
Abstract
Summary: Intraoral neurilemmoma is rare (only 1%), and the most common form is a unilobular tumor on the dorsum of the tongue in the patients in the 2nd and 3rd decades of life. Herein we describe the case of intraoral neurilemmoma in a 9-year-old girl complaining only of a sore throat. She had an exophytic multilobulated mass on the base of the tongue. MR imaging demonstrates the extension of the tumor and helps in the differential diagnosis. The signal intensity of the tumor is similar to that of neurilemmomas in the other sites.
Neurilemmoma is a common tumor in the head and neck region (1). However, reports of the radiographic findings of tongue-base tumors are scarce in the literature. This report describes a case of pedunculated neurilemmoma arising from the base of the tongue.
Case Report
A 9-year-old girl complained of a sore throat, and her father found a mass in the oral cavity. She came to the department of otorhinolaryngology at our institution. She did not have any dysphagia or upper airway obstruction. Physical examination revealed a 2-cm pedunculated multilobular mass associated with dilated vessels on the tumor surface. It was located on the midline of the base of the tongue; tongue motion was still present (Fig 1). Necrotic and minor bleeding foci were observed on the surface of the white-coated mass. Her medical history was noncontributory. There was no lymph node enlargement in the neck. Results of routine laboratory tests were within normal limits.

