
Abstract
Summary: We describe a case demonstrating active extravasation of contrast material into a hematoma resection cavity during CT angiography (CTA) that necessitated emergent reexploration, decompression, and hemostatic control. Our case highlights the value of neuro-CTA in the immediate postoperative setting and describes another scenario where CTA has added value. Prompt recognition of contrast extravasation is critical to the diagnosis and ultimately affects the quality of patient care.
CT angiography (CTA) is a fast, minimally invasive, and inexpensive neurovascular imaging technique that is gaining in popularity because of its availability and spatial resolution. As a relatively new technique, its technical strengths (spatial resolution) and limitations (temporal resolution) are being assessed in a variety of clinical scenarios, including aneurysms, vascular malformations, steno-occlusive disease, vasospasm, and trauma (1–8). Active extravasation, which indicates active bleeding, has been described during neuro-CTA examinations including ruptured aneurysms, subdural hematomas, and spontanteous parenchymal hematomas and is generally regarded as a medical emergency. Recognition and accurate interpretation of active extravasation can help localize areas of active bleeding.
Case Description
A 22-year-old man was thrown from a motorcycle and suffered severe head and facial trauma. The patient’s Glasgow coma score at the scene was 3 and improved to 6 in the emergency department. A noncontrast CT (NCCT) examination demonstrated a large left frontal and basal ganglionic hematoma with subfalcine herniation and brain stem compression (Fig 1A). An emergency craniotomy was performed to decompress the hematoma and achieve hemostasis. After reattaching the bone flap, the patient deteriorated clinically. The bone flap was removed and emergent NCCT and neuro-CTA were performed to assess the resection cavity. The NCCT showed reaccumulation of the hematoma (Fig 1B). The source data set from the CTA demonstrated multiple foci of high attenuation fluid (contrast) within the reaccumulated hematoma, including anteroinferiorly where the lenticulostriates reside (Fig 2A and B). The contrast foci were nonanatomic and did not conform to a known vascular structure. In addition, the contrast layered dependently in a fluid-fluid pattern. The patient was returned to the operating room for reexploration. The hematoma was again evacuated and multiple small active bleeders were cauterized. Two actively bleeding lenticulostriates were observed anteroinferiorly: one was clipped, and the other was cauterized. These lenticulostriates corresponded to one of the areas of active extravasation. The patient survived the injury and was transferred to a rehabilitation facility.
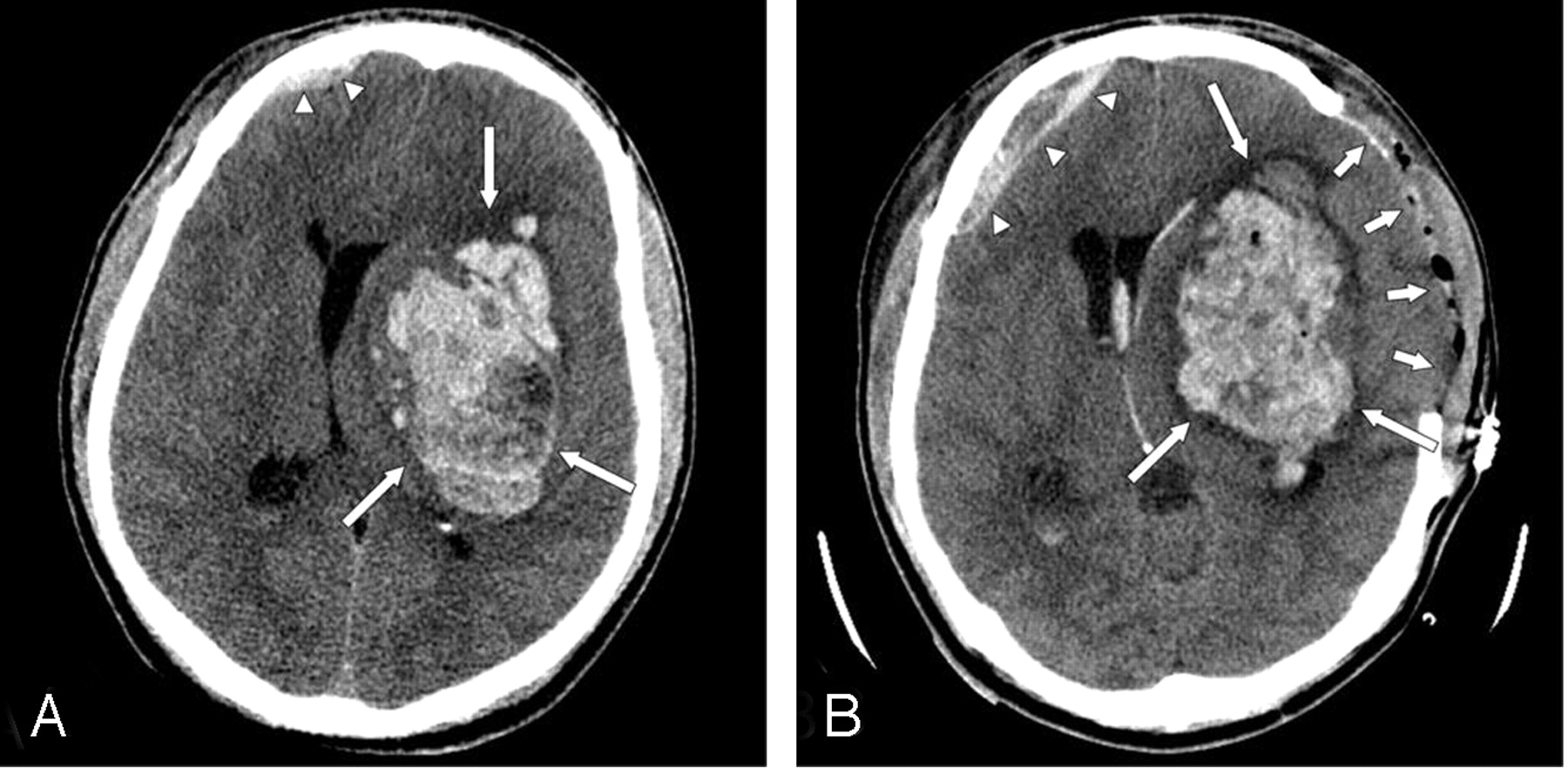
A, Axial CT scan at the level of the 3rd ventricle on admission showed a large left intrparenchymal hematoma (arrows) with vasogenic edema subflacine herniation. A small right frontal subdural hematoma is noted (arrowheads).
