
Abstract
Summary: We present a canine lingual artery bifurcation aneurysm and assess its value for training in endovascular techniques and testing new embolic agents. The experimental aneurysm described herein mirrors human bifurcation aneurysms, and with this model, we sought to reproduce endovascular technical difficulties. However, the lesions created in this canine model did not show angiographic or histologic evidence of aneurysmal recurrence. We conclude that this model may be useful for training in endovascular techniques, but because of the lack of sufficient aneurysmal recurrence, it is not suitable for evaluating new embolic agents.
Coil embolization of ruptured intracranial aneurysms leads to a better clinical outcome than does surgery (1), although the outcomes of this endovascular approach are less definitive than those of surgical clipping owing to a higher incidence of angiographically proved aneurysmal recurrences (2). New techniques or materials designed to improve long-term results of endovascular treatment must be evaluated in experimental models that reproduce the problem of recurrence before they can be proposed for a clinical application (3–10).
A lingual artery aneurysm model was designed to mimic clinical aneurysms, and its potential value as a training tool and its capacity to lead to recurrences with a sufficient frequency to be useful in the evaluation of new techniques or embolic agents were assessed.
Methods
Protocols for animal experimentation were approved by the Institutional Animal Care Committee in accordance with guidelines of the Canadian Council on Animal Care. All surgical and endovascular procedures were performed with the animals under general anesthesia. Seventeen beagles weighing 10–15 kg were sedated with an intramuscular injection of acepromazine (0.1 mg/kg), glycopyrrolate (0.01 mg/kg), and butorphanol (0.1 mg/kg), and anesthetized with intravenous thiopental (15 mg/kg). The animals were ventilated artificially and maintained under surgical anesthesia with 2% isoflurane. Postoperative anesthesia was provided for 3 days by a 50-μg fentanyl skin patch. Bifurcation aneurysms were constructed by using venous pouches in 17 animals on the external carotid arteries, at the origin of the lingual arteries. In brief, the lingual external carotid bifurcation was accessed from bilateral 3-cm-long incisions in the submandibular region. Two segments from the same external jugular vein were harvested to be used as venous pouches. The lingual nerve was carefully dissected, encircled, and moved aside. The external carotid and lingual arteries were also encircled with ligatures, and blood flow was arrested with microvascular clamps. The bifurcation was stretched to form a straight line between lingual and distal external carotid arteries (Fig 1). The arteriotomy creating the neck of the aneurysm was eccentric, with two thirds of its length (8 mm) on the external carotid and one third on the origin of the lingual artery. Venous segments approximately 10 mm long were attached with two stay sutures, and the anastomosis was completed with 7-0 running suture. The fundus of the aneurysm was closed with hemostatic clips. Circulation was then restored (Fig 1).

Surgical construction of lingual bifurcation aneurysms. 1, Normal anatomy; 2, surgical technique; 3, final result. a, lingual artery; b, external carotid artery; c, lingual nerve; d, venous pouch; e, stay sutures; f, arteriotomy; g, running 7.0 Prolene suture; h, hemostatic clip.
The embolization procedure was performed at least 2 weeks after surgery. Six aneurysms in three animals were followed up for 3 months before embolization. Two other animals were also followed up for 6 and 9 months, respectively. Coil embolization (standard platinum coils in 11, radioactive coils in six, and Hydrocoils [MicroVention, Aliso Viejo, CA]) in two aneurysms) was done, as described elsewhere (9), to achieve complete or nearly complete aneurysmal sac obliteration. Polymeric coils (NeuroVasx; Maple Grove, MN) were used to embolize six aneurysms. Ethylene vinyl alcohol was injected under the protection of a balloon (HyperGlide; MicroTherapeutics, Irvine, CA). Other detachable coils were provided by MicroVention, MicroTherapeutics, Cordis Corporation (TRUFILL DCS; Miami Lakes, FL) and Boston Scientific/Target (GDC, GDC-Soft, Fremont, CA). Transfemoral conventional angiography was performed immediately after embolization, 3 weeks postoperatively, and 3 months postoperatively. Angiographic results were scored according to a previously described classification (10). A score of 0 indicated complete obliteration; 1, “dog ears”; 2, residual or recurrent neck; 3, residual or recurrent aneurysm; and 4, large saccular recurrences.
Macroscopic and microscopic stereophotographs were taken after excision of aneurysms. Neointimal formation and recanalization at the neck of bifurcation aneurysms were evaluated according to a previously described scoring system (3, 8): a score of 0 indicated complete neointimal sealing of the neck; 1, small areas of recanalization; 2, crescent of recanalization around the neointima covering the embolic agent; 3, recanalization affecting the coil mass; and 4, no neointima. Arteries and aneurysms were studied after formalin fixation, axial sectioning, and staining with hematoxylin-phloxine-saffron and Movat pentachrome.