Macroscopic view of the tumor. A pedunculated mass is noted in the midline to the right side on the base of tongue.
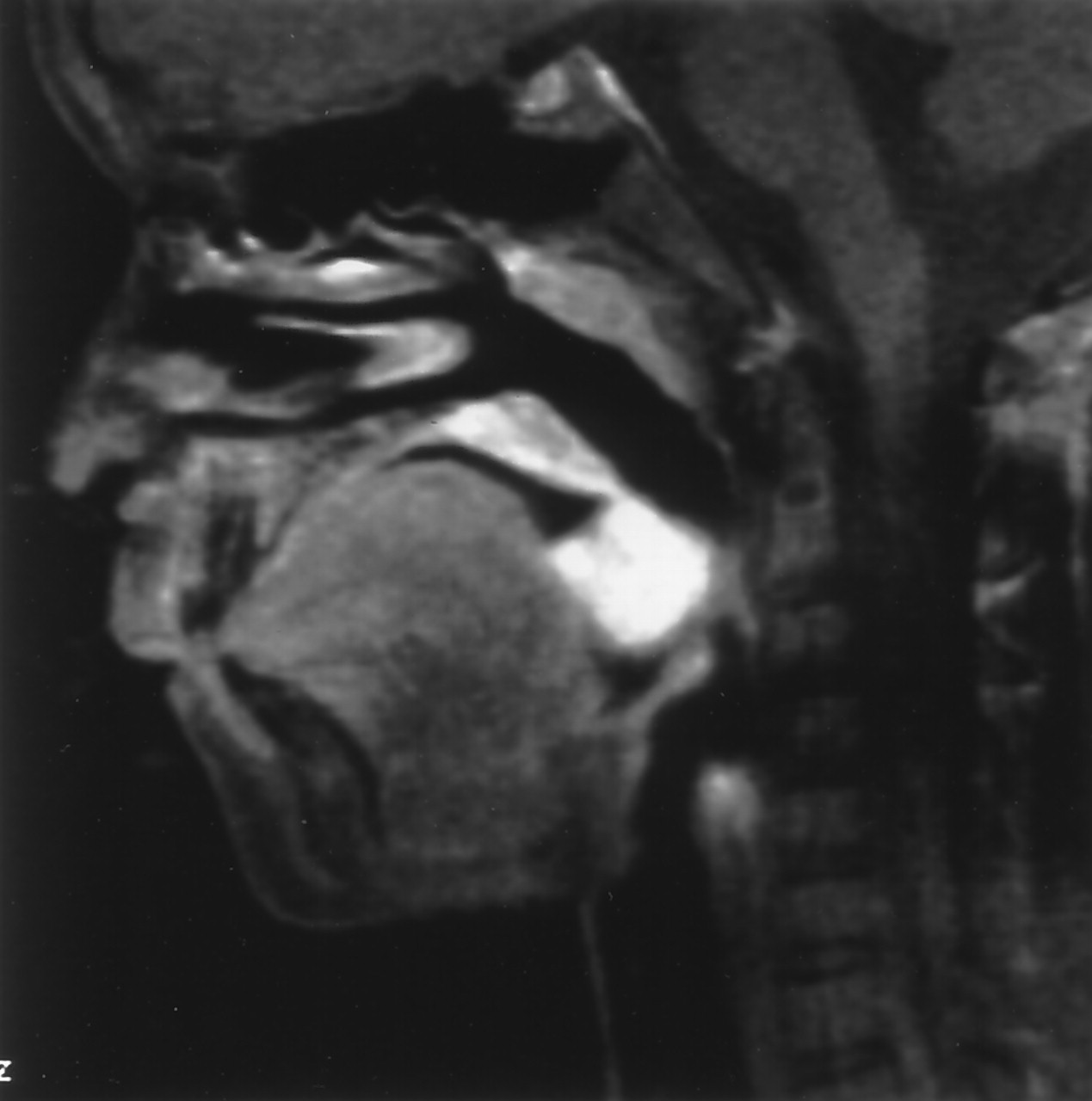
Contrast-enhanced CT showed a round soft-tissue mass on the base of the tongue. No calcification was noted (Fig 2). MR imaging demonstrated a mass with uniform isointensity relative to surrounding muscles on T1-weighted images without contrast enhancement, and on T2-weighted images, the signal intensity was markedly high (Fig 3). After intravenous administration of gadolinium DTPA, the tumor was markedly enhanced (Fig 4). Arteriography demonstrated a hypervascular mass fed by the lingual artery, mainly of the affected side, without encased vessels. Rhabomyosarcoma or hemangioma was considered as the diagnosis on the basis of preoperative findings. An endoscopic biopsy was performed under local anesthesia, but tumor tissue was not obtained. Under general anesthesia, the tumor was extirpated via transoral approach. The tumor was completely excised.

Sagittal reconstruction CT image after contrast enhancement. The tumor shows prominent enhancement in the base of the tongue. No calcification is noted in the mass.
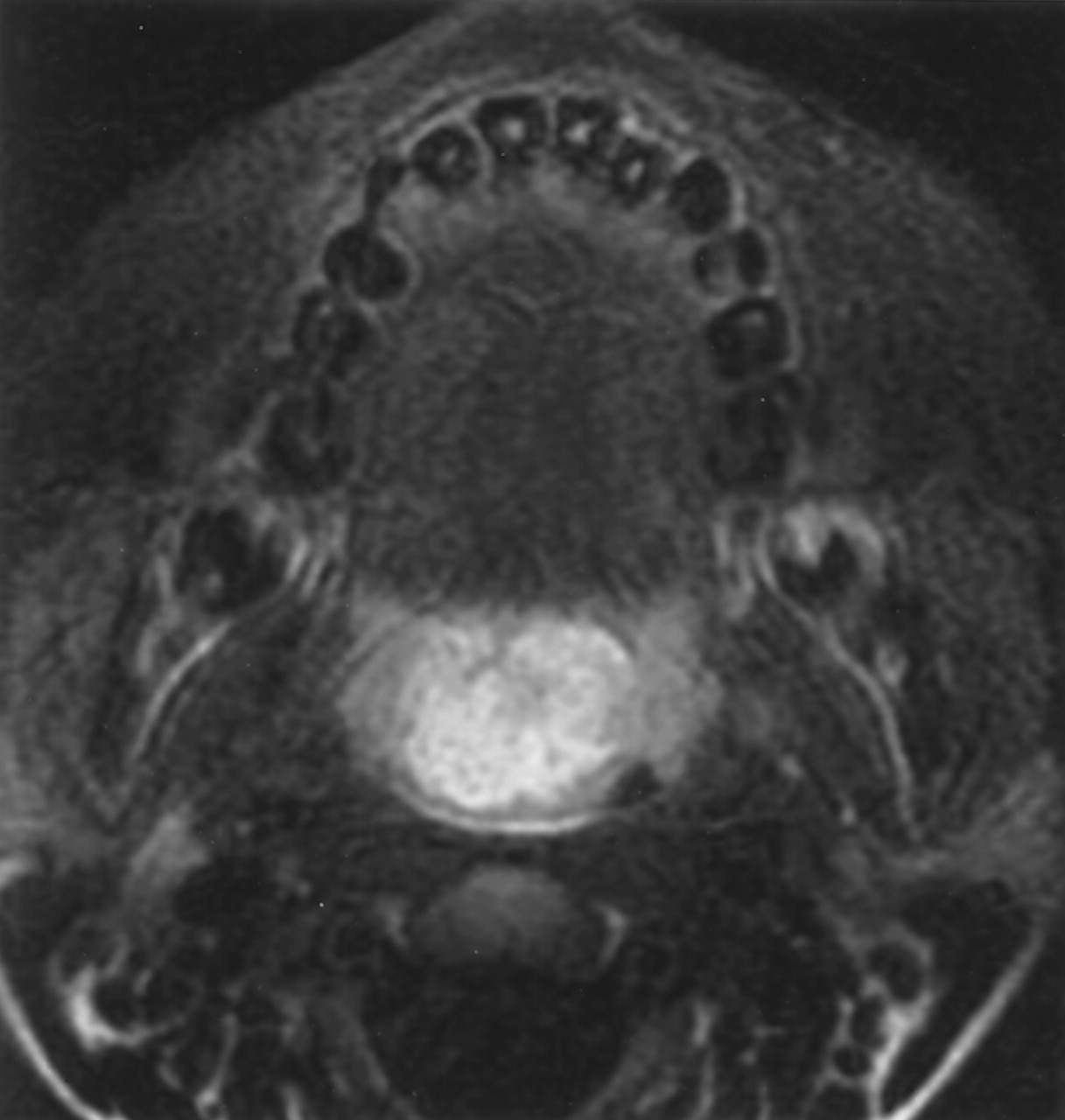
Axial T2-weighted MR image (fast spin-echo, TR/TE 3200/84) with fat suppression. The tumor has a high signal intensity with a well-defined margin.

