
Abstract
Summary: A case of multiple sclerosis presenting during anti–tumor necrosis factor treatment for rheumatoid arthritis is discussed. This association has been reported in the nonradiological literature, but is an important association for radiologists to be aware of, as they may be in a position to first suggest the diagnosis.
Tumor necrosis factor (TNF) alpha is an immunomodulatory cytokine that has been implicated in certain inflammatory diseases, including multiple sclerosis (MS), rheumatoid arthritis (RA), and Crohn disease (1). TNF alpha-blockers include the TNF-receptor fusion proteins etanercept (Enbrel) and lenercept, and infliximab (Remicade), an anti-TNF alpha monoclonal antibody. Etanercept and infliximab are effective treatments in RA and Crohn disease (2, 3). Anti-TNF therapy for RA has been associated with monophasic CNS demyelination (4, 5) and worsening of known MS (6, 7). There is only one prior case report of a first demyelinating episode and new onset of MS following treatment with anti-TNF therapy (8). Here we report a second case.
Case Report
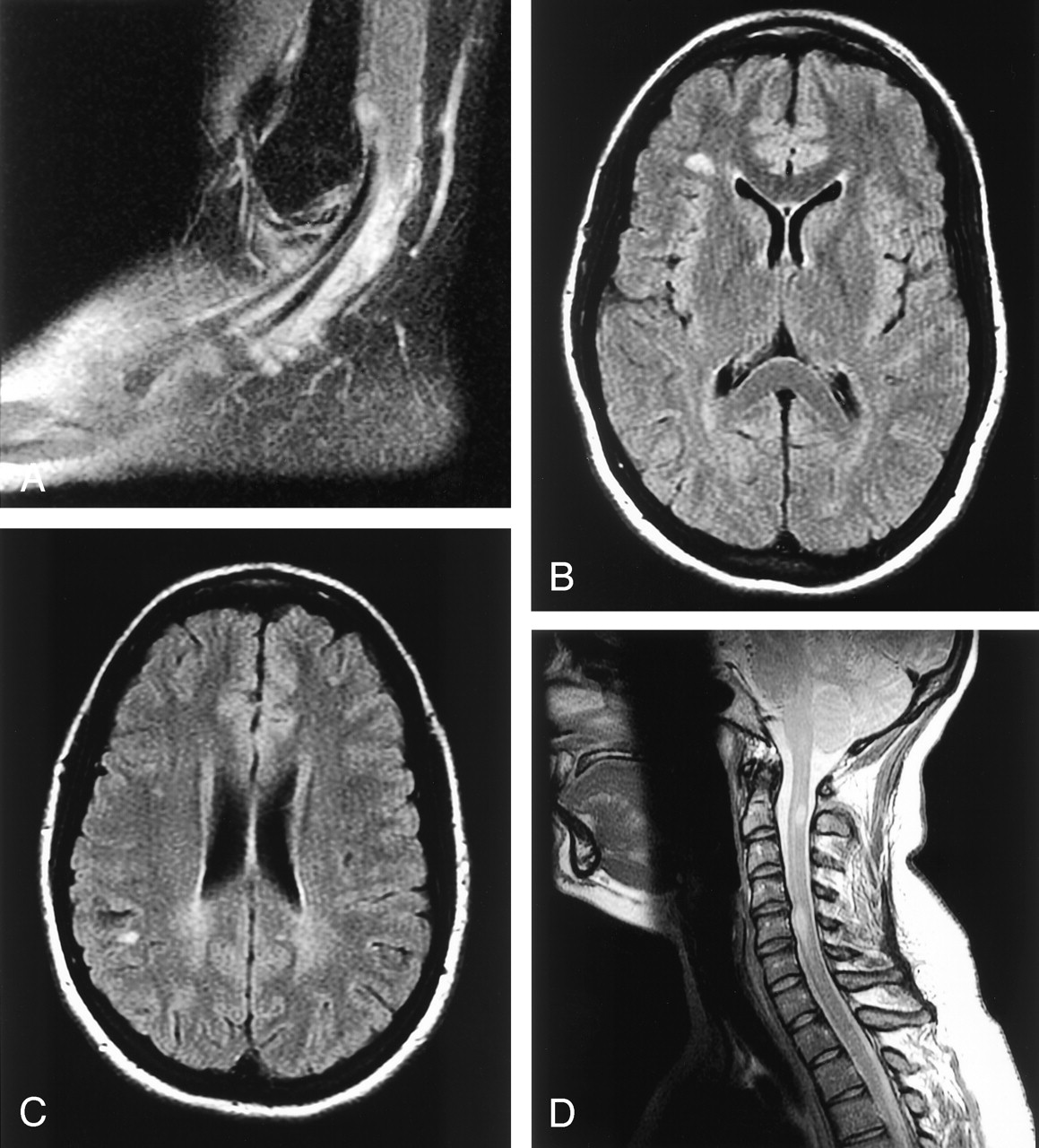
A 33-year-old woman with a 10-year history of RA presented with right-hand numbness, which gradually spread to her arm, chest, and thighs over 6 months, and L’Hermitte sign. She had been treated with etanercept for almost 2 years. Several months before, she complained of ankle pain, shown on MR imaging to be due to inflammatory peroneal tenosynovitis (Fig 1A). There was no prior history of neurologic disease and no family history of MS. The physical examination was remarkable for decreased position sense in her feet and hands. Etanercept was discontinued after MR imaging of the brain (Fig 1B and 1C) and cervical spine (Fig 1D) revealed multifocal cerebral white matter disease and cervical cord lesions, with some lesions enhancing following administration of gadolinium. Within 4 months, lesion enhancement resolved. Six months after stopping etanercept, a repeat MR imaging showed a new cervical cord lesion. Thereafter, she experienced exacerbation of her joint pains from her RA. Several months later and 1 year after stopping anti-TNF therapy, she developed diplopia and bilateral ptosis from supranuclear gaze and left cranial nerve III palsies. An MR imaging of the cervical cord showed significant regression of prior cord lesions, whereas the brain MR imaging showed a new nonenhancing lesion in the periaqueductal region of the midbrain (Fig 2) and a new enhancing lesion in the corpus callosum. She was treated with intravenous methylprednisolone with partial resolution of her symptoms.