B, Axial CT scan at the level of the 3rd ventricle immediately after surgical decompression and subsequent clinical decline showed a left frontal craniectomy (short arrows), reaccumulation of the hematoma (long arrows), persistent subflacine herniation, and a slightly larger right frontal subdural (arrowheads).

A, Source axial CTA image at the level of the bodies of the lateral ventricles showed a layering fluid collection in the ventral aspect of the hematoma including a dependent hyperattenuated component dorsally (long arrow) and a nondependent hypoattenuated component ventrally (short arrow). The hyperattenuated component represented contrast whereas the non-dependent component likely represents plasma.
B, Sagittal multiplanar reformatted image of the CTA source data set showed multiple areas of “nonanatomic puddling” of contrast (circles) within the hematoma indicating active extravastion during the CTA examination.
Discussion
Traumatic intracranial lesions can be broadly characterized as primary or secondary lesions, depending upon their temporal relationship with the initial injury (9). Primary lesions are a direct result of the traumatic force and can be characterized as neuronal injuries, hemorrhages, vascular injuries, or pia-arachnoid injuries. Primary hemorrhages occur in multiple spaces including subdural, epidural, subarachnoid, intraventricular, and intraparenchymal. In the blunt trauma patient, intraparenchymal hematomas arise due to sudden acceleration-deceleration and rotational forces, which then result in the disruption of arteries and/or veins such as the lenticulostriates and are frequently identified in the frontotemporal white matter or deep gray nuclei (9). Dissections or tears of small vessels such as the lenticulostriates are rare and difficult to detect because of current spatial resolution limitations and practice patterns: traumatic intracranial parenchymal hemorrhages do not routinely undergo vascular imaging. Although direct visualization of a vascular injury to a lenticulostriate is beyond the spatial and temporal resolution of current noninvasive techniques (CTA, MR angiography), the secondary sign of “contrast extravasation” can be identified.
Prompt recognition of a vascular injury and active hemorrhage is crucial for optimal patient care. Detection of active extravasation has been widely reported on conventional angiography in the setting of acute nontraumatic intracranial hemorrhage (10, 11). There have been several case reports of active extravasation detected during neuro-CTA including aneurysms, subdural hemorrhage, and nontraumatic intracranial hemorrhage (12–15).
Gosselin and Vieco (12) described two cases of active hemorrhage from ruptured aneurysms demonstrated on CT angiography. In those cases, irregularity of the wall of the aneurysm, nonanatomic collection of contrast, and contrast opacification of the preexisting hematoma on the delayed scan were seen. The term “hematoma opacification sign” was used to describe opacification of a previously nonopacified hematoma adjacent to an aneurysm. They also stressed the nonanatomic appearance of such a collection as critical in the accurate assessment of this finding. The outcome was fatal in both cases. Nakada et al (13) described a ruptured anterior communicating artery aneurysm that reruptured during the initial diagnostic CTA with obvious contrast extravasation around the anterior communicating artery. The rerupture was fatal.
Kinoshita et al (14) described contrast extravasation into a subdural hematoma during a CTA and accurately located the bleeding cortical artery.
Murai et al (15) evaluated the usefulness of CTA to detect active extravasation in the setting of acute nontraumatic spontaneous intracranial hemorrhage. In 31 consecutive patients, five cases of active extravasation were detected, three of which showed hematoma enlargement. Of the 26 cases without extravasation, the hematomas remained stable on follow-up imaging. They concluded that 3D-CTA was valuable in the detection of persistent hemorrhage in the subset of patients studied.
In the current case, initial decompression was performed, followed by reaccumulation of the hematoma. CTA demonstrated multiple areas of contrast “puddling,” which represented active bleeding and prompted emergent reexploration. Some of the puddling was deep in the cavity in the expected location of the lenticulostriate vessels. The CTA identified areas of active bleeding and helped guide the neurosurgeon to areas of active bleeding and eventual hemostatic control.
As CT technology advances—including higher section profiles, longer detector configurations and increased computing power—the temporal and spatial resolution of CTA will improve. Although desirable in most situations, improved temporal resolution can be a source of error for the detection of active extravasation when the leak is slow instead of brisk. In this circumstance, extravasation may only be detected on a delayed CT scan after a neuro-CTA (B Dillon, personal communication). If an active hemorrhage is suspected, adding a delayed CT of the brain after neuro-CTA may help reduce false-negative examinations and improve specificity.
Conclusion
Identifying active extravasation of contrast during a neuro-CTA is critical for timely management and optimal patient care. The sine qua non of active extravasation into a hematoma is “nonanatomic puddling of contrast” and can be recognized on the source CTA data set. A delayed CT scan after neuro-CTA may help identify slower hemorrhages and improve specificity.
References
- Received July 28, 2004.
- Accepted after revision August 6, 2004.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}