
Article Figures & Data
Figures
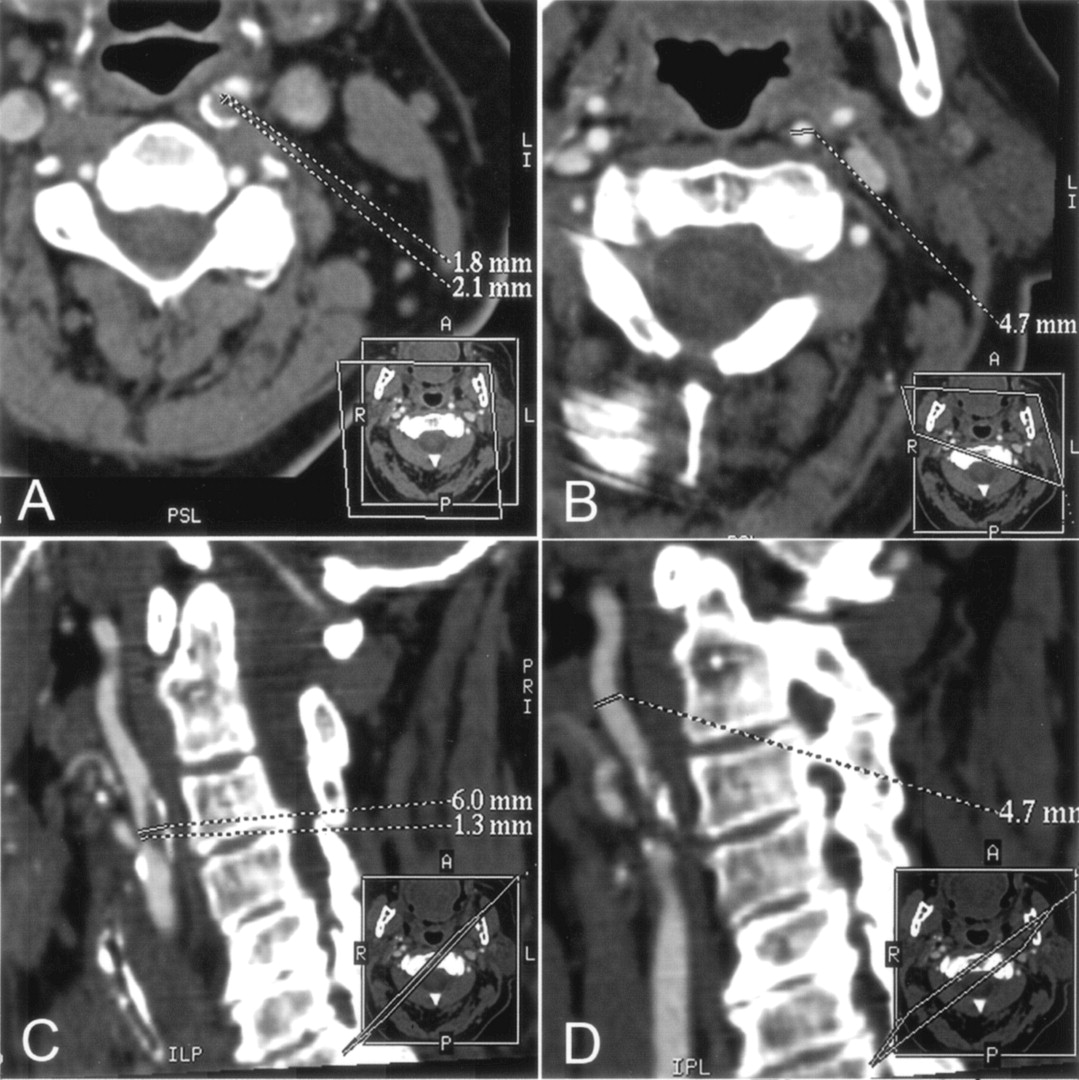
- Fig 1.
A–D, CT angiographic MPR images of the left ICA at the stenosis level (A and C) and at the distal extracranial ICA as the chosen reference level (B and D) for assessment of stenosis degree with NASCET criteria. Dotted lines indicate sites of measurement of vessel diameter. Every view was tilted according to the patient’s individual anatomy; the tilted planes are shown in small boxes in the right lower corner of each image.
A and B, Cross-sectional MPR images (data were reformatted with the double oblique mode) illustrate the accurate cross-section of the artery at the stenosis level (A) and at the chosen reference level (B). At the stenosis level, the minimum diameter was determined with an additional measurement perpendicular to the smallest diameter.
C and D, Oblique sagittal MPR images tilted along the course of the obliquely oriented ICA at the level of stenosis (C) and at the chosen reference level in the distal extracranial ICA (D) . At the stenosis level, the actual diameter of the entire ICA (upper dotted line in C), including the patent vessel lumen and the plaque, is shown.
