
Abstract
BACKGROUND AND PURPOSE: Blood flow of the internal jugular vein and intracranial venous sinuses is affected by respiratory state. The purpose of this study was to clarify the changes in flow velocity and direction and signal intensities of sigmoid sinuses on phase-contrast (PC) MR images obtained with regular breathing and with deep inspiratory breath holding.
METHODS: One hundred seven subjects without venous sinus abnormality were studied. Coronal 2D PC MR venography and axial 2D PC images with peripheral pulse gating were acquired with a 1.5-T MR unit, during regular breathing and deep inspiratory breath holding. The signal intensity changes of bilateral sigmoid sinuses on MR venograms and the changes of flow velocity and direction on the axial 2D PC images were analyzed.
RESULTS: Breath holding decreased signal intensities of the right and left sigmoid sinuses on MR venograms in 57 (53.3%) and 36 (33.6%) subjects, respectively. Increased signal intensity was observed in 12 (11.2%) and 33 (30.8%) subjects, respectively. In the flow analysis, retrograde flow was detected at the left sigmoid sinus in four subjects (3.7%) during regular breathing, which was normalized by breath holding. Flow velocities of the right and left sigmoid sinuses decreased during breath holding in 92 (86.0%) and 70 (65.4%) subjects, and increased in 15 (14.0%) and 37 (34.6%) subjects, respectively.
CONCLUSION: The signal intensities of sigmoid sinuses were affected by breath holding in about 2/3 of the subjects. Breath-holding maneuver can be used to increase blood flow and signal intensities of dural venous sinuses on PC MR venograms.
The intracranial venous system can be evaluated with several modalities, including angiography, CT venography (1, 2), and MR venography (3–6). In contrast to the other modalities, MR venography, which uses the time-of-flight or phase-contrast (PC) sequence, is noninvasive because it does not need injection of contrast material (5). Although angiography is the most reliable method to evaluate the intracranial venous systems, MR venography has also been used frequently because of its rapidity and noninvasiveness (7, 8).
Several pitfalls of MR venography have been reported. Ayanzen et al (4) described “flow gaps” in transverse sinus, which appeared as small defects on time-of-flight MR venograms. PC MR venography has been recommended over the time-of-flight sequence because inplane, slow, or turbulent flow mimics thrombosis on time-of-flight MR venograms (9, 10).
Another pitfall of MR venography is the breathing state, which affects the sinus blood flow. The blood flow of dural venous sinuses can be affected by breathing maneuvers, especially in supine position. Mehta et al (11) reported that deep inspiratory breath holding and deep expiratory breath holding resulted in a decrease in sinus blood flow. However, the data were based on the average flow in 15 volunteers, and the change of sinus flow in each individual was not presented. Hemostasis of the left internal jugular vein on tidal ventilation, which can be relieved by full inspiration, was reported by Tanaka et al (12). The cause of hemostasis is suspected to be compression of the left brachiocephalic vein between the aortic arch and the sternum. Because full inspiration increases the distance between the aortic arch and the sternum, it relieves hemostasis of the left internal jugular vein. As these flow changes of the dural sinuses induced by breathing maneuver can affect signal intensities on MR venograms, it can be a potential pitfall in diagnosing sinus thrombosis.
The purpose of this study was to clarify the changes in dural sinus signal intensity and flow direction and velocity between regular breathing and deep inspiratory breath holding, by using PC MR imaging.
Methods
Subjects
This study included 109 consecutive patients with lacunar infarction who underwent brain MR imaging for the purpose of routine follow-up, during a 3-month period (December 2001 to February 2002). Among them, two patients were excluded because MR imaging with peripheral pulse gating could not be performed owing to severe arrhythmia. A total of 107 subjects were eligible for this study. The population consisted of 52 men and 55 women (mean age, 56.1 years; range, 13–83 years). All patients were confirmed to have no history of craniotomy or sinus abnormality.
This study protocol was approved by the institutional review board, and informed consent was obtained from all patients.
