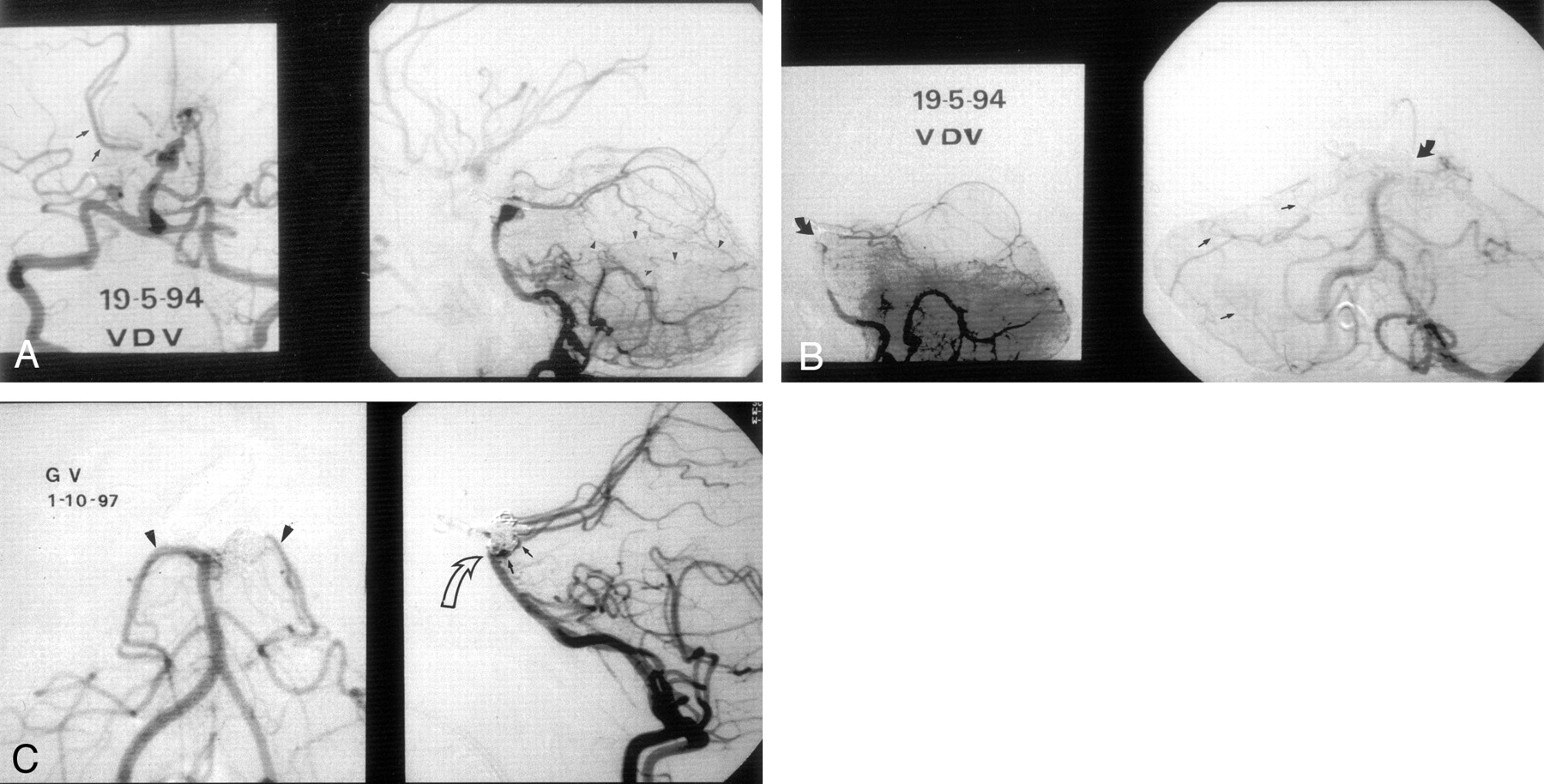
Anteroposterior digital angiography, right VA injection, performed after attempted wrapping of the aneurysm, immediately prior to coiling (A). There is no filling of the PCAs via the BA. The RSCA is patent (small arrows), but the LSCA is occluded at its origin. An extensive network of collateral vessels is already evident, arising from the left AICA and PICA (arrowheads). Following the first coiling, no residual filling of the aneurysm is seen (B). The coil mass (curved arrows) occludes the distal BA trunk, and flow in the RSCA is no longer evident. Several collateral vessels (small arrows) from the right AICA and PICA are present. Angiography 3 years following the last procedure (C), shows continued near-total aneurysm occlusion, with only a miniscule amount of body filling (small arrows). Both SCAs have recanalised, but the BA tip remains occluded between the SCA origins and the BA bifurcation (open, curved arrow).
