
Abstract
Summary: The case of a 24-week-old fetus that showed features suggestive of focal cortical developmental anomaly at prenatal MR imaging is presented. The anomaly was confirmed to be polymicrogyria by 34-week prenatal and the 3-day postnatal MR imaging studies. The report demonstrates that the development of polymicrogyria can be assessed throughout different stages by prenatal MR imaging. In the case reported, the additional presence of periventricular heterotopia strongly suggests that a neuronal migration alteration coexisted with a postmigrational disorder.
Prenatal MR imaging is widely used to confirm prenatal sonography (US) findings in cases of major and complex fetal brain malformations (1). Minor focal abnormalities of cortical development (ie, focal polymicrogyria) usually are not detectable by prenatal US. Very little information concerning prenatal MR imaging detection of cortical developmental anomalies is available (1, 2), especially about focal rather than extensive anomalies in fetuses <30 weeks old.
We present the case of a 24-week-old fetus that showed features suggestive of focal cortical developmental anomaly at prenatal MR imaging. The anomaly was confirmed to be polymicrogyria by 34-week prenatal and 3-day postnatal MR imaging studies.
Case Report
A 17-year-old woman, gravida II, para I (healthy child), was referred to our MR imaging service at 24 weeks’ gestation because a transabdominal US examination, performed a week earlier, had shown moderate bilateral ventriculomegaly (atrial width of 12 mm) without additional abnormal intracranial findings. Body biometric measurements were within normal limits. The pregnancy had been complicated by moderate vaginal bleeding during the first trimester of gestation. There were no serological signs of intrauterine infections. The woman’s guardian signed the prenatal MR imaging consent form in use at our institution. The prenatal MR imaging was performed with a 1.5-T system (Horizon-LX, Echo-speed, GE Medical Systems, Milwaukee, WI) and a flexible surface coil. Single-shot fast spin-echo (FSE) multiplanar images (field of view [FOV], 30 cm; matrix, 256 ×192; TR/TE, 4000/90 ms; section thickness, 3–4 mm) were acquired at the fetal brain level (Fig 1). The study confirmed the presence of mild bilateral ventriculomegaly; it also showed the absence of septum pellucidum. Posterior fossa anatomy was unremarkable. At the posterior frontal level of the left hemisphere, an unclear cortical-rim profile, wartlike irregularity was noticed. A small nodule of low T2 signal intensity was also visible in the periventricular region beneath the suspected focal cortical rim abnormality. Moreover, a thin line of low T2 signal intensity seemed to extend from the nodule toward the cortex. Because the absence of septum pellucidum has frequently been described as associated with monolateral or bilateral schizencephaly and cortical polymicrogyria (3), and frontal cortical findings were highly suspicious, it was decided to investigate the fetal brain at a later stage of development. A second prenatal MR imaging study was performed at 34 weeks’ gestation (Fig 1). At this time, US showed normal ventricular size (atrial width of 9 mm) and absence of the septum pellucidum. The second prenatal MR imaging study confirmed both US findings and the presence of a focal cortical rim abnormality (excessive gyral infolding and tightness) in the left posterior frontal lobe. At 39 weeks’ gestation, a male neonate was born by uncomplicated vaginal delivery. Neurologic status and findings were normal, with the exception of episodes of fine tremor and moderate hypertonia of upper and lower limbs. The electroencephalographic pattern was normal. No body anomalies were noted, with the exception of mild pulmonary artery stenosis at Doppler US.
