
Abstract
BACKGROUND AND PURPOSE: Children often present with enlargement of the nasopharyngeal soft tissues, which is usually due to benign hypertrophy of adenoids. The objective of this report is to emphasize that, although rare, nasopharyngeal carcinoma (NPC) does occur in children and can be diagnosed reliably when certain key radiographic features are recognized.
METHODS: The presenting scans of 11 patients with biopsy proven NPC were reviewed retrospectively by a CAQ-certified neuroradiologist. The age range was 12–17 years (median 15 years). Fifteen scans were reviewed, including 8 CT scans of the neck with intravenous contrast and 7 MR scans of the nasopharynx without and with gadolinium.
RESULTS: All 11 patients had a nasopharyngeal mass. The nasopharyngeal mass had invaded the central skull base in 10 patients (91%). Widening of the petroclival fissure was present in 8 (73%) patients; all except one patient had accompanying skull base invasion. The tumor had extended into the adjacent parapharyngeal space in 6 (55%), the pterygopalatine fossa in 2 (18%), and the masticator space in 2 (18%). Unilateral cervical lymphadenopathy was present in 4 (36%) and bilateral in 7 (64%). Lateral retropharyngeal lymphadenopathy that measured greater than 1 cm in maximal transverse dimension was present in 10 (91%).
CONCLUSION: Pediatric NPC is generally not suspected clinically until late into the disease process. Awareness that NPC can occur in children should prompt careful evaluation for distinctive radiographic features. Earlier diagnosis may then direct the patient to timely appropriate therapy when these key radiographic features are present and recognized.
Benign adenoidal hypertrophy (BAH) is far and above the most common cause of a mass in the posterior nasopharynx in children. Malignant tumors of the nasopharynx are rare in this age group and the histology generally varies with the age of the patient at presentation. Sarcomas and lymphomas are more common in younger children, whereas carcinoma of the nasopharynx (NPC) has a predilection for adolescents and teenagers (1). Unfortunately, these tumors tend to be locally advanced by the time they are diagnosed mainly because the clinical presentation is non-specific (2). Additionally, because they are rare, they may not be high on the list of differential diagnoses in children who present with a nasopharyngeal mass. The therapeutic implications of a delayed diagnosis of nasopharyngeal carcinoma (NPC) can be significant (3). The objective of this report is to emphasize that, although rare, nasopharyngeal carcinoma does occur in children and can be diagnosed reliably when certain key radiographic features are recognized.
Methods
The study population included 11 patients under the age of 18 years with previously untreated NPC diagnosed at our institution from March 1995 to July 2004. Retrospective chart review was carried out to collect pertinent clinical and pathologic data after obtaining institutional review board approval. All patients had histopathologically documented undifferentiated carcinoma of the nasopharynx. Table 1 is a summary of the patients’ demographics and clinical characteristics. The age range was 12–17 years with a median age of 15 years. There were 4 female and 7 male patients. All patients had locally advanced disease and were staged using AJCC staging system (4). All CT scans were performed with intravenous contrast employing contiguous 5-mm slice thickness, average field of view of 22 cm, and a 512 × 512 matrix. MRI scans were performed with a slice thickness of 5 mm (skip 1 mm) or 4 mm (skip 1 mm), most commonly with an 18 cm field of view and a 256 × 224 matrix. All MRI scans were performed without and with intravenous contrast. There were a total of 8 CT scans and 7 MRI scans; 4 patients had both CT and MRI scans. These pre-treatment films were retrieved and reviewed for key radiographic features (Table 2) by a CAQ-certified neuroradiologist (H.E.S.) who was not blinded to the purpose of the review.
Clinical characteristics of patients
Imaging features of NPCs
Results
Table 2 is a summary of the radiographic findings at diagnosis. All patients had an asymmetric mass in the posterior nasopharynx. The mass extended anteriorly to the posterior choana in 7 patients (64%) and into the nasal cavity in an additional two patients (18%). The nasopharyngeal mass had invaded the central skull base in 10 patients (91%). Widening of the petroclival fissure was present in 8 (73%) patients; all except one patient had accompanying skull base invasion. Ten (91%) patients had unilateral postobstructive mastoid opacification and 1 (9%) had bilateral partial opacification. The tumor had extended into the adjacent parapharyngeal space in 6 (55%), into the pterygopalatine fossa in 2 (18%) and the masticator space in 2 (18%). Unilateral cervical lymphadenopathy was present in 4 (36%) and bilateral in 7 (64%). Lateral retropharyngeal lymphadenopathy that measured greater than 1cm in maximal transverse dimension was present in 10 (91%).