Imaging Protocol
All MR examinations were performed with a 1.5-T superconducting MR system. Nontriggered 2D PC MR venography and peripheral pulse–triggered 2D PC MR images were obtained. Both image sets were acquired during regular breathing and deep inspiratory breath holding, during which the respiratory state was monitored by using a respiratory gating belt.
Single-section, nontriggered 2D PC MR venography was performed in the coronal plane with the following parameters: 20/8.4/3 (TR/TE/excitations); flip angle, 20°; velocity encoding, 20 cm/s (bipolar gradients were applied in the three orthogonal directions); field of view, 22 cm; section thickness, 10 cm; matrix, 128 × 256; acquisition time, 23 seconds. The plane of imaging was set in the posterior fossa and included the transverse and sigmoid sinuses. Magnitude images were reconstructed for visual assessment.
Peripheral pulse–triggered 2D PC imaging was performed in the axial plane by using the following parameters: gated/4.2/1; flip angle, 30°; velocity encoding, 30 cm/s (bipolar gradients were applied in the three orthogonal directions); field of view, 36 cm; section thickness, 6 mm; matrix, 128 × 256. The number of phases resolved and total acquisition time varied from 7 to 23 phases (average, 12.9 phases) and approximately from 18 to 28 seconds, respectively, depending on the heart rate. Imaging plane was placed at the level of the sigmoid sinuses. Magnitude and velocity images were reconstructed for the purpose of quantitative flow analysis.
Image Evaluation and Data Analysis
Coronal 2D PC MR venograms were evaluated by three neuroradiologists (K.K., S.T., T.A.). Both regular-breathing and breath-holding images of each patient were displayed simultaneously on the CRT of the image display terminal, in a randomized fashion. Each reader independently evaluated the change in signal intensity of the sigmoid sinuses before and after breath holding as follows: no change, higher in regular breathing, or higher in breath holding. The readers were blinded about the breathing status for an image set. Interobserver agreement was quantified by using κ statistics (13). A κ value of more than 0.8 indicates almost perfect agreement; 0.6–0.8, substantial; 0.4–0.6, moderate; 0.2–0.4, fair; and 0.0–0.2, slight agreement. When inconsistency occurred, the results of signal intensity evaluation were made on the findings of more than two readers.
Flow directions and velocities of both sigmoid sinuses were determined by measuring signal intensities of the sinuses with use of variable-sized regions of interest on peripheral pulse–gated 2D PC images. The regions of interest, which encompassed the entire vascular lumen, were drawn on the magnitude images by one observer (K.K.). The signal intensities on the velocity images during one cardiac phase were recorded and averaged. The changes in mean signal intensity and flow directions between the two breathing states (ie, before and after breath holding) were analyzed. Because of limitation in available imaging sequence and analyzing software, the absolute blood flow could not be calculated. Instead, the signal intensity on velocity images, which reflects relative flow velocity, was evaluated.
Comparison of average flow signal intensities during regular breathing and breath holding was made for all patients. Paired t test was used as the statistical test. Correlation between signal intensity change on MR venograms and velocity change on flow analysis was also analyzed, and in this case, the χ2 test was used to determine statistical significance. Statistically significant difference of each test was defined as a P value of less than .05.
Results
Signal Intensity on MR Venograms
The κ values of interobserver agreement in signal intensity evaluation on MR venograms ranged from 0.58 to 0.82 (Table 1). The average κ values among three readers for the right and left sigmoid sinuses were 0.67 and 0.71, respectively, indicating moderate agreement.
Kappa values for interobserver agreement between readers
Signal intensity changes of the sigmoid sinuses between regular breathing and breath holding on MR venograms are summarized in Table 2. On the right side, 57 patients (53.3%) showed lower signal intensity during breath holding than regular breathing, whereas 12 patients (11.2%) showed increased signal intensity on breath holding. There was no signal intensity change in 38 patients (35.5%). On the left side, 36 patients (33.6%) showed lower signal intensity during breath holding, and 33 patients (30.8%) showed higher signal intensity. Thirty-eight patients (35.5%) showed no signal intensity change.
