
Abstract
Summary: An 11-month-old female patient presented with symptoms of orbital venous congestion. A CT scan showed enlarged superior ophthalmic vein and cavernous sinus on the symptomatic side. Catheter angiography confirmed a direct carotid-cavernous fistula with intra- and extracranial venous drainage. Successful coil embolization of the fistula was performed with resolution of the infant’s symptoms and return of previously elevated intraocular pressures to normal. To our knowledge, no cases of carotid cavernous fistulas in infancy have been previously reported.
Carotid cavernous fistulas can be spontaneous, secondary to trauma, or associated cavernous sinus pathology. Typically they are seen in adults and have been classified according to their hemodynamic properties (1, 2). They rarely occur in children with connective tissue disorders such as Ehlers-Danlos syndrome or after trauma (3–8). Spontaneous childhood fistulas are extremely unusual, the youngest reported patient being in a 5-year-old boy (9). We report a case of an 11-month-old female patient with a symptomatic direct carotid cavernous fistula without a preceding history of trauma or coexisting collagen vascular disorder.
Case Presentation
An 8-month-old white female patient with bilateral, congenital, nasal lacrimal duct obstruction was referred to our ophthalmology service for recurrent right epiphora after four probing and irrigation procedures and 2 weeks of right eye injection. Left epiphora had improved after one probe and irrigation procedure. The patient was otherwise healthy. There was no family history of inherited medical conditions.
Preoperative examination revealed a right increased tear lake with mattering of the right eyelids, consistent with nasal lacrimal duct obstruction. There were prominent conjuctival vessels in the right eye. Orbital examination, visual acuity, dilated fundus examination, and the rest of the ocular examination were normal.
The patient underwent repeat, right-probe irrigation balloon dilation with silicone tube placement. The procedure involves passing a probe through the eyelid puncta, canaliculus, lacrimal sac, and the lacrimal duct, which ends beneath the inferior turbinate. This passage is dilated with a balloon and intubated with a silicone tube, which is left in place. The posterior orbit is not involved in this procedure. Two days after the procedure, the parents noticed an increase in the dilated conjunctival vessels and new upper eyelid fullness that worsened over the following week.
Postoperative examination 3 weeks later revealed improved epiphora but increased, markedly dilated episcleral vessels in the right eye, with erythema, and fullness of the right eyelids. Right intraocular pressure was increased (22 mm Hg) compared with that of the left (11 mm Hg). There was slight right proptosis, which did not increase with inverting the child (Valsalva equivalent). The rest of the examination, including visual acuity and motility, was normal. There was no physical examination finding suggestive of connective tissue disorder.
Radiologic Findings
An initial nonenhanced CT scan showed an enlarged right superior ophthalmic vein and a prominent cavernous sinus on the symptomatic side suggestive of a cavernous sinus fistula.
Cerebral angiography confirmed a direct high flow carotid-cavernous fistula (Barrow type A; 1) in the right proximal cavernous internal carotid artery (Fig 1). There was no opacification of the supraclinoid internal carotid artery, because nearly all the blood was diverted into the cavernous sinus. Venous drainage was into an enlarged right superior ophthalmic vein and intracranially into cortical veins, internal cerebral veins, and the inferior petrosal sinus.
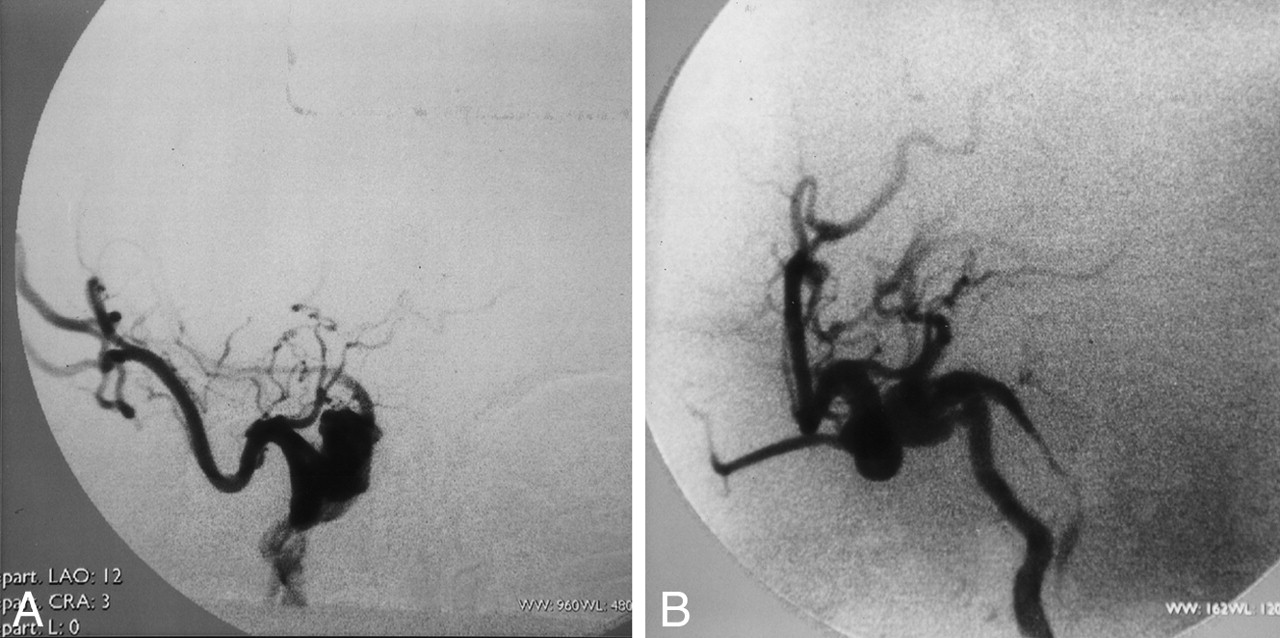
Anteroposterior (A) and lateral (B) internal carotid angiograms demonstrate the direct carotid-cavernous fistula with opacification of the cavernous sinus, the superior ophthalmic vein, and the inferior petrosal sinus. There is also early intracranial venous drainage.
