
Abstract
Summary: We simultaneously injected both internal carotid arteries (ICAs) during 3D rotational digital subtraction angiography in a patient with a ruptured anterior communicating artery (Acom) aneurysm and vasospasm. Shaded surface display (SSD) images from this acquisition provided more anatomic detail than did SSD images created from individual ICA 3D rotational digital subtraction angriography. In the evaluation of complex Acom aneurysms, this technique can facilitate the choice of optimal working projections for safer aneurysm coiling.
With increasing clinical application, 3D rotational cerebral angiography helps overcome the limitations of 2D angiography by more efficiently and more definitively visualizing aneurysm anatomy (1–6). We present a case of an extended application of 3D rotational angiography. In a patient with a ruptured anterior communicating artery (Acom) aneurysm and vasospasm, both internal carotid arteries (ICAs) were simultaneously injected during 3D rotational angiogram acquisition to more clearly define complex aneurysm and adjacent vessel anatomy before endovascular treatment.
Case Report
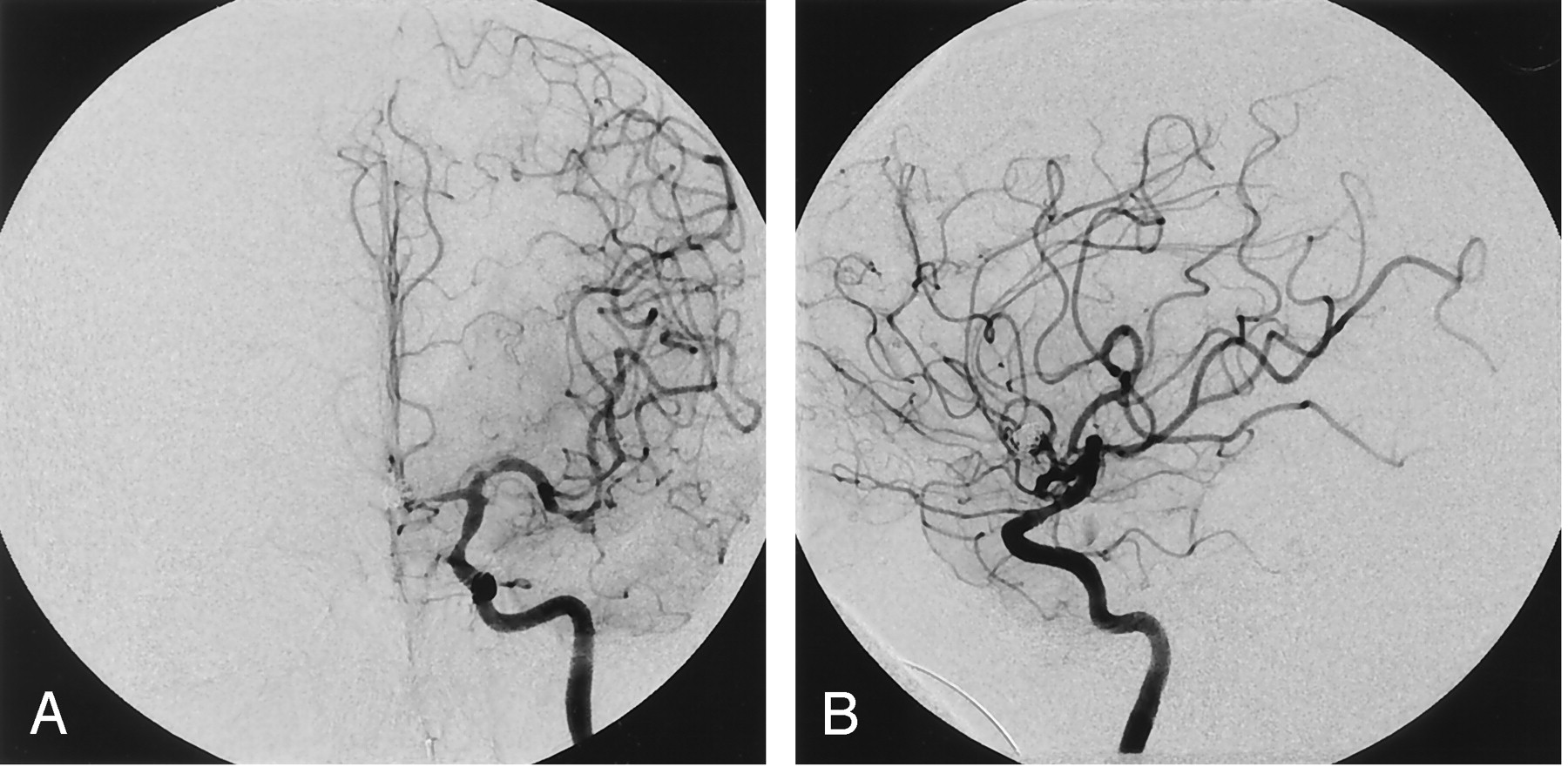
A 48-year-old right-handed man collapsed at home from a subarachnoid hemorrhage. On examination, the patient was lethargic with left hemiparesis. Cerebral angiography showed a complex Acom aneurysm and vasospasm (Fig 1A and B). The aneurysm appeared to originate at the junction of the right A1 segment and a prominent callosomarginal artery originating from the base of the aneurysm. Left internal carotid injection showed the left A2 segment seeming to originate from its proximal neck.

