
Abstract
BACKGROUND AND PURPOSE: Endovascular techniques are the methods of choice for the treatment of patients with carotid cavernous fistulas. We report our experience using stent-assisted coil placement for treatment of patients with high-flow fistulas that are associated with severe laceration of the internal carotid artery.
METHODS: In a retrospective review of an internal endovascular therapy database covering the interval between October 2001 and October 2003, we identified a total of 5 patients presenting with 6 high-flow type A carotid cavernous fistulas (one had a bilateral fistula) that were associated with severe laceration of the internal carotid artery. All were treated first with stenting of the injured segment of the internal carotid artery followed by transarterial (3/6) and/or transvenous (4/6) obliteration of the fistula with detachable platinum coils. In 2 cases, a liquid adhesive was also used. In all instances, a compliant balloon was inflated within the stented arterial segment during coil deposition to avoid extension of coils into the parent artery.
RESULTS: All 6 fistulas were obliterated, and each internal carotid artery was successfully reconstructed. Except for posttraumatic cranial nerve dysfunction in 1 patient, clinical outcome was very good. Follow-up angiograms in 3 of the 6 patients obtained at intervals between 3 and 6 months (mean, 4.5 months) revealed no fistula recurrence and no evidence of intimal hyperplasia within the stent.
CONCLUSION: In this series of patients with high-flow carotid cavernous fistula associated with severe injury to the internal carotid artery, stent-assisted coil placement offered a safe and effective treatment. Stent-assisted coil placement may increase the ability to successfully treat fistulas with severe injury to the internal carotid artery with preservation of the parent artery.
Most type A carotid cavernous fistulas are high flow and traumatic in origin (1). Type A carotid cavernous fistulas secondary to the rupture of an aneurysm of the cavernous segment of the internal carotid artery are much less common, accounting for no more than 20% of reported cases (2, 3). In our experience over the past 2 decades, most type A fistulas have a rather discrete laceration of the wall of the internal carotid artery and are readily repaired with either detachable balloons or coils inserted via either transarterial or transvenous approach. A minority, however, are associated with such severe laceration of the wall of the internal carotid artery that it is impossible to visualize, over a long segment, the course of the internal carotid artery. Because of the inability, in such circumstances, to be sure if a device (balloon or coil) used to close the fistula was either in or compromising the lumen of the internal carotid artery, trapping of the fistula with parent artery occlusion is often the safest treatment option.
Significant advances in stent and catheter design now make it possible in many instances to deploy either balloon-expandable or self-expanding stents designed for use in the coronary arteries in the cavernous and supraclinoid segments of the internal carotid artery. With these devices, it is possible to reconstruct a severely injured artery. Several recent case reports have described the use of stents in conjunctions with other embolic materials for the treatment of direct carotid cavernous fistulas. Lee et al (4) reported successful treatment of a patient with a traumatic aneurysm of the supraclinoid internal carotid artery and an associated carotid cavernous fistula with a balloon-expandable coronary stent and coils The same technique was used by Ahn et al and Men et al (5, 6) in the treatment of traumatic carotid cavernous fistulas. Redekop et al (7) reported 6 patients with traumatic vascular lesions of the skull base that were successfully treated using endovascular stents There have also been several case reports of patients with direct carotid cavernous fistulas as a result of iatrogenic internal carotid artery laceration associated with intracranial angioplasty (8–10) or after transsphenoidal surgery for pituitary adenoma (11–13) treated by stent placement. We present our experience treating 5 patients with 6 high-flow type A carotid cavernous fistulas associated with significant laceration of the internal carotid artery with stent-assisted coiling.
Methods
Patients
A search of an internal endovascular database during the interval between October 2001 and October 2003 revealed 5 patients with 6 type A carotid cavernous fistulas (one was bilateral) who were treated with stent-assisted coil placement. A retrospective review of all medical and imaging records of these patients was performed.
All patients presented with clinical signs or symptoms typical of high-flow type A carotid cavernous fistula, including exophthalmos (n = 4), chemosis (n = 2), cranial nerve deficits (n = 2), decrease in visual acuity (n = 2), headache (n = 2), and diplopia/ptosis (n = 1). Three patients were male and two were female. Their age ranged between 19 and 83 years (mean, 42 years). Four had a clear history of significant trauma (one had bilateral carotid cavernous fistula). One had no history of any trauma and was thought to have a rupture of an aneurysm of the cavernous segment of the internal carotid artery.