- Fig 2.
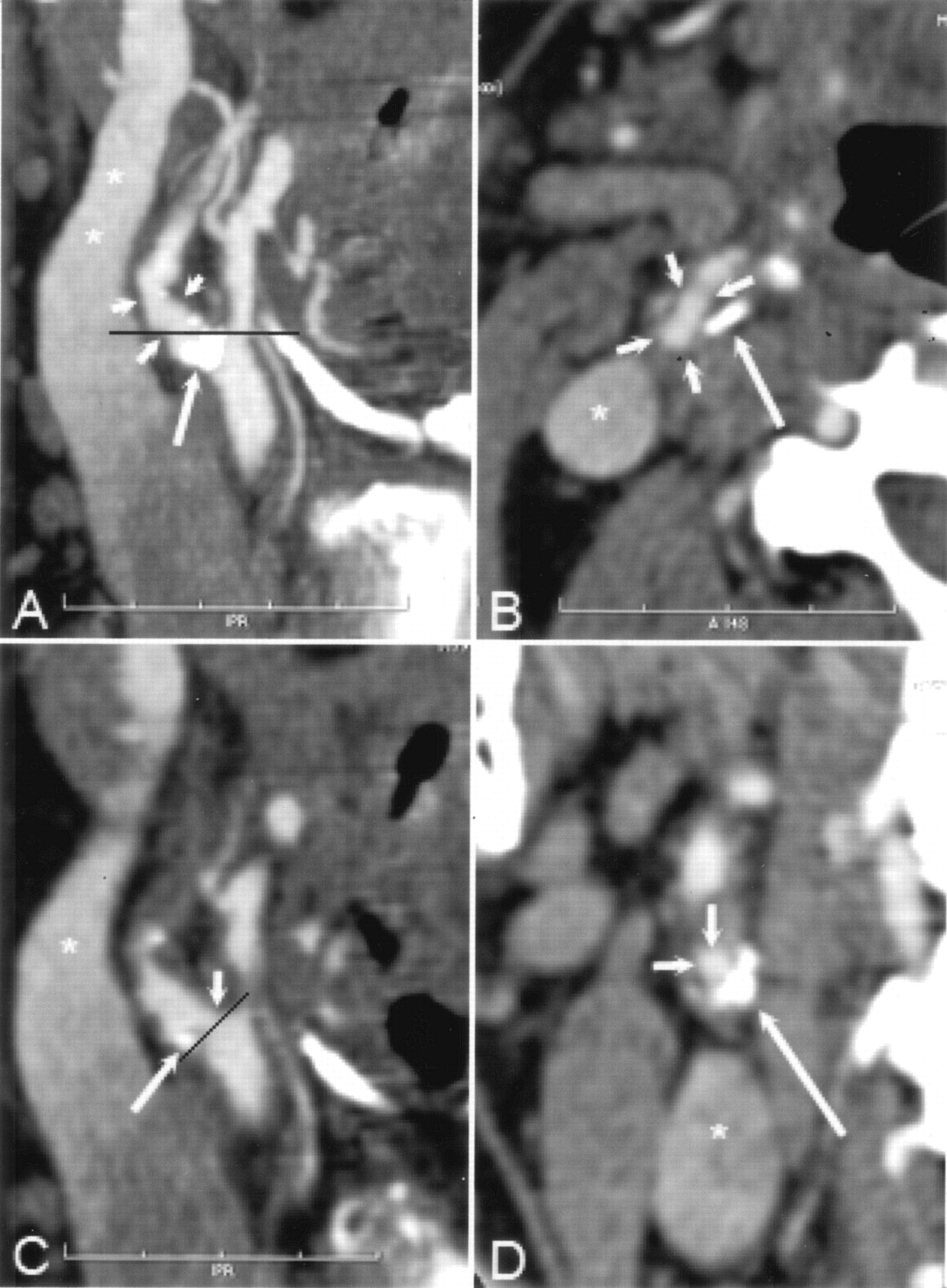
A and B, CT angiographic thin-slab MIP images with slab thickness of 6 mm in the right carotid artery reveals atherosclerotic changes (short arrows in A) and an extensive mural calcification (long arrow in A and B) in the bulbar area of the ICA. The black line in A indicates the corresponding axial plane in B. Note that the course of the ICA seen entirely on the MIP image deflects from the caudocranial scanning plane. Therefore, the cross-section of the ICA (short arrows in B) is elongated. Asterisk indicates partly enhanced jugular vein.
C, Oblique sagittal MPR image with section thickness of 0.3 mm shows that the hemodynamically insignificant stenosis (short arrow) is seen next to the mural calcification (long arrow), which hides the stenosis area seen on the MIP image in A. Black line indicates the orientation of the cross-sectional MPR image in D; asterisk indicates partly enhanced jugular vein.