Case 2
A 17-year-old male adolescent presented with SAH due to a fusiform BA aneurysm located between the AICA and SCA origins (Fig 2A). An attempt at surgical obliteration was unsuccessful. The patient gradually recovered from his initial bleeding episode, but he was left with residual altitudinal diplopia and a mild right ptosis. He presented to our institution for endovascular treatment 5 months later. BA occlusion was considered a probable outcome of endovascular treatment, as a result of the fusiform configuration of the aneurysm. However, because he had large PCoAs, this was thought to be a reasonable therapeutic proposition, given his otherwise poor long-term prognosis. Therefore, the aneurysm was catheterized and occluded with three coils. After coiling, the aneurysm was completely occluded, but several coil loops protruded into the adjacent BA. However, flow persisted through the coil basket. The patient awoke with mild weakness in the right arm and leg, as well as his preexisting deficits. He then became drowsy and developed moderate ataxia and dysarthria. Nonenhanced CT performed at 48 hours showed a peripheral area of hypoattenuation in the left cerebellar hemisphere, consistent with a focus of cytotoxic edema. His condition stabilized, then improved over the next 72 hours. Angiography performed on day 7 showed a short segment of BA occlusion between the AICA and SCA origins (Fig 2B), with excellent filling of the distal BA from a large PCoA. CT performed on the same day showed no evidence of cerebellar or cerebral infarction, with resolution of the changes seen on the previous study. The patient continued to improve rapidly, and he was discharged home on day 11, having regained his prior level of neurologic function. Angiography performed at 4 months (Fig 2C) showed persistent occlusion of the aneurysm and BA, and he remained well. Follow-up studies performed elsewhere have confirmed a lasting therapeutic outcome. He remained well and had returned to work as a computer programmer.

Lateral digital subtraction angiography, left VA injection, performed prior to endovascular treatment (A). A fusiform aneurysm affecting the middle of the BA is shown (solid arrow). Angiography, AP projection, left VA injection, performed on day 7 after coiling (B), shows tapering of the proximal BA leading to a short segment of occlusion (long arrow) between the AICA and SCA origins. Some collateral vessels are seen arising from the PICAs and AICAs.
Angiography performed 4 months after coiling (C) shows persistent occlusion of both the BA and the aneurysm.
Case 3
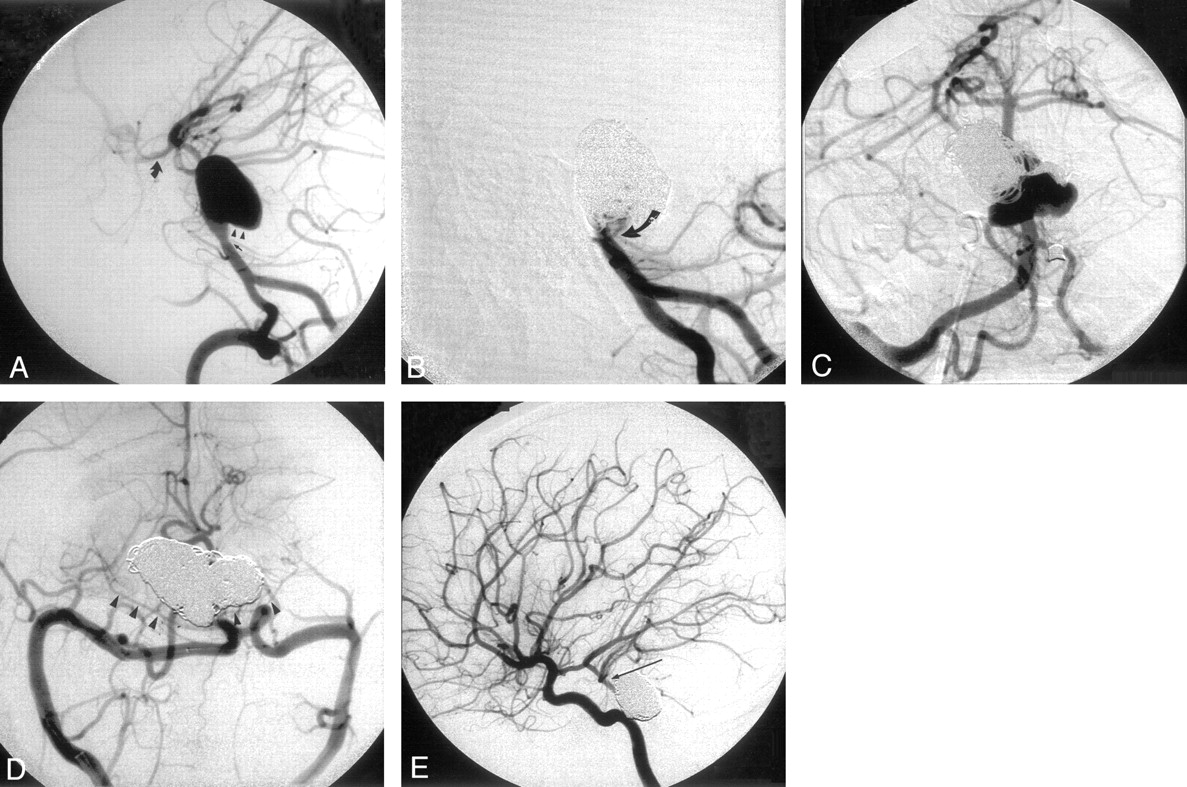