Left ICA angiogram, frontal (A) and lateral (B) oblique projections, show Acom aneurysm associated with severe distal A1 and A2 segment vasospasm.
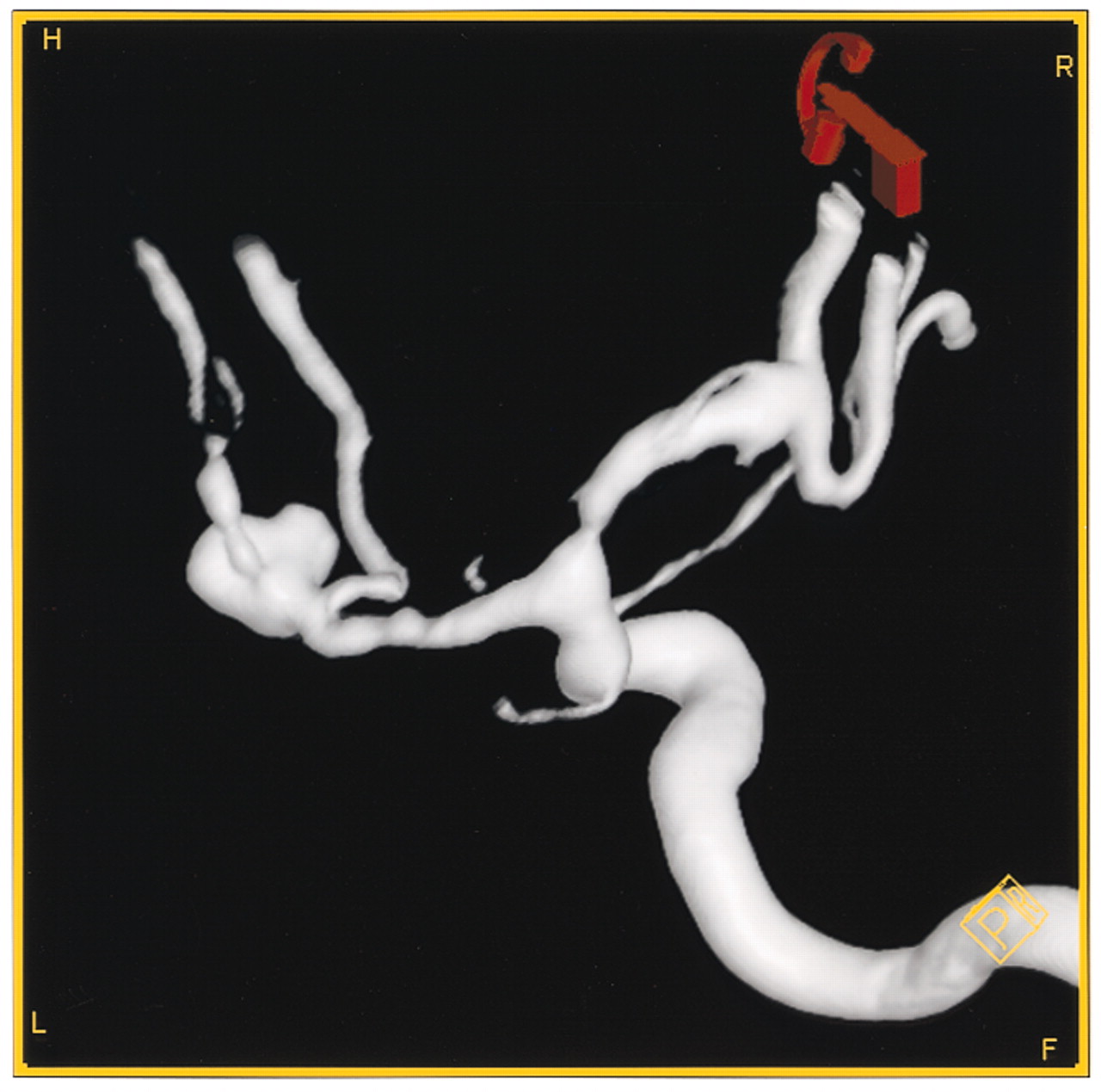
We performed 3D rotational angiography by injection of contrast medium into the right and left ICA separately (Siemens Biplane, Axiom Artis BA; Leonardo InSpace workstation, Erlangen, Germany). The resultant 3D shaded surface display (SSD) reconstruction (Fig 2), however, showed incomplete visualization of the complete aneurysm and adjacent arteries. Because of the midline location of this aneurysm, the frequent competing flows at the Acom level, superimposed vasospasm, and the complex anatomic relationships of the different vessels near the aneurysm, we performed simultaneous bilateral ICA 3D rotational angiography (Fig 3A). By using bilateral groin percutaneous access, separate catheters were placed into each ICA. One catheter was connected to a power injector with injection of 3 mL/s for 7 seconds while the other ICA catheter was simultaneously hand-injected with 20 mL of contrast medium. The resultant 3D SSD better showed the relationship of the base of the