Signal changes of the sigmoid sinuses on MR venography
One typical example of signal intensity change in MR venography is illustrated in Fig 1A and 1B. Breath-holding maneuver decreased the signal intensity of the right sigmoid sinus and increased the signal intensity on the left side. The change was consistent with flow analysis (Fig 1C).

Case of a 66-year-old woman.
A and B, Coronal 2D PC MR venograms obtained during regular breathing (A) and breath holding (B). The right sigmoid sinus is clearly depicted on the regular-breathing image. Signal intensity decreases with breath holding. The left transverse and sigmoid sinuses are not seen on the regular-breathing image. However, the signal intensities of these veins (arrows) are depicted on the breath-holding image.
C, Velocity image of the peripheral pulse–triggered 2D PC sequence shows the signal intensities of the sigmoid sinuses. The signal intensity of the right sigmoid sinus decreases during breath holding. However, increased signal intensity is observed in the left sigmoid sinus with breath holding, compared with regular breathing. These flow changes of the sinuses are consistent with the results on the MR venograms. ○ indicates the right sigmoid sinus (regular breathing); •, the right sigmoid sinus (breath holding); □, the left sigmoid sinus (regular breathing); ▪, the left sigmoid sinus (breath holding).
Flow Analysis
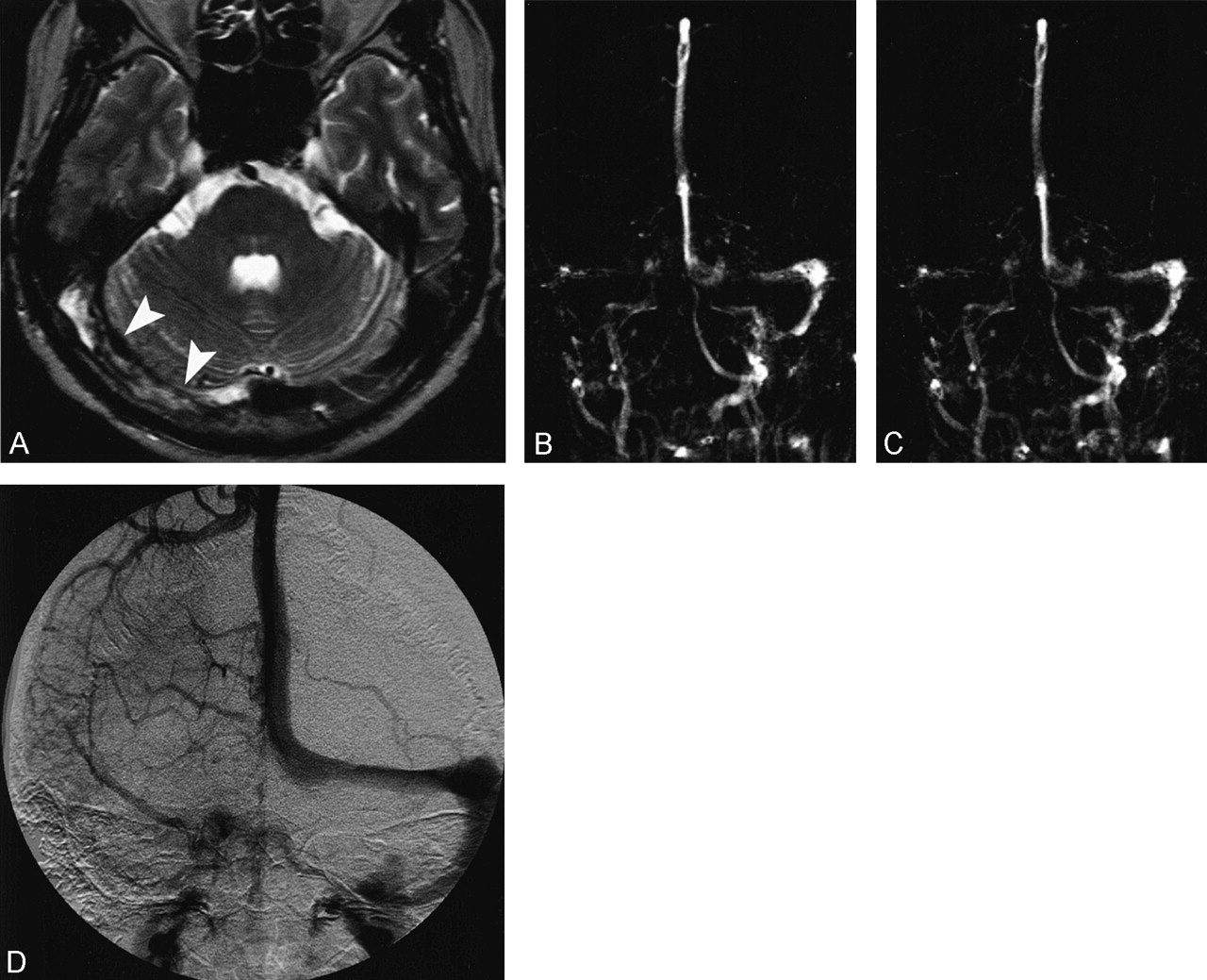
In all patients, normal antegrade flow was observed in the right sigmoid sinus during both regular breathing and breath holding (Table 3). Four patients (3.7%) showed retrograde flow in the left sigmoid sinus during regular breathing (Fig 2A-C). However, the retrograde flow normalized to antegrade flow during breath holding. Among these four patients, 3D time-of-flight MR angiography was conducted in two patients and allowed strong visualization of sigmoid sinus and internal jugular vein in one patient (Fig 2D).

Case of a 63-year-old man.
A and B, Coronal 2D PC MR venogram with regular breathing (A) and breathholding (B). Right transverse and sigmoid sinuses are seen on both regular-breathing and breath-holding images. The left sigmoid sinus is not visualized on regular-breathing image, but is seen on the breath-holding image (arrow).
C, Velocity image shows signal intensities of sigmoid sinuses. The signal intensity of the right sigmoid sinus decreases slightly during breath holding. The signal intensity of the left sigmoid sinus with regular breathing is below zero, which indicates retrograde flow. With breath holding, the retrograde flow is normalized, but the signal intensities are small, indicating slow flow. ○ indicates the right sigmoid sinus (regular breathing); •, the right sigmoid sinus (breath holding); ▪, the left sigmoid sinus (regular breathing); ▪, the left sigmoid sinus (breath holding).