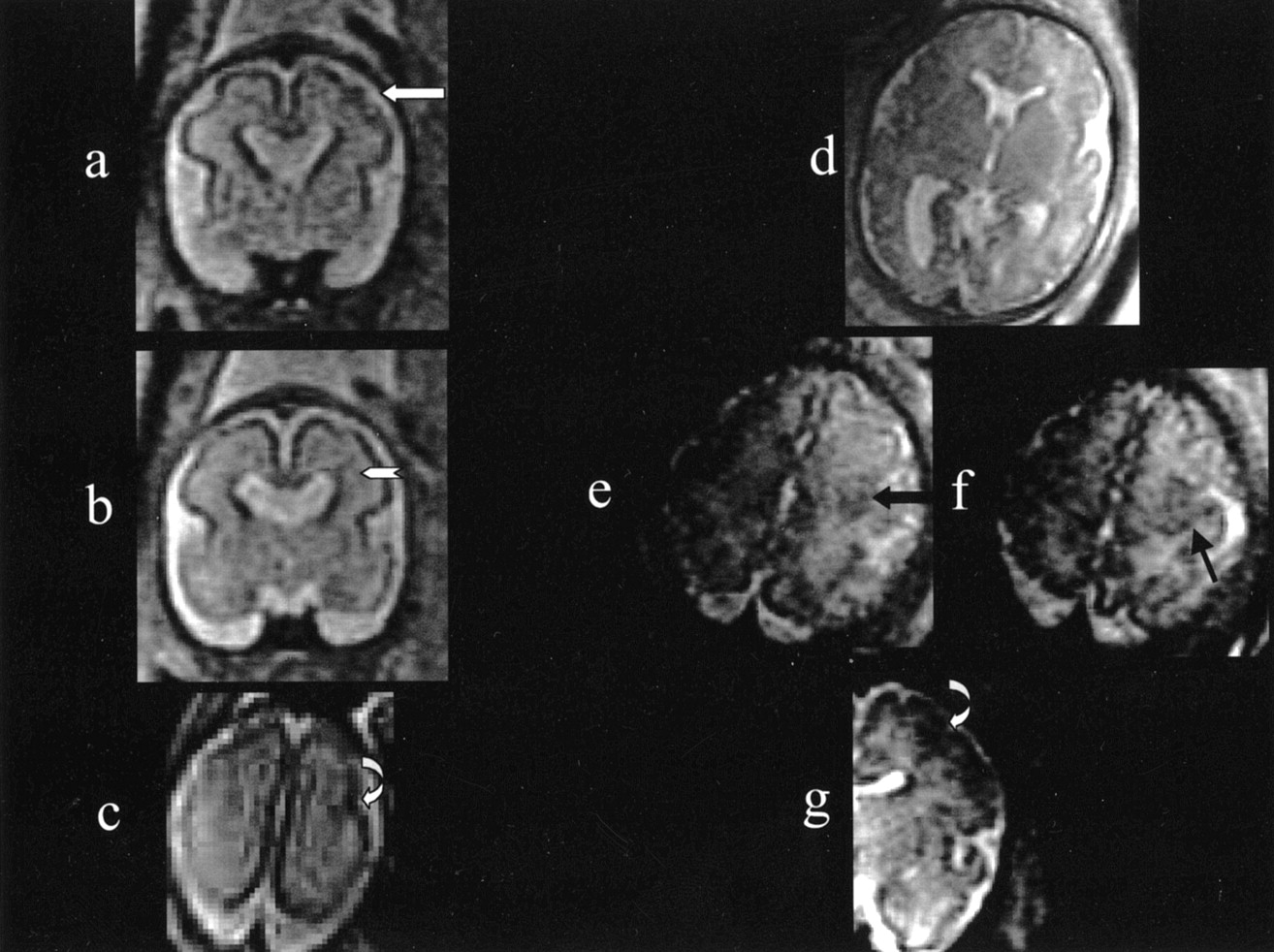
Multiplanar T2-weighted single-shot fast spin-echo sections from 24-week (A–C) and 34-week (D–G) gestational age.
A, Coronal section showing absent septum pellucidum and focal irregular wartlike profile of the cortical rim in the left hemisphere (white arrow).
B, Contiguous coronal section depicting a small hypointense subependymal nodule associated with a thin hypointense line extending toward the cortex (white arrowhead).
C, Axial section showing an unclear area of cortical-rim abnormal profile with apparent irregular infolding in the left hemisphere (curved white arrow).
D, Axial section depicting the absence of septum pellucidum.
E (left) and F (right), Axial contiguous sections from the same study showing in the left posterior frontal lobe a focal area of abnormal cortical-rim profile with some irregular infolding (black arrow).
G, Coronal section from the same study depicting in the left frontal lobe the same area of irregular and abnormally tight cortical gyri infolding (curved white arrow). Only the left half of the section has been reproduced, to eliminate the dynamic windowing problems related to the high signal intensity in the right side of the image, caused by the proximity to the surface coil.
At 3 days of age, a brain MR imaging was performed, by using the same system of prenatal studies (Fig 2). Three-millimeter-thick axial and coronal FSE T2-weighted sections were acquired (FOV, 16 × 12 cm; matrix, 320 × 320; TR/TE, 6000/200 ms). T1-weighted sections were also acquired, but they were of low quality because of motion artifact image degradation. The MR imaging confirmed the absence of septum pellucidum and the mild bilateral lateral ventricle enlargement. In the posterior frontal cortex, in the left hemisphere, an area of abnormal cortical gyri, with increased convolution and tightness, was clearly visible. Similar cortical findings, albeit less clear and less extensive, were also noticeable in the same location of the contralateral hemisphere. In the subependymal region underneath the left frontal cortex abnormality, a nodule of heterotopic gray matter was also clearly visible. No other cerebral hemispheres or posterior fossa abnormalities were present. The optic nerves, chiasm, and the hypothalamic-pituitary region appeared to be normal. At the 2-month clinical follow-up, the neurologic examination was completely normal. On this occasion, the fundus oculi was inspected and found to be normal. The karyotype was also normal, as was the electroencephalographic pattern. No seizure episodes were reported.

Three T2-weighted coronal FSE sections from the postnatal MR imaging study. A focal area of abnormally tight cortical infolding at the left frontal lobe cortex level is visible (white arrows). A much less extensive and unclear area of similar focal cortical alteration is visible also contralaterally (white arrowheads). In the subependymal region underneath the left frontal cortex abnormality, a nodule of heterotopic gray matter is clearly visible (black arrow). The septum pellucidum is absent.
