
Abstract
Summary: Giant cell angiofibroma (GCA) is a benign pathologic entity that has recently been reported in the literature. Originally described in the orbit, extraorbital sites of disease have also been reported. Herein, we describe the clinical, imaging, and pathologic findings of a case of GCA of the orbit.
Giant cell angiofibroma (GCA) is a rare benign tumor that shows a predilection for the orbit and soft tissues of the head and neck. Imaging reveals a highly vascular, circumscribed soft-tissue mass that may simulate a malignant or aggressive process. Surgical excision is often curative, but the tumor may respond to radiation therapy if surgery is not an option. In this report, we present the salient clinical, imaging, and pathologic features of a case of GCA of the orbit in one patient.
Case Report
A 60-year-old male patient presented to his ophthalmologist with a 4–5-year history of pain and discomfort in the left orbit. He reported no change in visual acuity and no diplopia. His medical history was notable for retinal detachment and a scleral encirclement procedure of the left eye 10 years previously. On physical examination, he had marked left proptosis with limited lateral movement of that globe. His cranial nerve examination was otherwise unremarkable.
CT at the time of initial presentation revealed a 3-cm noncalcified, uniformly enhancing soft-tissue mass in the left upper quadrant of the left orbit with associated proptosis (Fig 1). The mass was largely extraconal, without evidence of optic nerve involvement and did not erode or invade adjacent osseous structures. With a presumptive diagnosis of orbital hemangioma, an orbitotomy and attempted resection were performed. During surgery, the tumor bled profusely, and hemostasis was difficult to achieve. The tumor was also felt to be unresectable because of possible intraconal extension with involvement of the optic nerve. A biopsy was not obtained. Therefore, a lateral orbital wall decompression was performed, and the procedure was terminated.
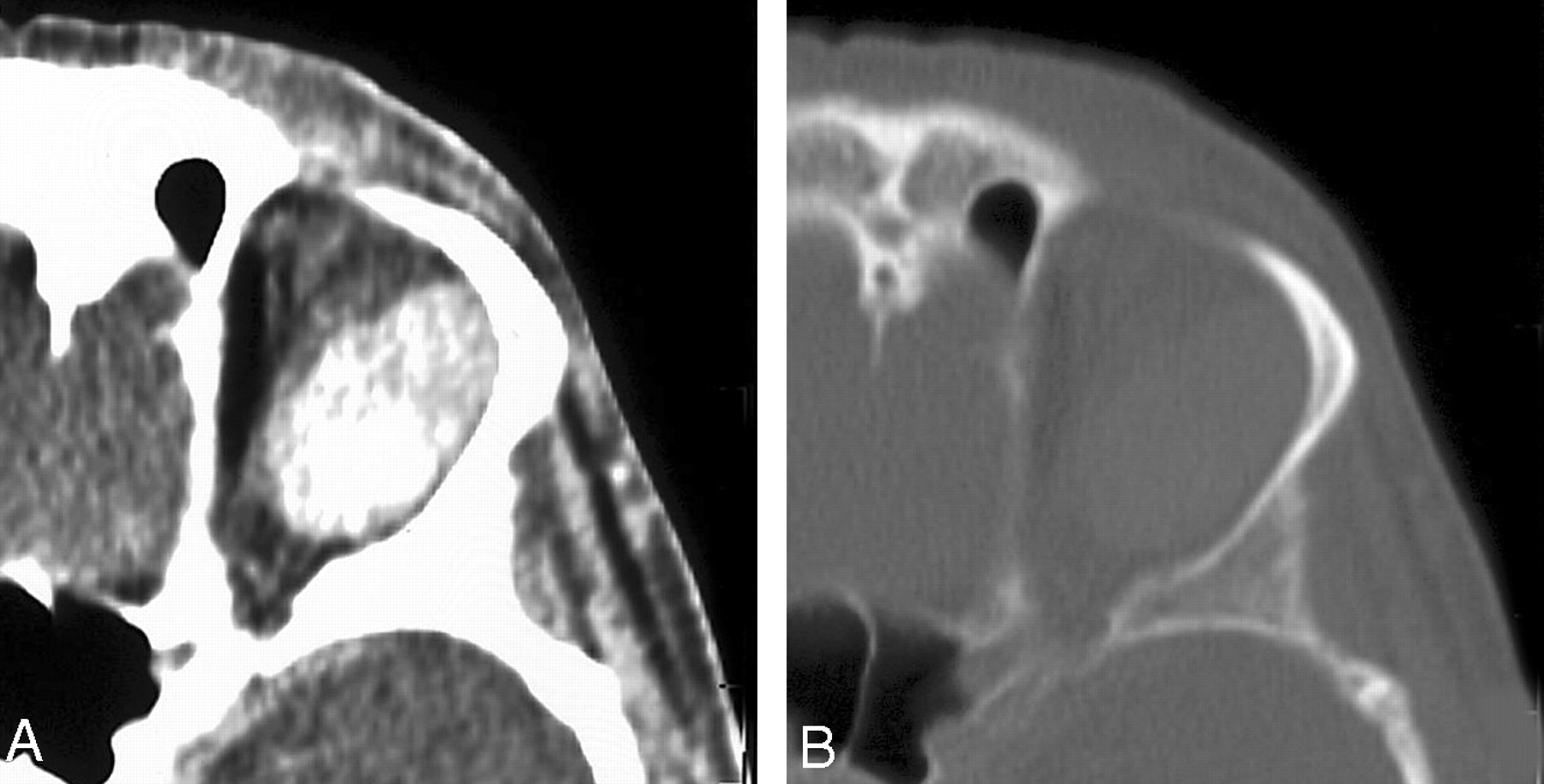
Axial contrast-enhanced (A) and bone window (B) CT images through the left orbit demonstrate a circumscribed extraconal soft tissue mass. The mass shows intense contrast enhancement and no internal calcification. There is no involvement of adjacent osseous structures or intracranial extension.