An 11-year-old boy presented to our institution with headache, right hemiparesis and dysarthria. MR imaging, MR angiography, and conventional angiography showed a giant fusiform aneurysm of the BA extending from the origins of the AICAs to the midbasilar trunk (Fig 3A). A stent-assisted endovascular approach was considered inappropriate because of the absence of a suitable location for stent deployment. Large PCoAs were present, however; therefore, coil occlusion of the aneurysm was undertaken with a view to occluding both the aneurysm and the affected BA segment. The aneurysm was catheterized and filled with 18 coils, resulting in almost complete obliteration of the aneurysm and occlusion of the midbasilar artery (Fig 3B). A small residual pocket of aneurysm appeared to give rise to the AICAs, which remained patent. As a result, no attempt was made to occlude this part of the aneurysm. The distal BA and its branches filled normally from the PCoAs. The patient awoke with no new deficits, and his existing signs and symptoms had regressed by 6 weeks. He was discharged from the hospital several days later, with a prescription for oral aspirin 150 mg daily. Follow-up angiography performed at 2 months showed reestablishment of the BA lumen, evidence of coil compaction, and recanalization of previously thrombosed aneurysmal loculi (Fig 3C). The patient underwent a second treatment session at 4 months. The residual aneurysm was catheterized, and 13 coils were deployed. Care was taken to preserve the AICAs, which arose close to the inferior aspect of the aneurysm. The final angiogram showed filling of both AICAs, complete obliteration of the aneurysm, and occlusion of the BA (Fig 3D), with good filling of the distal BA from the PCoAs (Fig 3E). The patient awoke with no deficit. His most recent angiogram, obtained 6 months after the second procedure (not shown), demonstrated complete occlusion of the aneurysm sac and recanalization of the BA trunk. He had returned to school and remained active and well with no neurologic sequelae.

Oblique digital subtraction angiography, right VA injection, performed at the time of presentation (A). A giant fusiform aneurysm of the BA is shown. Although the AICA origins are apparently separate from the bulk of the aneurysm, the left AICA originates from the junction of normal and ectatic vessel (small arrow). The straight configuration of the inferior aspect of the aneurysm sac suggests the presence of intra-aneurysmal thrombus (arrowheads). Note the large left PCoA (short curved arrow). Following deployment of 18 coils (B), near-total occlusion of the aneurysm sac is shown. A small amount of residual inferior body filling was accepted due to the proximity of the left AICA origin to this loculus (curved arrow). The BA trunk is occluded, and continued filling of the distal BA and PCAs via the PCoAs was confirmed on bilateral ICA angiography (not shown). Angiography performed prior to the second coiling procedure, 4 months after initial presentation (C). There has been aneurysm recanalisation and coil compaction. The BA has recanalised. Angiography performed after the second coiling procedure (D). The BA trunk has been reoccluded. No residual aneurysm filling is seen, and the AICAs have been preserved (arrowheads). Lateral right ICA angiograms (E) confirms good filling of the PCAs and the distal BA via a large PcoA (long arrow).