A 33-year-old woman with longstanding RA on etanercept treatment, presenting with neurologic symptoms including body numbness and L’Hermitte sign.
A, Sagittal T2-weighted fat suppressed image of the left ankle shows severe peroneal tenosynovitis from the patient’s known RA.
B and C, Axial brain images from fluid-attenuated inversion recovery sequence reveal multifocal white matter lesions.
D, Midline sagittal proton attenuation weighted image of the cervical spine reveals large demyelinating lesions at the C2 and C5 levels.

One year after discontinuation of etanercept, the patient developed new diplopia, gaze deficit, and left cranial nerve III palsy. Shown is an axial T2-weighted image at level of the midbrain, revealing a demyelinating lesion centered in the left periaqueductal region, in proximity to the oculomotor nucleus.
Discussion
Anti-TNF associated demyelinating disease has been described in the neurologic and rheumatologic literature, but we are unaware of similar descriptions in the radiologic literature. Mohan et al in 2001 (4) reviewed cases of neurologic symptoms in patients receiving anti-TNF therapy for inflammatory arthritis reported to the U.S. Food and Drug Administration from 1998 to 2000. Of a total of 20 patients, 18 received etanercept and two received infliximab. Ages ranged between 21 and 56 years, similar to that seen in MS. Sixteen of 19 patients who had MR imaging examinations had findings considered compatible with demyelination, and one patient had clinical optic neuritis with normal MR imaging. Four of these patients had a prior history of either MS or symptoms suggestive of MS (9). The duration of therapy before development of neurologic symptoms ranged from 1 week to 15 months, with a mean duration of 5 months. The most common presentation was paresthesias, followed by optic neuritis. Other symptoms included gait disturbance, weakness, and bladder dysfunction. All patients showed complete or partial resolution of their neurologic symptoms after discontinuing anti-TNF therapy. One patient was rechallenged and experienced recurrent symptoms. Follow-up on these patients, however, is limited, and therefore it is not clear whether these cases were etanercept-induced demyelination or the unmasking of definitive MS.
Sicotte and Voskuhl (8) describe a definitive case of new-onset MS in a 21-year-old woman with a history of RA. The patient developed optic neuritis after 9 months of etanercept therapy. MR imaging of the brain showed several T2 hyperintensities in the white matter and two enhancing lesions. Therapy was continued, and 2 months later there were two new enhancing lesions. At this point, etanercept was discontinued. Six weeks later, she had new neurologic symptoms and the MR imaging showed two additional enhancing lesions.
In this case, the diagnosis of MS was made on the basis of polyphasic occurrence of neurologic events and MR findings, independent of etanercept cessation. Polyphasic disease argues against acute disseminated encephalomyelitis. Cerebral vasculitic ischemic disease can occur in RA. The appearance and location of lesions in this case, however, were typical of white matter disease and not of infarcts. Moreover, in a study assessing the extent of white matter disease in RA on MR images, Bekkelund et al (10) found no white matter difference in RA patients versus control subjects, even when accounting for pharmacologically treated RA (none treated with etanercept) or longstanding RA. In addition, no RA patients studied revealed lesions in the brain stem, corpus callosum, or cerebellum.
The incidence of MS onset associated with anti-TNF therapy is rare but may be underreported because of insufficient follow-up in most cases. It is also unclear how many patients with known MS have been exposed to anti-TNF therapy. Although a causal relationship is not conclusive, the apparent temporal association has raised enough concern that caution is warranted in the treatment of patients with anti-TNF therapy if there is any history of MS or neurologic symptoms suspicious of MS. In these cases, if anti-TNF therapy is initiated, close neurologic surveillance with MR imaging of the brain is recommended (6, 8).
It is interesting that anti-TNF therapy reduces inflammation in RA but may promote CNS demyelinating disease. Indeed, TNF-alpha is implicated in oligodendroctye cell death, active MS lesions are found to contain elevated TNF alpha, and there may be correlation between CSF TNF alpha level and demyelinating disease activity (1, 7, 11). Anti-TNF alpha antibodies and TNF-receptor fusion proteins block experimental autoimmune encephalomyelitis (EAE) mouse model of autoimmune demyelination (11). Trials of an anti-TNF antibody and lenercept in humans affected with MS, however, showed probable disease worsening (6, 7). Proposed theories to explain the apparent discordant response to anti-TNF include the inability of peripherally administered anti-TNF agents to act directly on the CNS, enhanced peripheral autoreactive T-cell activity that then enter the CNS, up-regulation of CNS TNF receptors, elevated interferon gamma, and latent infection (1, 6). It is unclear whether the effectiveness of anti-TNF in EAE is related to greater blood-brain barrier disruption inherent in most cases of EAE or due to a difference in pathophysiology (1).
It is important that radiologists be aware of the rare association of anti-TNF therapy and demyelinating disease, because they may be uniquely able to suggest it as an etiology of white matter changes on imaging and thus may aid clinicians in deciding to discontinue anti-TNF therapy. Furthermore, elucidating the exact mechanism of the apparently paradoxical response to anti-TNF therapy in MS may yield significant advancement in our understanding of the pathophysiology of MS.
References
- Received July 26, 2004.
- Accepted after revision September 16, 2004.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.