Discussion
The National Cancer Institute estimates that approximately 12,400 children and adolescents younger than 20 years of age are diagnosed with cancer in the United States each year. Sarcomas of the soft tissue and bone occur more commonly than malignant epithelial tumors within the head and neck region in children. Carcinoma of the nasopharynx accounts for less than 1% of all childhood cancers (1) and children aged between 10 and 19 years are the most common age-group affected. The clinical experience in diagnosis and treatment of this condition is therefore limited. Benign adenoidal hypertrophy, on the other hand is by far the most common cause of a mass of the posterior nasopharynx in children. In light of this fact, NPC is unlikely to be considered in the differential diagnosis unless the radiologist is aware that NPC can occur in children and therefore deliberately looks for associated secondary diagnostic signs. The objective of this study was to describe salient radiologic features that might help diagnose the condition.
When evaluating significant masses in the posterior nasopharynx, the age of the pediatric patient is an important consideration in narrowing the differential diagnosis. For example, rhabdomyosarcoma or lymphoma is the more likely diagnosis in younger children where as NPC or lymphoma is more common in adolescents (1). The association of non-keratinizing NPC to Epstein-Barr virus (EBV) is well known, and the virus has been associated with NPC in children as well (5). EBV blood titers, however, are of little supplemental value to the imaging findings because of the widespread prevalence of elevated titers in the general population. Children with NPC generally present with neck mass and/or nasal symptoms such as obstruction, bleeding and discharge or fever of unknown origin (2). These patients are generally treated with several courses of antibiotics without response, and ultimately require a biopsy to exclude other pathology such as NPC or lymphoma. However, there are no specific symptoms that point to the diagnosis of NPC. NPC is primarily a disease of adults and its incidence in children varies with geographic location. In China, where there is a high frequency of this tumor, less than 1% of NPC occurs in children under 14 years of age. By comparison, 10–20% of NPC in Tunisia, Uganda, Kenya, Nigeria, and Sudan occur in children (6). In the United States there are reports of higher prevalence of NPC in African Americans, but the relationship of ethnicity to NPC in children is unclear (7).
The primary echelons of lymphatic drainage from the nasopharynx include the lateral retropharyngeal, high level II and high level V lymph nodes (8). The lateral retropharyngeal lymph nodes are therefore commonly involved in NPC as seen in the majority of our patients. In addition, all of our patients also had cervical lymphadenopathy. Adenoidal hypertrophy is also frequently associated with cervical and to a lesser degree retropharyngeal lymphadenopathy in the normal pediatric population making the diagnosis of NPC difficult. Therefore, presence or morphology of enlarged lymph nodes is not diagnostic in isolation. In addition, the morphologic appearance of reactive lateral retropharyngeal lymph nodes can be difficult to distinguish from metastatic lymphadenopathy (9).
Certain radiographic features of the primary tumor can however be very useful in differentiating NPC from benign adenoidal tissue (10, 11). In contrast to benign masses, the configuration of NPC is almost always asymmetric (Fig 1). Local spread of the tumor outside the confines of the nasopharynx is dictated in large measure by the local anatomy. The pharyngobasilar fascia acts as a barrier to local spread of the tumor and tends to direct the advancing tumor towards the central skull base (clivus). Skull base invasion is therefore frequently seen with locally advanced tumors and occurred in the majority of our patients. Invasion of the skull base is more easily recognized on MRI imaging than CT by changes in the marrow signal of the clivus. As demonstrated in Figure 2, patients with involvement of the marrow have decreased signal on T1-weighted images, enhancement post contrast administration and generally increased signal on T2-weighted images. Widening of the petroclival fissure due to infiltration by tumor is best appreciated on CT bone windows and was present in 73% of our patients (Fig 3). Later in the course of the disease, the tumor breaches the pharyngobasilar fascia and gains access to the parapharyngeal space.