Gadolinium-enhanced sagittal T1-weighted MR image (spin-echo, TR/TE 600/8.7) with fat suppression. Marked homogeneous enhancement is seen in the tumor.
The histologic examination revealed a well-encapsulated neurilemmoma of Antoni type A (Fig 5). An S-100 immunoperoxidase stain was positive. The nerve origin of the tumor was not determined. She had no recurrent tumor 17 months after the resection.

Histologic examination. Densely packed spindle cells join into compact bands running in different directions. Verocay bodies (arrows) are surrounded by cellular areas of palisading nuclei. (hematoxylin and eosin stain; original magnification ×20)
Discussion
The acoustic tumor is the most common intracranial neurilemmoma (Schwannoma or neurinoma) in the head and neck region. Of extracranial neurilemmomas, 25% are located in the head and neck region; however, intraoral neurilemmoma is rare (1%; 1). Neurilemmomas may occur at any age but are common between the ages of 20 and 50 years (2). Tumors in the oral cavity are often seen in the 2nd and 3rd decades of life, but are very rare in those aged 10 years or younger (3). There is no gender predilection. Recurrence is rare after complete resection. The tongue is a common site of neurilemmoma, followed by the buccal mucosa, the floor of the mouth, and the palate (3). The mobile portion, such as the dorsum, of the tongue is the most commonly affected site, but the base of the tongue is rare (3, 4, 5). Hatziotis et al (3) summarized 106 oral neurilemmomas seen between 1945 and 1964; only five cases among 59 cases of tongue neurilemmomas were located on the base or root of the tongue. In the recent reports (1, 3, 6–14), only two cases were on the base of the tongue (Table).
Summary of reported cases
The neurilemmoma is indistinguishable from other ecapsulated benign tumors on the basis of imaging findings, and therefore, definite diagnosis requires histologic examination. The histopathologic features are classified into two patterns: densely packed spindle cells with palisading arrangement (Verocay bodies) as Antoni A type, and loose hypocellular arrangement with hyalinized blood vessels and no definite architecture as Antni B type (15). Positive reactivity to S-100 protein and Leu-7 antigen supports the Schwann-cell nature of this tumor on immunohistochemistry (16, 17). The tumor presents with a smooth and demarcated mass without crossing the midline or invasion into the surrounding tissue (9). Mutilobular tumor growth is rare; instead, it is usually unilobular. Neoplastic proliferation of many Schwannoma cell lobules results in larger nodules, and such a growth pattern applies to the overactive tumors (8).
Differential diagnosis includes eosinophilic granuloma, rhabdomyoma or rhabdomyosarcoma, neurofibroma, hemangioma, lingual thyroid, epidermoid, dermoid cyst, and salivary gland tumors. Lingual thyroid, epidermoid and dermoid were excluded by the identification of normally located thyroid gland and no fatty signal intensity on MR images. Rhabdomyomas are extremely rare in the tongue and are most commonly encountered at the base of the tongue as ill-defined masses (18). Varied histologic changes of longstanding tumor associated with degenerative processes have been reported as ancient neurilemmomas (19).
Conclusion
Reports of MR imaging findings of tongue-base neurilemmoma are scarce in the literature (11, 12). In these reports, the tumor revealed a well-circumscribed, solid mass having homogeneous isointensity relative to the surrounding tissue on T1-weighted images and hyperintensity on T2-weighted images. Marked enhancement with gadolinium-DTPA is noted. Imaging features, including CT and MR imaging, are relatively nonspecific, but they can be included in the differential diagnosis on the basis of shape and location.
References
- Received February 3, 2004.
- Accepted after revision June 14, 2004.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}