D, Cross-sectional MRP image shows a concentric plaque in the ICA wall with eccentrically located extensive mural calcification (long arrow), and the enhanced lumen (short arrows) appears circular. Asterisk indicates partly enhanced jugular vein. According to our experience, it was slightly easier to determine the maximal stenosis point of the carotid artery with cross-sectional MPR than with sagittal MPR mode. With sagittal MPR mode, it is possible to rotate the image plane 360°, leading to inaccuracy in detecting the shortest diameter in eccentric stenoses. In addition, during the procedure to produce the MPR images at the GE workstation, there is a mark point on the target vessel (not shown) that sometimes hampers visualization of the stenosed carotid artery, especially with sagittal MPR mode.
- Fig 3.
Distal lesion in the petrous part of the left ICA detected correctly with CT angiography.
A and B, Axial (A) and coronal (B) MPR images of distal ICAs show the smaller diameter of the left ICA (long arrow) compared with the normal ICA on the right (short arrow).
C and D, Selective angiograms verify the stenosis (arrow in C) and a near-occlusion (arrow in D) at the bulb. This tandem lesion on the symptomatic side was successfully treated with angioplasty and stent placement.
- Fig 4.
A–D, Scatterplots show the distribution of absolute diameters in millimeters between rotational angiography and cross-sectional MRP (cMPR) (A) and oblique sagittal MPR (sMPR) (B) of CT angiography and between DSA and cross-sectional MPR (C) and oblique sagittal MPR (D) of CT angiography. The absolute diameter measurements were obtained from the stenosed level (filled square) and from the reference level (open circle).
- Fig 5.
A and B, Selective angiogram of the left carotid artery (A) shows a stenosis in the proximal ICA (arrow), which was measured to be 58%. Three-dimensional rotational angiogram of the same carotid artery (B), which was reconstructed from the 80 original projections, shows the stenosis (arrow) without overlapping arterial branches. Note that only the original projection images (not shown) instead of 3D reconstructions were used in the study as the reference for CT angiography. The stenosis degree was measured to be 69% on the original rotational angiograms (not shown).
C and D, CT angiographic cross-sectional (C) and oblique sagittal (D) MPR images show no mural calcification at the maximum stenosis (arrow). White lines on the carotid artery indicate the manually measured diameters of the vessels. Cross-sectional MPR image (C) shows the noncircularity of the lumen at the stenosed level. With CT angiographic measurements by the two radiologists, the stenosis degree was underestimated by 28–38% on the cross-sectional MPR images compared with rotational angiographic measurements. The underestimation rate was lower (2–18%) with use of oblique sagittal MPR images. In this particular case, the stenosis degree was visually estimated to be 70% with CT angiography
- Fig 6.
A, Right anterior oblique DSA image reveals high-grade stenosis (arrow) in the left ICA; degree of stenosis was calculated to be 82%. A high-grade stenosis is also present at the origin of the left external carotid artery.
B–D, CT angiograms verify the stenosis of the ICA (short arrow). Left sagittal view of 3D reconstruction MIP image (B) also shows stenosis of the external carotid artery. CT angiographic sagittal (C) and cross-sectional (D) MPR views reveal the stenosis in the ICA (short arrow) without over projection of mural calcification (long arrow). On the MIP image (B), mural calcification (long arrows) is over projected with the lumen. The degree of stenosis was considerably underestimated with CT angiography using the MPR measurements. However, the hemodynamic significance of the stenosis was obvious in the interactive interpretation of CT angiograms.
E and F, Rotational angiograms show that notable pulsation movement of the stenosed artery in the craniocaudal direction (arrow) can be detected when comparing the location of the stenosis to the upper endplate of the third cervical vertebra between these two images obtained in different phases of the cardiac cycle. The movement artifact might have caused extra blurring of the vessel wall on CT angiograms obtained without electrocardiographic gating.




Tables
DSA Rotational Angiography 0–29% 30–49% 50–69% 70–99% 100% 0–29% 10 1 11 30–49% 4 3 7 50–69% 1 4 5 70–99% 1 8 9 100% 1 1 10 6 8 8 1 33 Note.—Data are number of arteries in which both DSA and rotational angiography were performed.
- TABLE 2:
CT Angiographic MPR measurements of degree of stenosis compared with rotational angiographic measurements in 33 carotid arteries
MPR Method Observer Mean Difference* (% ± SD) r Value κ Value (95% CI) 50%† 70%‡ Cross-sectional 1 6.9 ± 17.6 0.82 0.58 (0.31–0.84) 0.40 (0.05–0.76) 2 10.7 ± 16.1 0.86 0.58 (0.33–0.83) 0.29 (−0.04–0.62) Sagittal 1 2.8 ± 19.2 0.80 0.70 (0.45–0.94) 0.40 (0.05–0.76) 2 9.1 ± 16.8 0.84 0.58 (0.31–0.84) 0.42 (0.06–0.76) * A positive mean difference value indicates an underestimation of stenosis degree with CT angiography.