D, Three-dimensional time-of-flight MR angiogram. The left internal jugular and sigmoid sinuses are seen on the maximum intensity projection image (arrow). Visualization of these veins can be explained by the in-flow effect of retrograde flow.
Flow direction of the sigmoid sinuses
Table 4 summarizes the flow velocity change determined by flow analysis. Flow velocity in the right sigmoid sinus was decreased by the breath-holding maneuver in 92 patients (86.0%) and increased in 15 patients (14.0%). Decreased flow was observed in the left sigmoid sinus in 70 patients (65.4%), and increased flow was noted in 37 patients (34.6%). Average flow of all patients is summarized in Fig 3. Breath holding significantly decreased the average sinus flow of all subjects in both sides.

Average flow signal intensity in all subjects. Breath holding decreases the sinus flow in both sides. * indicates statistically significant difference (P < .05). Bars indicate standard deviation; RB, regular breathing; BH, breath holding
Velocity change of the sigmoid sinuses
Tables 5 and 6 show correlation between the signal intensity change on MR venograms and the velocity change on flow analysis in the right and left sigmoid sinuses, respectively. Although there was some inconsistency, good correlations were observed for both sides. The χ2 test revealed statistical significance on both sides.
Correlation between signal change of MRV and velocity change of flow analysis (right sigmoid sinus)
Correlation between signal change of MRV and velocity change of flow analysis (left sigmoid sinus)
Discussion
Intracranial venous flow can be affected by respiratory state or breathing maneuvers. Decreased flow of bilateral transverse sinuses during deep inspiratory and expiratory breath holding has been reported by Mehta et al (11). As in the Valsalva maneuver, deep inspiratory breath holding induces positive intrathoracic pressure, which in turn causes a decrease in venous return of the body’s circulatory system, including intracranial venous sinuses. However, deep expiratory breath holding and the Müller maneuver can produce negative intrathoracic pressure, resulting in increased venous return. Possibly, however, venous return may decrease as the veins at the thoracic inlet collapse during this maneuver. Mehta et al reported only the average data of 15 subjects, and individual change of sinus blood flow affected by breathing maneuver was not presented.