The evolution of angiographic scores over time, following standard platinum coil embolization, was analyzed by using a Wilcoxon signed ranks test. A P value less than .05 was considered a significant difference.
Results
Most animals tolerated the surgical, embolic, and angiographic procedures without complications, except for one dog that died owing to an adverse reaction to anesthetic that immediately led to death after embolization. Of 32 constructed aneurysms that could be followed up, angiography showed 31 to be patent at 2-week follow-up. Six of six aneurysms followed up for 3 months were still patent, whereas two of two and two of two were also patent 6 and 9 months after surgery, respectively. Aneurysms tended to grow with time, as documented at 2-week and 3-month follow-up, but aneurysms followed up for 6 and 9 months were stable after the initial increase in size.
Catheterization of aneurysms was uncomplicated, and coil embolization could be performed in a fashion similar to that in clinical practice. It was often difficult to obtain complete obliteration of aneurysms without stenosing or occluding the origin of the lingual artery (Fig 2). When the origin of the lingual artery was stenosed at the time of embolization, it usually recovered a normal flow by 3 months (Fig 2).

Angiographic evolution after embolization. Carotid angiograms performed before 1), immediately after 2), and 3 months after 3) coil embolization of lingual bifurcation aneurysms, showing no recurrence.
The angiographic scores of lesions treated by coiling tended to remain stable and without recurrences. Some lesions improved with time, and one did recur at 3 months.
Mean size of aneurysms, mean packing density, and median angiographic and neointimal scores of lesions treated by standard coiling are summarized in the Table. There was no significant difference in the angiographic scores at 3 months as compared with initial scores (P=.713).
Angiographic and neointimal scores of lingual aneurysms treated with platinum coils
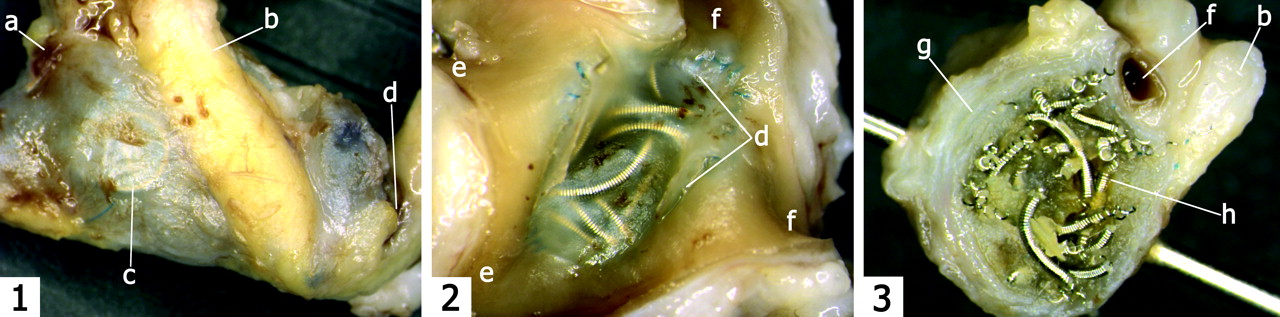
Macroscopic photography of the neck of aneurysms showed a well-defined neointima in most lesions (median neointimal score, 2; Fig 3). The neointimal tissue that formed at the surface of the embolic agents had nonspecific histopathologic features.
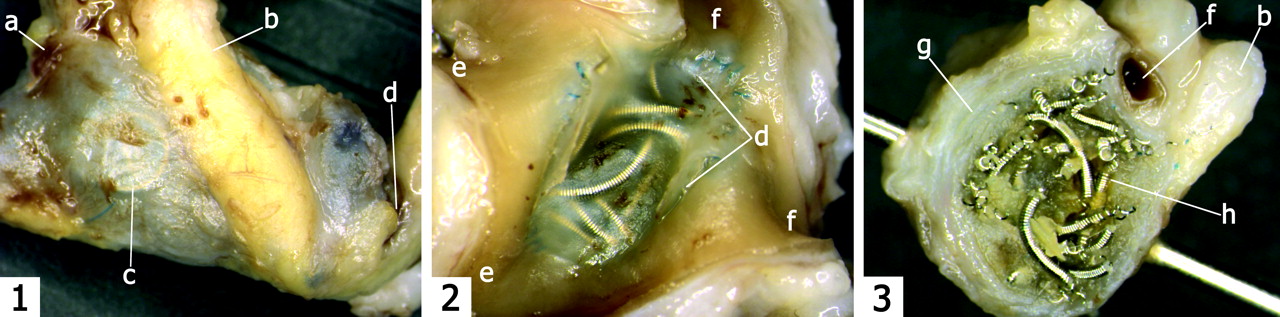
Macroscopic photography of aneurysms 3 months after embolization. 1, Side view; 2, view of the neck; 3, transverse section through the aneurysm. a, fundus; b, lingual nerve; c, coil inside the aneurysm; d, neck; e, carotid artery; f, lingual artery; g, aneurysm wall; h, coils.