aneurysm to both A1 segments of the anterior cerebral arteries, left A2 anterior cerebral artery (ACA) segment, and branches of a prominent right callosomarginal artery arising from the base of the aneurysm (Fig 3B).
Left ICA oblique angiogram during 3D rotational angiography shows attenuation of the distal A1 segment and the complex Acom aneurysm. The SSD reconstructions did not convincingly reveal the relationship of the aneurysm and the adjacent anterior cerebral artery vessels.

Simultaneous bilateral ICA injections during 3D rotational angiogram acquisition reveal heart-shaped Acom aneurysm and both A1 segments (A). 3D SSD reconstructions from the simultaneous bilateral ICA injection 3D rotational angiogram shows clearly the relation of the aneurysm and both A1 segments as well as the right callosomarginal artery branches arising from the base of the aneurysm (B).
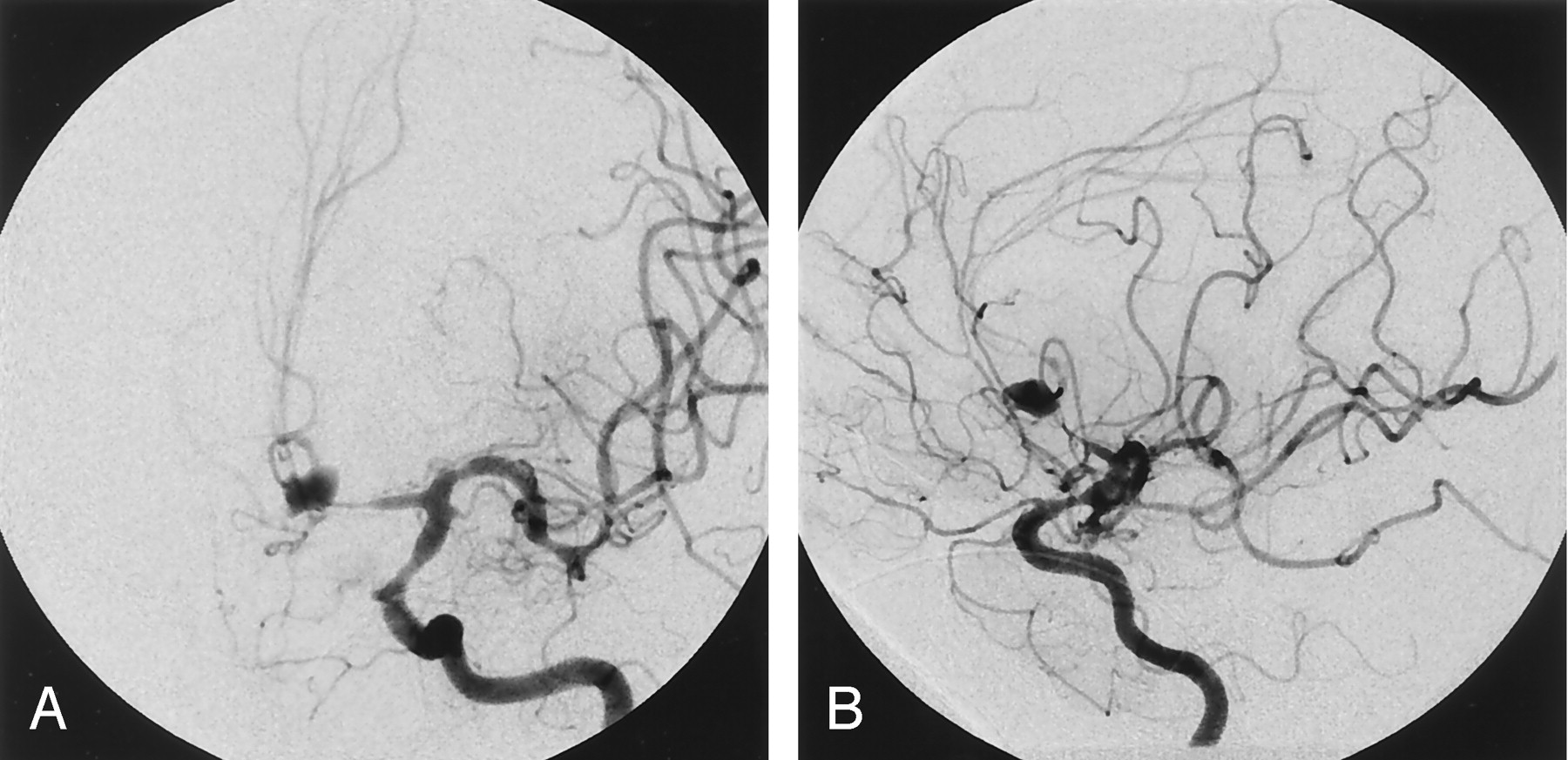
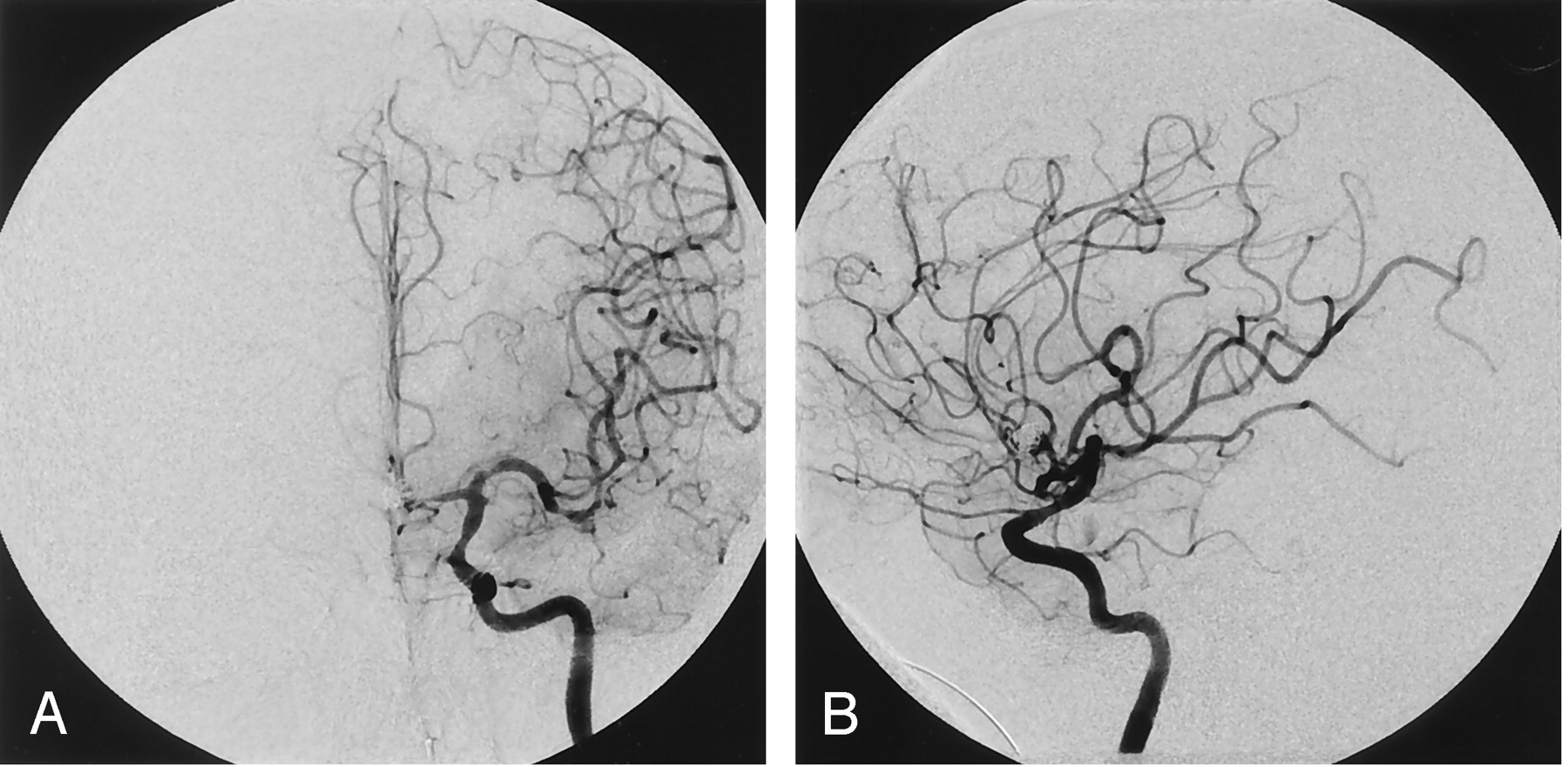
With this additional knowledge, we were able to occlude the aneurysm successfully with coils, while preserving both the anterior cerebral arteries (Fig 4A and B). The patient made a significant recovery and was discharged to a rehabilitation facility, independently caring for himself and ambulating with a stable mild left hemiparesis.