The most common location of the fistula was the cavernous segment (3/6), followed by 2 in the petrous–cavernous junction, and 1 in the petrous segment. There was severe laceration of the internal carotid artery in the 5 traumatic fistulas. This made it impossible to define the course of the internal carotid artery over a long segment. The single fistula thought to be due to rupture of a cavernous aneurysm also showed a very high-flow carotid cavernous fistula. The venous drainage involved variably all the tributaries to the cavernous sinus, most frequently (5/6) from the anterior region either from the superior ophthalmic vein and/or the inferior ophthalmic vein, also to the posterior and inferior regions including inferior petrosal sinus (2/6) and pterygopalatine plexus respectively, to the intracranial veins (2/6), and to the contralateral cavernous sinus in 1 case.
Treatment Technique
Endovascular treatment was carried out with patients under general anesthesia. Vascular access was achieved by placing 6- or 7-French sheaths into 1 or both common femoral arteries and, in instances in which transvenous coiling was performed, into one of the common femoral veins. Following placement of the access sheathes, we administered intravenous heparin sufficient to increase the baseline activated clotting time to 2.5- to 3.0-times baseline values. This level of anticoagulation was maintained until treatment was completed and was then reversed. All patients were given both aspirin and clopidogrel bisulfate (Plavix; Bristol-Myers Squib, New York, NY) for at least 24 hours before treatment. This regimen was then maintained for at least 6 weeks following treatment. At the end of the procedure, hemostasis at the access sites was achieved by using an AngioSeal (St. Jude Medical, Inc., Sylmar, CA).
Angiography was performed by using a biplane Axiom Artis BA with 3D capability (Siemens Medical Systems, AG, Malvern, PA). All patients underwent complete cerebral angiography. These acquisitions were used for analysis of the morphology of the carotid cavernous fistula as well as for measurement of vessel diameter to determine the appropriate stent size.
For stent placement, a 6- or 7-French Envoy guiding catheter (Cordis Corp., Miami, FL) was placed into the distal cervical segment of the ipsilateral internal carotid artery. Through this, a standard microcatheter (Excelsior, Boston Scientific, Natick, MA) was advanced over a 0.014-inch exchange guidewire across the injured segment of the internal carotid artery. The wire was manipulated by using road map and real-time fluoroscopic guidance until it was positioned in the visualized segment of the internal carotid artery above the level of the fistula. If a vertebral arteriogram or contralateral internal carotid artery arteriogram did not provide adequate visualization of the supraclinoid segment of the involved internal carotid artery, an injection through the microcatheter allowed visualization of the internal carotid artery above the fistula. Appropriate stent size was selected on the basis of these images. After removal of the microcatheter, we advanced a BX Sonic (n = 1) or a BX Velocity (n = 5) 4 × 18 mm stent (Cordis Corp., Miami, FL) and deployed it across the site of the fistula, using nominal pressures (10 atm) for deployment. In 4 of the carotid cavernous fistulas, coiling of the fistula was performed in the same session as stent placement. In 1 patient with bilateral carotid cavernous fistulas, bilateral stent placement of both internal carotid arteries was done 1 day followed by coiling of 1 fistula on the following day and the second fistula 5 days later. For coil deposition, a 4 × 20 mm HyperGlide balloon (Micro Theraupetics, Inc., Irvine, CA) was first placed inside the stent. Then, with the balloon uninflated, a microcatheter was introduced either alongside the balloon and through the stent into the cavernous sinus or from a venous approach into the cavernous sinus. Through this, a series of detachable platinum coils were introduced, positioned, and detached. During insertion and positioning of the coils, the balloon was inflated so that it prevented coils from coming through open cells of the stent and into the parent artery. A variety of coils from multiple vendors was used for coiling. Transarterial coiling was used as a sole method for coil deposition in 2 patients. In 1 patient, a combined transarterial and transvenous approach was used for coiling. Three other patients had coiling performed only from a transvenous approach. Venous access was achieved by catheterization of the inferior petrosal sinus in 3 patients and of the superior ophthalmic vein in 1 patient. In 2 patients, because of persistent flow after deposition of many coils, a small aliquot of N-butyl-2-cyanoacrylate (NBCA) mixed with Ethidol (Cordis Corp., Miami, FL) was injected as the last stage of treatment. During injection of the NBCA, we inflated the balloon in the internal carotid artery.