Discussion
Animal models are essential to the preclinical evaluation of embolic material and devices. The surgical construction of venous-pouch aneurysms provides a reliable method to obtain aneurysms of homogeneous characteristics, such as consistent size and neck diameters. They remain patent for extended periods, provided they are created in the appropriate species, particularly in dogs and rabbits. Porcine models have a strong tendency for thrombosis and exuberant neointimal formation and have therefore been extensively used to study restenosis after stent implantation. However, because of the spontaneous healing of porcine aneurysms, they are inappropriate to assess results after embolization (4, 10–12). They may be used for acute experiments, although they are still incapable of assuring the safety of embolic materials (4). The advantages of surgical models are obtained at the cost of decreased biological pertinence due to surgical trauma, the artificial neck, the presence of suture material, and the venous composition of the aneurysmal wall, all factors that may influence tissue reactions after treatment. The claim that elastase models, another method to create experimental aneurysms artificially, provide lesions that are more similar to the human condition is a plausible hypothesis that has not been scientifically validated (11). The technique introduces its own artifacts, the lesions are less consistent, and the animal size necessitates significant modifications of endovascular techniques. Surgical aneurysms cannot be used to study the biology of aneurysm development and rupture, but recanalization and recurrences can be reproduced (3–10). We have elsewhere described an intraoperative sponge embolization model in canine lateral wall aneurysms with a tendency to recur (10). Coil embolization of canine carotid lateral wall aneurysms, however, is not followed by frequent recurrences (9). Bifurcation aneurysms have a stronger propensity for recurrence after coil embolization, especially when a wide-neck model is used (3, 8, 9). The bifurcation is a surgical anastomosis between the two carotid arteries. The aneurysms, parent vessel, and branches are large, and the model permits the construction of only one bifurcation aneurysm (3, 8, 9).
The lingual artery aneurysm model provides bilateral bifurcation aneurysms that mimic clinical lesions (Fig 2). The size of lesions and arterial branches mirrors that in the clinical setting. Evaluation of some coil characteristics, such as the rigidity and length of the junction between the coil and the pusher wire that may cause microcatheter kickback, could be performed with confidence. Attempts at complete occlusion of the lesion while preserving the origin of the lingual artery led to the same technical difficulties encountered in clinical procedures, including occlusion of the lingual artery, not protected by balloon inflation, with liquid embolic material. One anatomic feature of aneurysms constructed in this location is the close topographic relationship with the lingual nerve, which could be used to assess the safety or potential radiation damage to cranial nerves when using a radioactive coil strategy (6; Figs 1 and 3).
Angiographic results 3 months after coil embolization did not show sufficient recurrences for this model to be useful in the assessment of the potential of new embolic agents in improving long-term results. The reasons for the decrease in the recurrence rate as compared with other bifurcation models may be hemodynamic, because the model is closer to a lateral wall construction. Lesion and neck sizes are also inferior, which significantly increases the incidence of clinical recurrences (2).
Conclusion
Lingual artery bifurcation aneurysms provide a realistic model to mimic clinical procedures and could be helpful to evaluate embolic agents or materials in the acute setting as well as for the training of operators in the use of new devices. Unfortunately, they do not recur with sufficient frequency to assess the potential of new interventions in improving long-term results of endovascular treatment.
Footnotes
Supported by grants from Canadian Institutes of Health Research, and Hearth and the Stroke Foundation of Canada
References
- Received January 8, 2004.
- Accepted after revision March 7, 2004.
- Copyright © American Society of Neuroradiology
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Flow diversion of bifurcation aneurysms is more effective when the jailed branch is occluded: an experimental study in a novel canine model
- Creation of sidewall aneurysm in rabbits: aneurysm patency and growth follow-up
- Testing Flow Diverters in Giant Fusiform Aneurysms: A New Experimental Model Can Show Leaks Responsible for Failures
- Creation of Large Elastase-Induced Aneurysms: Presurgical Arterial Remodeling Using Arteriovenous Fistulas
- Five-Year Follow-Up in Elastase-Induced Aneurysms in Rabbits
- A New Canine Carotid Artery Bifurcation Aneurysm Model for the Evaluation of Neurovascular Devices
- Safety and Effectiveness of Radioactive Coil Embolization of Aneurysms: Effects of Radiation on Recanalization, Clot Organization, Neointima Formation, and Surrounding Nerves in Experimental Models