Treatment
A decision to treat the fistula was made not only because of the risk to the infant’s vision, but also because of the significant intracranial venous drainage with its subsequent inherent risks of venous hypertension and its complications (hemorrhage, developmental delay) (10). The treatment options included occlusion of the fistula as the first choice, with carotid sacrifice, either endovascular or surgical, as an alternative if direct embolization could not be achieved. Endovascular embolization of the fistula was performed from a transarterial approach by means of detachable coils.
Postembolization angiograms showed complete occlusion of the fistula with a normal caliber and contour of the cavernous internal carotid artery segment (Fig 2). Furthermore, normal flow through the supraclinoid internal carotid, anterior, and middle cerebral arteries had been restored.

Postembolization internal carotid anteroposterior (A) and lateral (B) angiograms show complete occlusion of the fistula and restoration of blood flow to the supraclinoid internal carotid artery and the middle and anterior cerebral arteries.
Outcome and Follow-up
Immediately after coil placement, the intraocular pressure returned to normal (11 mm Hg). The patient was observed in the pediatric intensive care unit overnight without complication. The next day, the intraocular pressure remained normal and the proptosis, eyelid fullness, and dilated conjunctival vessels were improved. Two weeks later, ocular examination remained stable, except for a new right abduction deficit and 15-prism diopter esotropia, from a right sixth-nerve palsy. The patient was treated with a prism and continued follow-up in our ophthalmology department. Genetic evaluation for recessive or sporadic familial connective tissue disorder is in progress.
Discussion
To the best of our knowledge, this is the first reported case of a spontaneous direct, high-flow carotid cavernous fistula in infancy. Although the types, manifestations, and treatment options of carotid-cavernous fistulas have been extensively discussed in the current literature, most of this knowledge is based on an older population. Furthermore, younger patients often have associated connective tissue disorders, and childhood fistulas rarely occur after trauma (3–8). Although the patient had surgery, it is highly unlikely that this caused a traumatic fistula, because the anatomic location is remote, tissue manipulation was minimal, and her conjuctival vessels were dilated before the procedure. These fistulas can often present to the ophthalmologist with eyelid fullness, proptosis, dilated episcleral vessels, chemosis, bruit, increased intraocular pressure, and decreased visual acuity. Initially, these signs may be subtle, and early suspicion by the eye care provider is paramount.
The types, manifestations, and treatment options of carotid-cavernous fistulas have been extensively discussed in the current literature. This case is extremely unusual in the age group in which it presented. In fact, this is the first reported case of a direct, high-flow carotid cavernous fistula in infancy.
Initial imaging often consists of a CT scan. An asymmetrically enlarged cavernous sinus or superior ophthalmic vein is suggestive of a carotid-cavernous fistula and should prompt a call to the referring physician for further clinical information. Digital subtraction angiography is essential in confirming the diagnosis and delineating exact venous drainage patterns. This is performed under general anesthesia, in centers comfortable with infant angiography, ideally with a pediatric anesthesiologist. In our experience, soft detachable coils rather than balloons allow a relatively more precise and controlled occlusion of the fistula. One should also be prepared ahead of time for carotid artery sacrifice if needed.
In summary, this case report discusses the presentation and treatment of mainly an adult disease in a previously unreported age group.
- Received July 23, 2003.
- Accepted after revision August 10, 2003.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.