Follow-up angiography was performed in all patients before hospital discharge and in 3 patients at 3–6 months after treatment (mean, 4.5 months). Neurological assessment was also performed at these intervals (Figs 1 and 2).


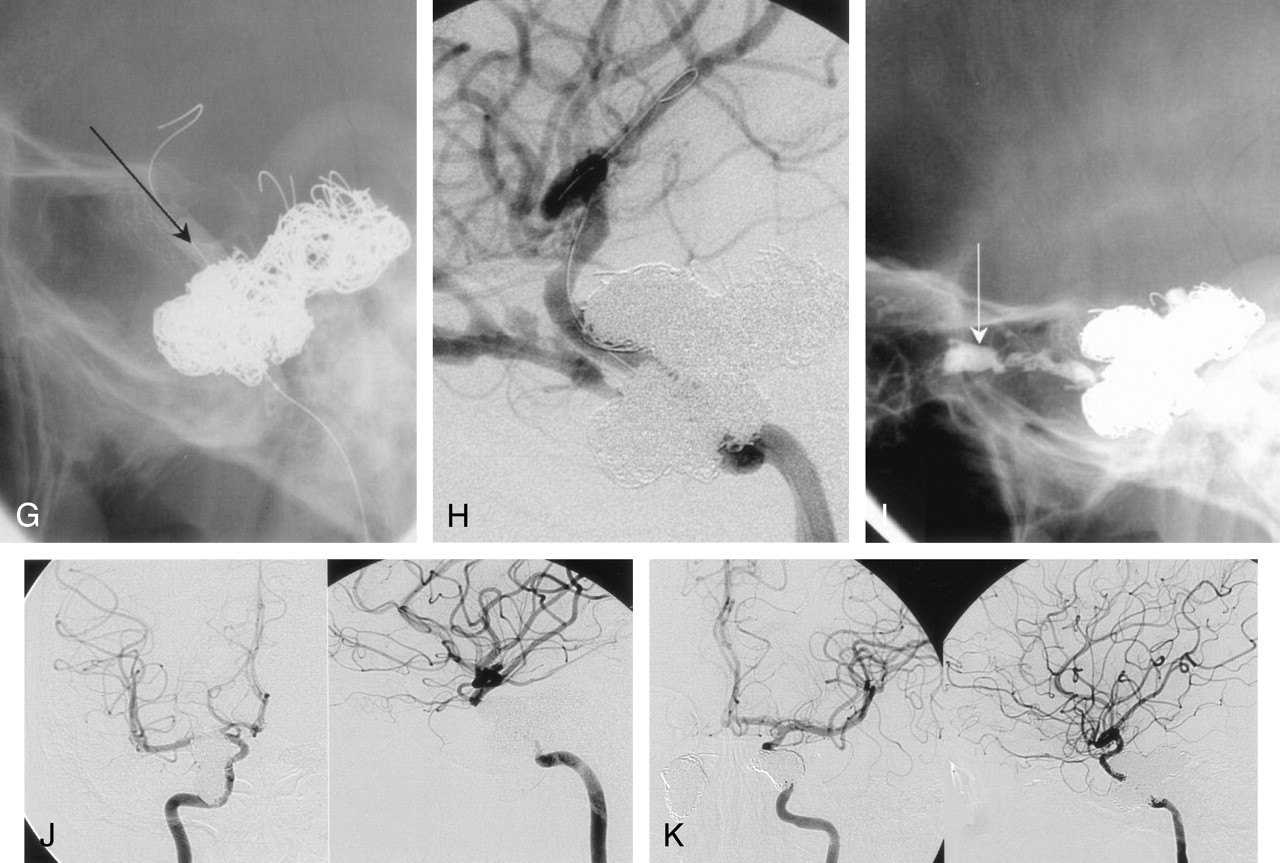
20-year-old woman (patient #3, Table 1) injured in an equestrian accident with multiple skull base fractures and bilateral carotid cavernous fistulas. A, Lateral projection of right common carotid artery arteriogram shows type A carotid cavernous fistula with no filling of the intradural segment of the internal carotid artery. Note prominent intracranial and orbital venous drainage. B, Lateral projection of right vertebral artery arteriogram demonstrates forward filling into right internal carotid artery. No demonstration of the communication between the proximal and distal internal carotid artery is seen. C, Lateral projection of right internal carotid artery angiogram following stent deployment with reconstruction of the vessel shows that there is now brisk antegrade filling of the internal carotid artery distal to the site of the fistula. D, Lateral projection of left internal carotid artery arteriogram shows type A carotid cavernous fistula. Although there is antegrade flow distal to the site of the fistula, the course and caliber of this segment of the internal carotid artery could not be determined. E, Lateral projection of left internal carotid artery arteriogram after stent deployment shows improved visualization of the cavernous segment of the internal carotid artery. Venous drainage to orbital veins persists. F, Lateral unsubtracted projection demonstrates bilateral stents in place (arrows). G, Lateral right internal carotid artery angiogram, unsubtracted, shows an inflated balloon inside the stent (arrow). This was used during coil deposition. H, Lateral projection of left internal carotid artery arteriogram demonstrates persistent flow after extensive coiling. I, Lateral projection of left internal carotid artery arteriogram shows a small aliquot of liquid adhesive (arrow) that was instilled in the proximal portion of the superior ophthalmic vein. This resulted in complete closing of the fistula. J-K, Frontal and lateral projections of right internal carotid artery (J) and left internal carotid artery (K) on 3-month follow-up arteriogram demonstrate patency of both internal carotid arteries with antegrade filling of their branches, dense coil packing, and complete closure of the fistulas.