In the present study, we found that the average flow of all subjects decreased during deep inspiratory breath holding, which is consistent with the previous report. However, upon analysis of blood flow in individual subjects, not only decreased flow, but also increased flow was observed (right, 14.0%; left, 34.6%). Increased flow induced by breath holding can be explained by the fact that physiologic venous stenosis at the thoracic inlet is relieved by deep inspiratory breath holding (Fig 4). Anatomically, the left brachiocephalic vein drains into the superior vena cava where it crosses the aortic arch. Therefore, the left brachiocephalic vein can be easily compressed between the sternum and aortic arch or right brachiocephalic artery, especially when the artery becomes ectatic due to aging or atherosclerosis. The compression is relieved by full inspiration, because the distance between the aorta and sternum increases. In contrast, the right brachiocephalic vein cannot be compressed by such mechanism, because it runs parallel to the ascending aorta. Our findings that the venous stasis and increased flow are observed more frequently on the left side are consistent with the previous report by Tanaka et al (12).

Diagram illustrates the physiologic venous stenosis at the thoracic inlet.
A, The left brachiocephalic vein (Bv) is compressed between the aortic arch (Ao) and the sternum (St) during regular breathing (arrowheads).
B, The compression is relieved by full inspiration (arrowheads), because the distance between the aorta and sternum increases due to the elevation of anterior chest wall (arrows). E indicates esophagus; Sv, superior vena cava; T, trachea; V, vertebra
Similarly, change in signal intensities of the sigmoid sinuses was noted on MR venograms during breath holding. Signal intensity decrease was noted in most of the subjects; this decrease was probably caused by an increase in intrathoracic pressure, a mechanism similar to the Valsalva maneuver. However, signal intensity increase of the right and left sigmoid sinuses was observed in 11.2% and 30.8% of the subjects, respectively. This phenomenon is also considered to result from the relief of venous stenosis at the thoracic inlet during deep inspiratory breath holding.
Although there were good correlations between signal intensity change on MR venograms and velocity change on flow analysis, some inconsistency was also observed. The inconsistency can be explained by the differences in imaging parameters, such as velocity encoding and gating, between the two sequences. Incomplete or inconstant breath-holding maneuver, which produces fluctuation of sinus flow, can be another cause of inconsistency. In this study, MR venography was performed in 23 seconds, which is considered to be short enough for breath holding in most patients. In contrast, duration of 2D PC MR imaging for flow analysis varied from 18 to 28 seconds. The imaging time depended on the heart rate, because peripheral pulse triggering was used. Despite monitoring the respiratory phase and repeating imaging if breath holding was incomplete, some patients could not complete legitimate breath holding during imaging, especially when the imaging time was long.
The intracranial venous system can be evaluated noninvasively with MR venography by using the PC sequence. Visualization of the veins depends on the blood flow when contrast material is not used. Thus, in performing MR venography in suspected cases of venous thrombosis, care should be taken that the signal intensity change can be induced by the breathing state. Defect in venous sinuses on regular breathing does not always mean venous thrombosis or hypoplasia, but can be improved by breath holding (Fig 5). Acquiring MR venograms during breath holding is a simple and quick method to reduce false-positive interpretations in patients suspected of having venous sinus thrombosis. In contrast, defect of the sinuses on MR venograms does not change under breath holding in true sinus thrombosis (Fig 6).

Venous stasis mimicking sinus thrombosis in a patient with systemic lupus erythematosus.
A, Axial fast fluid-attenuated inversion-recovery image (9000/110/2300/1 [TR/TE/TI/excitation]) shows high signal intensity in the left transverse sinus (arrowhead). Venous thrombosis is suspected.