Discussion
The main feature of the present report is the capability of prenatal MR imaging to help detect even minor focal cortical developmental alterations. The other interesting aspect is that the development of focal cortical anomalies can be assessed throughout different stages. In our case, the cortical focal anomaly progressed from an unclear irregular and wartlike appearance to an excessive increase in cortical gyri convolution and tightness. The wartlike and initial cortical infolding, which we noticed at 24 weeks’ gestation, resembles what has been described in experimentally induced microgyria in rats in which cortex is almost lissencephalic, similar to that at 24 weeks’ gestation in the normal human fetus (4).
The cortical focal abnormality we detected at birth can be identified as a form of focal polymicrogyria in which the typical excessive convolution and tightness of cortical gyri is less marked than that usually visible in older patients (ie, when myelination is complete). It is likely that such focal cortical alteration will progressively “mature,” resulting in the MR imaging appearance of typical focal cortical polymicrogyria after the 1st year of age. The presence in our case of a heterotopic subependymal nodule is consistent with the periventricular heterotopia often associated with cortical developmental anomalies in older patients (5). It is worth mentioning the the presence at 24 weeks’ gestation of a thin T2 hypointense line extending from the periventricular nodule toward thecortical abnormality. Although this finding was not striking, it underscores the diagnostic accuracy of prenatal MR imaging and also provides some clues that explain the pathophysiology of the developmental alterations we observed. The periventricular and cortical abnormalities are very likely the result of a combination of neuronal migration and cortical organization disorders (6), which involved the cortexcertainly unilaterally and, possibly, bilaterally before 20 weeks’ gestation. Our case presents some significant differences with respect to the one described by Inder et al (7); namely, a postnatal MR imaging follow-up study in an infant (born at 27 weeks’ gestational age) with polymicrogyria. The authors described a bilateral perisilvian polymicrogyria, which was associated with periventricular leukomalacia and appeared as a minor unclear abnormality at 31 weeks’ postconceptional age at MR imaging; its classic appearance was reached at the corrected age of 3 months. They referred to the polymicrogirya as a pure postmigrational disorder because of the simultaneous postnatal onset with the periventricular leukomalacia. In our case, the presence of periventricular heterotopia strongly suggests that a neuronal migration alteration coexisted with a postmigrational disorder. The postmigrational cortical-organization disorder sustained the changing MR imaging features of the focal cortical abnormality, which “matured” along with the normal cortical gyration process.
Two main histologic forms of polymicrogyria have been described: a layered one, which contains four cellular layers and is likely to be the result of postmigrational events (8), and an unlayered one, which contains radially distributed neurons with no horizontal organization and is frequently associated with periventricular neuronal heterotopia (9). The latter form is believed to be caused by events occurring before the end of the neuroblast migration process (10). We hypothesize that, in our case, both histologic forms of polymicrogyria may coexist, because both the neuronal heterotopia and the progression of the cortical abnormality were present. The coexistence of both unlayered and layered polymicrogyria within the same subject has been already shown by pathology reports (11, 12).
The absence of septum pellucidum is one of the key features of the septo-optic dysplasia syndrome; however, septo-optic dysplasia is a clinically and radiologically heterogeneous syndrome (13). In our case, septo-optic dysplasia cannot be excluded, although it is unlikely, at least in its classic form, because of the normal appearance of optic nerves and chiasm and because of the absence of the typical boxlike shape of the frontal horns. The absence of septum pellucidum has been demonstrated to be highly correlated with the presence (3, 14) of bilateral or unilateral schizencephalic-polymicrogyric clefts, specifically confined within the frontal lobe. A segmental developmental alteration involving both the interhemispheric structures and the neocortex has been hypothesized to explain the topographic correlation between the absence of septum pellucidum and the cortical defects within the frontal lobe (especially in the posterior part). The patients carrying such alterations are usually affected by major neurodevelopmental deficits and by a major epileptic syndrome. The case herein is probably a mild form (without schizencephaly) within the spectrum of such major congenital malformations.
Conclusion
The clinical impact and usefulness of the early prenatal MR imaging diagnosis of a nonextensive (minor) cortical malformation is still not clear. Cortical malformations may or may not be associated with severe neurologic symptoms, depending on the location and extension of the cortical defects (15) and the presence of associated brain malformations. In our case, the neonate, taking into account the limited clinical follow-up, did not show neurologic deficits and was free from seizures. More prenatal MR imaging cases with longer postnatal follow-up need to be collected to provide prognostic data to clinicians and parents about similar conditions.
References
- Received March 10, 2003.
- Accepted after revision April 29, 2003.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Automatic Quantification of Normal Brain Gyrification Patterns and Changes in Fetuses with Polymicrogyria and Lissencephaly Based on MRI
- Hindbrain Herniation in Chiari II Malformation on Fetal and Postnatal MRI
- Diagnostic Value of Prenatal MR Imaging in the Detection of Brain Malformations in Fetuses before the 26th Week of Gestational Age
- Evaluation of Subependymal Gray Matter Heterotopias on Fetal MRI
- What Does Magnetic Resonance Imaging Add to the Prenatal Sonographic Diagnosis of Ventriculomegaly?
- Prenatal Diagnosis of Polymicrogyria by Fetal Magnetic Resonance Imaging in Monochorionic Cotwin Death