Postcoiling left ICA angiograms, frontal (A) and lateral (B) projections, show aneurysm occlusion and preservation of the left ACA branches, including opacification of both pericallosal arteries.
Discussion
3D rotational digital subtraction angiography with SSD display provides significantly more detailed information for evaluating cerebral aneurysms than that provided by the conventional 2D technique (1–6). 3D rotational angiography is performed with the injection of a target vessel such as an ICA or vertebral artery, usually with a power injector (1–6). In almost all cases with patients who are cooperative or who are under general anesthesia, where patient motion does not degrade the reconstructions, standard protocols are sufficient to produce adequate anatomic images for endovascular decision-making. In our case, however, because of vasospasm and anatomic variation in pericallosal and callosomarginal origins, standard 3D rotational angiography of each ICA did not cross-fill the other A1 segment.
Although the technical possibility of cross-compression of the contralateral carotid artery during 3D rotational angiography has been mentioned, cross-compression for Acom aneurysms has not been performed in any series (1). Cross-compression was considered in our case; however, considerations of operator exposure to radiation and creating misregistration artifact during rotation of the image intensifier dissuaded us from cross-compression. In patients with a complex unruptured Acom aneurysm, good-quality CTA can provide similar information and can be obtained before treatment. In patients with an acutely ruptured aneurysm, however, obtaining a CTA immediately before angiography is rarely performed.
Conclusion
Simultaneous bilateral ICA 3D rotational angiography can be a useful technique in the pretreatment evaluation of complex Acom aneurysms. Simultaneous different-vessel-injection 3D rotational angiography may be useful in the real-time treatment evaluation of selected brain arteriovenous malformations, dural fistula, and facial malformations.
References
- Received April 19, 2004.
- Accepted after revision May 19, 2004.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.