Approximately 9 months later, because of persisting symptoms, the patient underwent another partial resection of the tumor. Difficulty with hemostasis was again encountered, but this time a large portion of tumor mass was resected and sent for tissue diagnosis. Gross pathologic examination revealed a firm, tan-brown specimen. Histologic analysis demonstrated a proliferation of spindle cells in a fibrous stroma. Multinucleated giant cells were found as were multiple pseudovascular spaces. Mitotic activity was inconspicuous. A diagnosis of GCA was rendered on the basis of these findings.
Follow-up MR imaging to assess tumor status was performed 9 months after this partial resection (Fig 2). This demonstrated interval growth of the residual tumor, which measured 5 cm. The mass was homogeneously enhancing and located in the superolateral aspect of the left orbit. The mass showed both extra- and intraconal involvement and abutted the optic nerve. There was medial displacement of the optic nerve and proptosis. There was no intracranial extension. Multiple small signal intensity voids were noted within the lesion. No restriction of diffusion was noted on diffusion-weighted imaging.

Axial T2-weighted (3782/102/1 [TR/TE/NEX]) (A) and coronal pre- (B) and postcontrast (C) T1-weighted (510/14/1) images through the left orbit demonstrating the GCA as a well-circumscribed, homogeneously enhancing soft tissue mass with proptosis and posterior compression of the globe. The mass abuts and medially displaces the optic nerve. Stippled signal intensity voids are present in the precontrast images.
Because of persisting symptoms due to incomplete tumor resection, the patient underwent a course of external beam radiation therapy to the orbit. This provided marked symptomatic relief and diminished proptosis. Immediate postradiation follow-up MR imaging demonstrated a slight reduction in the size of the tumor, which remained closely applied to the optic nerve. Since that time, the tumor has remained stable in size without further intervention. The patient has been followed up for 5 years after initial presentation and is currently well with tumor.
Discussion
GCA is a benign neoplasm that was first described in 1995 in a study of seven patients with a distinctive orbital tumor (1). Since that time, approximately 39 cases have been reported in the literature, including our patient. Sixteen of these tumors have involved the orbit and periorbital soft tissues. For lesions occurring in the orbit, involvement of the globe has not been reported.
Extraorbital sites of disease include the nasolacrimal duct, buccal mucosa, submandibular region, trunk, mediastinum, retroperitoneum, vulva, and extremities (2–8). Tumor size ranges from 1.2 to 11 cm, with a mean size of 4 cm. GCAs may grow rapidly and simulate an aggressive or malignant process. They may also have an indolent course, growing slowly or remaining stable in size over many years. There is one report of two synchronous lesions arising from the buccal mucosa of one patient (9).
The age of patients with GCA ranges from 18 to 81 years, with a mean age of 48 years. This entity has not been reported in children. No sex predisposition has been noted.
Patients typically present with a solitary painless soft tissue mass. Other symptoms depend on the site of the tumor, are secondary to local mass effect, and include pain, visual disturbances, and respiratory difficulty (1, 4). One lesion occurring in the inguinal region clinically mimicked a hernia (10).
For lesions amenable to resection, surgical excision is the treatment of choice. Two instances of local postoperative recurrences have been reported (1, 2). As shown in our patient, radiation therapy may reduce tumor size or retard its growth when surgical resection could result in loss of function or is not possible.
Histologically, GCA is characterized as an intermediate tumor between a solitary fibroma and a giant cell fibroblastoma (1, 11, 12). They are well circumscribed and contain pseudovascularized spaces in a stromal matrix of patternless spindle cells with sparse multinucleate giant cells (6, 12, 13). GCAs are invariably positive for immunohistochemical staining with vimentin and CD34 (1–3,5, 6, 11, 13). GCAs have not been reported to be invasive, nor has any evidence for metastasis been documented, to date (2, 11). They are histologically distinct from nasopharyngeal angiofibromas, which contain highly cellular fibrous tissue composed of fibroblasts and myofibroblasts and do not contain giant cells (13). Cytogenetic testing in one study has revealed an associated chromosomal abnormality on 6q (14).
The imaging characteristics of our case corroborate the histologic features of this tumor. MR imaging shows the tumor to be well marginated. Stippled signal intensity voids seen on our patient’s MR images likely correspond to the many pseudovascular spaces seen in this highly vascular tumor, which also shows intense contrast enhancement. No bony erosion has been reported, and none was seen in our case.
The traditional radiologic differential diagnosis for a highly vascular orbital lesion includes hemangioma, lymphangioma, and metastasis. Because GCA can mimic both aggressive and indolent processes, it may be included in this differential diagnosis as well. Clinicians should be alerted to this possibility, because attempts at resection may be complicated by difficulty with hemostasis.
Conclusion
GCA is a benign tumor with a predilection for the orbit and head and neck regions in adults. Diagnostic imaging can play a role in determining tumor resectability, assessing surgical risks, and evaluating for tumor recurrence. In our case, its imaging appearance was compatible with a highly vascular soft tissue mass of the orbit, demonstrating flow voids and intense enhancement. GCA is uncommon but should be included in the differential diagnosis when an orbital mass has findings such as those here described.
References
- Received October 2, 2003.
- Accepted after revision November 22, 2003.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.