Discussion
Giant aneurysms, particularly those in the posterior circulation, remain a daunting prospect from both the neurosurgical and endovascular standpoints. Patients with these aneurysms continue to have a poor long-term prognosis. Several series in the neurosurgical literature have demonstrated limited success in treating BA trunk aneurysms, but few workers have attempted definitive exclusion of the aneurysm sac combined with BA trunk occlusion.
Published series by Steinberg et al (2), Drake and Peerless (1), Drake (3), and Pelz et al (4) have shown limited success with BA ligation or aneurysm trapping. In these series, good or excellent outcomes were achieved in around 65–70% of cases, with severe morbidity and mortality of around 30–35%. Although there is no doubt that surgery has some theoretical advantages over endovascular treatment in the management of giant BA aneurysms, surgery within the confines of the posterior fossa poses substantial risks of trauma to the cranial nerves and vital brainstem structures, even in the most experienced hands. Rates of non-neurologic morbidity, such as deep venous thrombosis, are also higher for surgery than for endovascular therapy.
Endovascular treatment offers a relatively noninvasive means of approaching posterior fossa aneurysms, but reports of endovascular occlusion of giant BA aneurysms with BA trunk occlusion are few. Hodes et al (5) and Aymard (6) have described successful treatment of BA aneurysms with balloon occlusion of the BA or vertebrobasilar junction respectively. In a series by Uda (7), five BA aneurysms were successfully treated with unilateral or bilateral vertebral artery coil occlusion. Most recently, Jones et al (8) published a case report describing successful endosaccular treatment of a giant BA aneurysm with BA trunk occlusion.
In determining the safety of BA occlusion, the most important factor to be taken into account is the presence and size of the PCoAs. Steinberg et al (2) showed that patients with two large (>1 mm) PCoAs had better outcomes than those of patients with one large and one small (<1 mm) PCoA and patients with two small PCoAs. Therefore, before occlusion of the BA during therapy is considered, documentation of the presence and size of the PCoAs is essential.
Assessment of aneurysm morphology is also critical. In the case of BA aneurysms, it is highly likely that many of the brain stem perforators incorporated into the aneurysm sac are occluded by thrombus at the time of diagnosis and that involved perforating artery territories are already supplied by collateral circulation. The latter was certainly evident in our cases. When not occluded by thrombus, these perforating arteries may be either deficient or disrupted by the traction forces applied to them as the aneurysm expands away from the brain stem. However, irrespective of the integrity of incorporated perforators, the capacity of leptomeningeal and other minor collateral pathways is remarkable, as has been noted by other investigators (1).
The best long-term results with endovascular treatment are achieved with obliteration of the aneurysmal inflow zone (9). This prevents recanalization due to shearing forces directed along the interface between the coil mass and the aneurysm wall (9–11). Giant or fusiform BA aneurysms present a dilemma in that the inflow zone often comprises most or all of the circumference of the BA itself, and the extensive inflow zone cannot be obliterated without notable coil prolapse or occlusion of the BA.
It is also worth noting that multiple or staged treatments should not be considered treatment failure, especially in the context of a condition with such a poor prognosis. In many areas of interventional neuroradiology, recurrent disease and staged therapy are considered normal and predictable. Therefore, it is perhaps not appropriate to directly compare treatment aims and outcomes for giant or fusiform BA aneurysms with the treatment goals for conventional saccular aneurysms; in many respects, these represent an entirely different disease entity.
Conclusion
Coil occlusion of giant or fusiform BA aneurysms with BA trunk occlusion offers a safe and potentially long-lasting cure for aneurysms of this type. Surgical alternatives in such cases are severely limited by technical difficulties and operative morbidity and mortality. Endovascular treatment requires meticulous evaluation of aneurysm morphology and of the PCoAs and minor collateral pathways of the posterior circulation before this treatment option is considered. In some cases, multiple treatment sessions may be necessary to achieve a complete or acceptable result. Moreover, it is likely that, with further advances in stent and coil technology and continuing improvements in endovascular techniques, even more effective treatment will be possible in the near future.
References
- Received November 15, 2002.
- Accepted after revision January 21, 2003.
- Accepted after revision January 21, 2003.
- Copyright © American Society of Neuroradiology




{kind=link}
{kind=link}
{kind=link}