† 50% cutoff point for hemodynamically significant stenosis.
‡ 70% cutoff point for hemodynamically significant stenosis.
- TABLE 3:
CT angiographic MPR measurements of degree of stenosis compared with DSA measurements in 70 carotid arteries
MPR Method Observer Mean Difference* (% ± SD) r Value κ Value (95% CI) 50%† 70%‡ Cross-sectional 1 −0.4 ± 23.0 0.76 0.53(0.33–0.73) 0.50(0.27–0.72) 2 5.3 ± 21.8 0.76 0.70(0.53–0.87) 0.36(0.14–0.58) Sagittal 1 −3.8 ± 24.5 0.73 0.55(0.36–0.74) 0.54(0.32–0.76) 2 3.7 ± 21.7 0.77 0.79(0.65–0.94) 0.38(0.15–0.61) * A positive mean difference value indicates an underestimation of stenosis degree with CT angiography.
† 50% cutoff point for significant stenosis.
‡ 70% cutoff point for significant stenosis.
- TABLE 4:
Diagnostic performance of various CT angiographic MPR analysis methods for assessment of degree of stenosis in carotid arteries compared with rotational angiography
MPR Analysis Method Observer Sensitivity (%) Specificity (%) Overall Accuracy (%) Cross-sectional 1 65 (11/17) 94 (15/16) 79 (26/33) 2 59 (10/17) 94 (15/16) 76 (25/33) Sagittal 1 82 (14/17) 88 (14/16) 85 (28/33) 2 65 (11/17) 94 (15/16) 79 (26/33) Combined* 1 82 (14/17) 88 (14/16) 85 (28/33) 2 71 (12/17) 88 (14/16) 79 (26/33) Note.—Numbers in parentheses are number of arteries. A 50% stenosis was the cutoff point for a hemodynamically significant finding.
* Combined MPR was considered to be positive when either of the MPR (cross-sectional or oblique sagittal) measurements yielded a positive result.
- TABLE 5:
Diagnostic performance of various CT angiographic MPR analysis methods for assessment of degree of stenosis in carotid arteries compared with DSA
MPR Analysis Method Observer Sensitivity (%) Specificity (%) Overall accuracy (%) Cross-sectional 1 73 (22/30) 80 (32/40) 77 (54/70) 2 77 (23/30) 98 (39/40) 88 (62/70) Sagittal 1 87 (26/30) 70 (28/40) 77 (54/70) 2 87 (26/30) 95 (38/40) 91 (65/70) Combined* 1 87 (26/30) 70 (28/40) 77 (54/70) 2 90 (27/30) 95 (38/40) 93 (66/70) Note.—Numbers in parentheses are numbers of arteries. A 50% stenosis was the cutoff point for a hemodynamically significant finding.
* Combined MPR was considered to be positive when either of the MPR (cross-sectional or oblique sagittal) measurements yielded a positive result.
- TABLE 6:
Diagnostic performance of CT angiography in the assessment of carotid artery stenosis on the symptomatic side compared with DSA
Analysis Method of CT Angiography Sensitivity (%) Specificity (%) Overall Accuracy (%) PPV (%) NPV (%) Visual 100 (21/21) 50 (7/14) 80 (28/35) 75 (21/28) 100 (7/7) Combined MPR* 95 (20/21) 86 (12/14) 91 (32/35) 91 (20/22) 92 (12/13) Visual-quantitative† 95 (20/21) 93 (13/14) 94 (33/35) 95 (20/21) 93 (13/14) Note.—PPV indicates positive predictive value; NPV, negative predictive value. Numbers in parentheses are number of arteries. A 50% stenosis was the cutoff point for a hemodynamically significant stenosis.
* Combined MPR was considered to be positive when either of the MPR (cross-sectional or oblique sagittal) measurements yielded a positive result.
† Visual-quantitative analysis consisted of first-line visual CT angiography interpretation and subsequent measurement only for the positive cases.
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Imaging Carotid Atherosclerosis Plaque Ulceration: Comparison of Advanced Imaging Modalities and Recent Developments
- Window Settings for the Study of Calcified Carotid Plaques with Multidetector CT Angiography
- Contrast-Enhanced MR Angiography Is Not More Accurate Than Unenhanced 2D Time-of-Flight MR Angiography for Determining >=70% Internal Carotid Artery Stenosis
- Superselective transcatheter arterial chemoembolisation of an unresectable hepatocellular carcinoma using three-dimensional rotational angiography