62-year-old woman (patient 5, Table 1) with sudden left-sided ptosis. A, Frontal projection of left internal carotid artery arteriogram confirms type A carotid cavernous fistula with poor antegrade filling of the internal carotid artery branches. Note extensive venous drainage to superior ophthalmic vein, pterygopalatine plexus, and both inferior petrosal sinus and contralateral cavernous sinus. B, Lateral projection of left vertebral artery arteriogram does not demonstrate communication between the proximal and distal internal carotid artery segments. The right internal carotid artery arteriogram (not shown) also did not demonstrate a connection between these two segments. C, Lateral unsubtracted projection demonstrates the stent in place (arrow). D, Lateral road map image of left internal carotid artery arteriogram shows inflated balloon in stent (triple black arrows), used during coiling to prevent coils from coming into the arterial lumen, which could not be visualized. Note microcatheter in inferior petrosal sinus (white arrow) for transvenous embolization. E, Lateral projection of left internal carotid artery arteriogram after extensive coiling with almost complete obliteration of the aneurysm and carotid cavernous fistula. Note small residual aneurysm (arrow) and antegrade filling of the internal carotid artery branches. No additional coils could be placed. F, Lateral projection of left internal carotid artery on 6-month follow-up arteriogram demonstrates stable appearance of the aneurysm and carotid cavernous fistula with normal antegrade filling of the internal carotid artery. G, In lateral unsubtracted projection of left internal carotid artery on 6-month follow-up arteriogram, the stent demonstrates the lumen (arrow) of the internal carotid artery.
Results
All 6 carotid cavernous fistulas were completely obliterated by stent-assisted coiling from either a transarterial (n = 3), transvenous (n = 3), or combined approaches (n = 1) The internal carotid artery was preserved in all 6 patients. There were no procedure-related adverse events. At 3- and 6-month follow-up, the clinical outcome was excellent in all patients with complete recovery from symptoms except for a residual cranial nerve dysfunction in 2 patients. Both of these patients had severe closed head injury, and the cranial nerve dysfunction was thought to be due to nerve injury from the trauma. Follow-up angiograms obtained in 3 patients at intervals between 3 and 6 months showed no evidence of recurrent fistula. There was also no evidence of intimal hyperplasia or thrombus formation in the stented segments of the internal carotid arteries (Table 1).