B and C, Coronal 2D PC MR venograms. Although the left transverse and sigmoid sinuses are not visible on the regular-breathing image (B), these veins are clearly depicted on the breath-holding image (arrows in C). Venous occlusion is ruled out by MR venography with breath holding.
Case of a 53-year-old man with venous sinus thrombosis.
A, Axial fast spin-echo T2-weighted image (4500/106/2 [TR/TE/excitations]) shows inhomogeneous high and low signal intensity in the right transverse sinus (arrowheads).
B and C, Coronal 2D PC MR venograms show partial defect in the right transverse sinus and sigmoid sinus on the regular-breathing image (B). The right internal jugular vein is not seen. These defects do not change on the breath-holding image (C).
D, Anteroposterior venous phase image of right carotid angiography shows filling defect in the right transverse and sigmoid sinuses.
In addition to venous stasis, which is improved by breath holding, retrograde flow of the left sigmoid sinus was also observed in four subjects. Physiologic stenosis of the left brachiocephalic vein can be the cause of retrograde flow, as well as venous stasis described above. Two of the four subjects underwent MR angiography with the 3D time-of-flight sequence, and one subject showed prominent left sigmoid sinus. Ouanounou et al (14) reported that the cavernous sinus and inferior petrosal sinus were frequently depicted in healthy subjects with 3D time-of-flight MR angiography, and they suggested that it depends on technical factors concerned with the imaging sequences. Although the inferior petrosal sinus was not visualized in our subjects, it is possible that the retrograde flow of the left internal jugular vein and sigmoid sinus can cause retrograde flow of the inferior petrosal sinus. We speculate that visualization of the inferior petrosal sinus on MR angiograms, as well as the sigmoid sinus, is partly due to the retrograde flow caused by the thoracic inlet stenosis. A recent report demonstrated retrograde flow in the inferior petrosal sinus by using presaturation band (15).
There are several limitations in this study. The short imaging time for obtaining breath-holding images limited spatial resolution and number of acquisitions. Despite the poor signal-to-noise ratio, the images allowed evaluation of signal intensity change between regular breathing and breath holding. The imaging sequence and analyzing software for flow velocity analysis, which did not allow calculation of the absolute blood flow, were also limiting factors. As the purpose of this study was to compare the sinus flow between regular breathing and breath holding, the signal intensity on velocity images, which reflects the relative flow velocity, instead of the absolute blood flow, was evaluated.
In this study, venous stasis and retrograde flow were proved only in the sigmoid sinuses, but flow in the jugular vein or stenosis of the thoracic inlet were not evaluated directly. Measurement of the distance between aortic arch and sternum could be the direct proof to venous stasis. However, we speculate that it is caused by the physiologic stenosis of thoracic inlet veins, because the stasis and retrograde flow were normalized by deep inspiratory breath holding (12). The knowledge that visualization of the intracranial venous sinuses can be affected by breath holding could be helpful in evaluating venous sinuses with MR venography by using a PC sequence.
Conclusion
The breath-holding maneuver affected the signal intensity of the sigmoid sinuses on MR venograms in about 2/3 of the subjects. In addition to decreased signal intensity, increased signal intensity was also observed by breath holding. The breath-holding maneuver can be used to increase blood flow and signal intensities of dural venous sinuses on MR venograms by using the PC sequence. When a signal intensity defect of the venous sinus is seen on PC MR venograms during regular breathing, acquisition of additional images with breath holding may allow increase in signal intensity and reveal if it is a false sinus defect. MR venography during breath holding can be used to differentiate false sinus defect from true sinus thrombosis.
References
- Received June 17, 2003.
- Accepted after revision October 10, 2003.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Normal Flow Signal of the Pterygoid Plexus on 3T MRA in Patients without DAVF of the Cavernous Sinus
- Value of MR Venography for Detection of Internal Jugular Vein Anomalies in Multiple Sclerosis: A Pilot Longitudinal Study
- Sonographic Findings of Physiologic Left Brachiocephalic Vein Compression in a Case Initially Misdiagnosed as a Left Internal Jugular Vein Thrombus