Summary of 5 patients with 6 type A CCF treated with a combination of metallic stent and platinum coils
Discussion
Since the introduction of the detachable balloon by Serbinenko in 1974 (14), the management of carotid cavernous fistulas has evolved from a surgical approach, usually consisting of trapping of the fistula by ligation of the internal carotid artery above and below the cavernous sinus, to an endovascular approach in which one or more detachable balloons were placed inside the cavernous sinus, and finally to an endovascular approach in which the fistula is closed by using detachable coils that are introduced into the cavernous sinus either from a venous or an arterial approach. Now, with an endovascular approach, most type A traumatic carotid cavernous fistulas can be successfully occluded with preservation of the internal carotid artery. Type A fistulas that are either low flow or associated with extensive laceration of the internal carotid artery are difficult to treat from a transarterial approach. The exact incidence of type A carotid cavernous fistula with such severe injury is, to our knowledge, not established; however, some series report a need for parent artery occlusions in up to 20% of type A carotid cavernous fistulas (2, 3, 10).
Higashida et al (15) reported preservation of the parent artery in 88% (n = 206) of the patients whom they treated using detachable balloons. Others describe a need for parent artery occlusion in as many as 20% of their cases (2, 3). Because of these limitations with detachable balloons (as well as their lack of availability in the United States), there has been increasing use of coils for the treatment of these lesions (16–19).
Closure of a direct carotid cavernous fistula with detachable coils can be achieved by transvenous or transarterial means. Although the transvenous approach is a route more commonly used for the treatment of dural carotid cavernous fistula, it has also been reported for direct carotid cavernous fistulas (20, 21). The transarterial route has been used successfully in many case series; however, there was still a need for parent artery occlusion in approximately 15–20% of the cases (16, 22, 23). There is thus a substantial percentage of patients with type A carotid cavernous fistula who still require occlusion of the internal carotid artery for successful treatment. The availability of stents suitable for use in the intracranial vasculature has increased the tools that are available to treat these difficult lesions. These devices allow initial reconstruction of the damaged segment of the internal carotid artery and then controlled coil deposition into the cavernous sinus.
As shown in our 6 cases, the use of stent-assisted coiling allows staged successful reconstruction of the damaged internal carotid artery and then obliteration of the fistula with preservation of the parent artery. Because most stents used for this application are balloon-expandable, the ability to carefully analyze the morphology of the fistula and to accurately measure the size of the internal carotid artery at the site of injury is, in our opinion, critical because it allows correct choice of the size of the stent to be deployed. Improper choice of stent size may lead to an increased incidence of adverse events because undersizing with poor stent apposition may cause thrombus formation, whereas oversizing may result in arterial rupture.
In our experience, despite excellent biplane simultaneous fluoroscopic monitoring of coil deposition, it is still impossible to be certain that coils, introduced from either the venous or the arterial side, are not herniating through an open stent cell and compromising the lumen of the internal carotid artery. For this reason, we believe that balloon protection of the internal carotid artery lumen during coil deposition is critical. As in other applications in which stents are placed in the arterial system, the ability to premedicate patients with antiplatelet medication before stent placement should offer protection against thromboembolic events.
We have no experience with the use of covered stents in carotid cavernous fistulas. However, on the basis of a limited experience in other applications, we believe that in most instances, these devices are still too stiff to offer a satisfactory solution.
Conclusion
In these patients, stent-assisted coiling was a useful technique for the treatment of their type A carotid cavernous fistulas associated with severe laceration of the internal carotid artery. It should be considered as an alternative to parent artery occlusion in patients with such fistulas.
References
- Received June 15, 2004.
- Accepted after revision November 23, 2004.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Combined use of Onyx and coils for transarterial balloon-assisted embolization of traumatic carotid-cavernous fistulas: a report of 16 cases with 17 fistulas
- Complications of endovascular therapy for acute ischemic stroke and proposed management approach
- Direct puncture of the highest cervical segment of the internal carotid artery for treatment of an iatrogenic carotid cavernous fistula in a patient with Ehlers-Danlos syndrome
- Multimodal endovascular therapy of traumatic and spontaneous carotid cavernous fistula using coils, n-BCA, Onyx and stent graft
- Comparison of the Risk of Oculomotor Nerve Deficits between Detachable Balloons and Coils in the Treatment of Direct Carotid Cavernous Fistulas