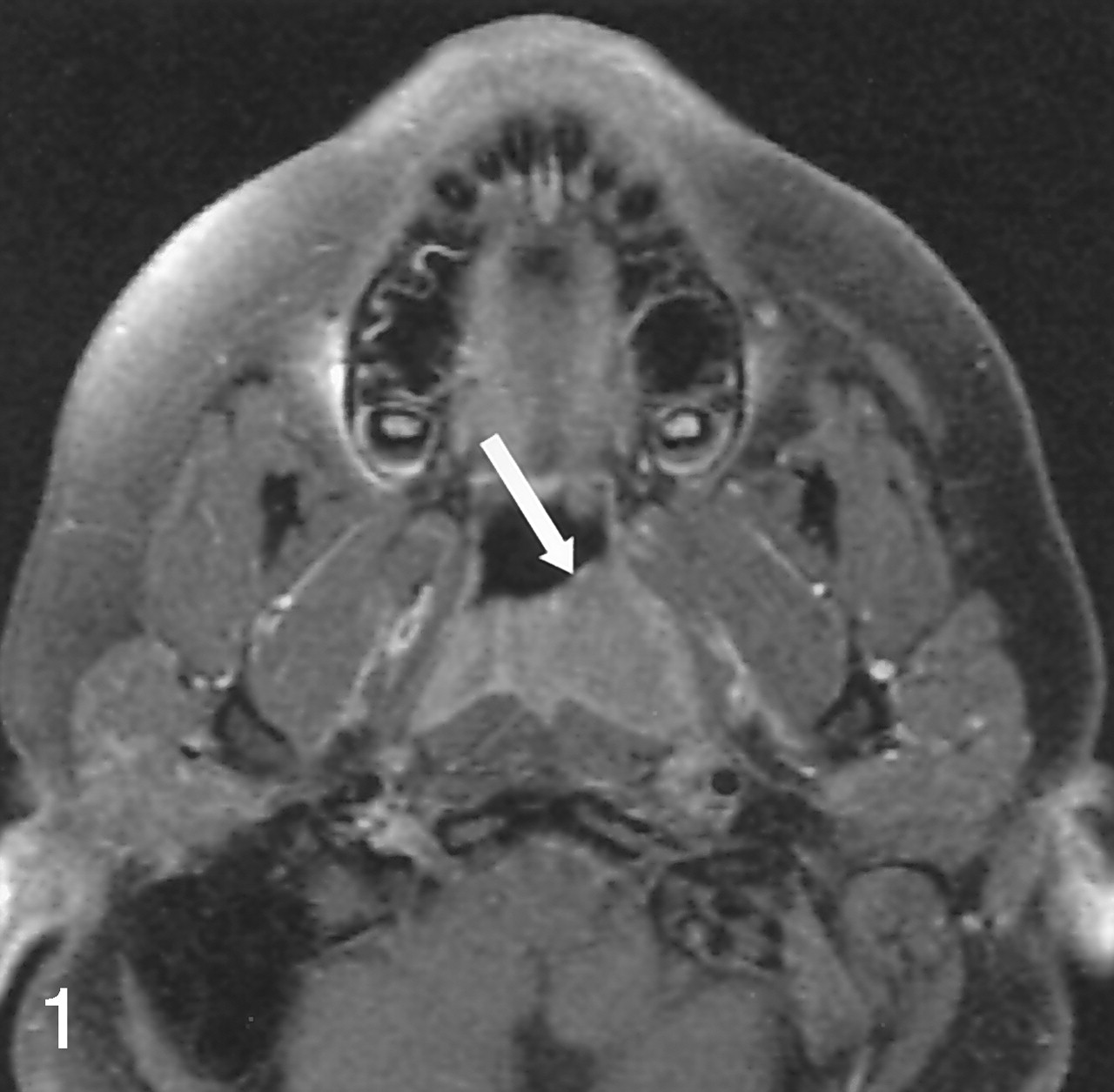
The configuration of NPC is almost always asymmetric as seen in this contrast enhanced, axial T1 weighted fat saturation MRI image (TR = 400, TE = 10.3).
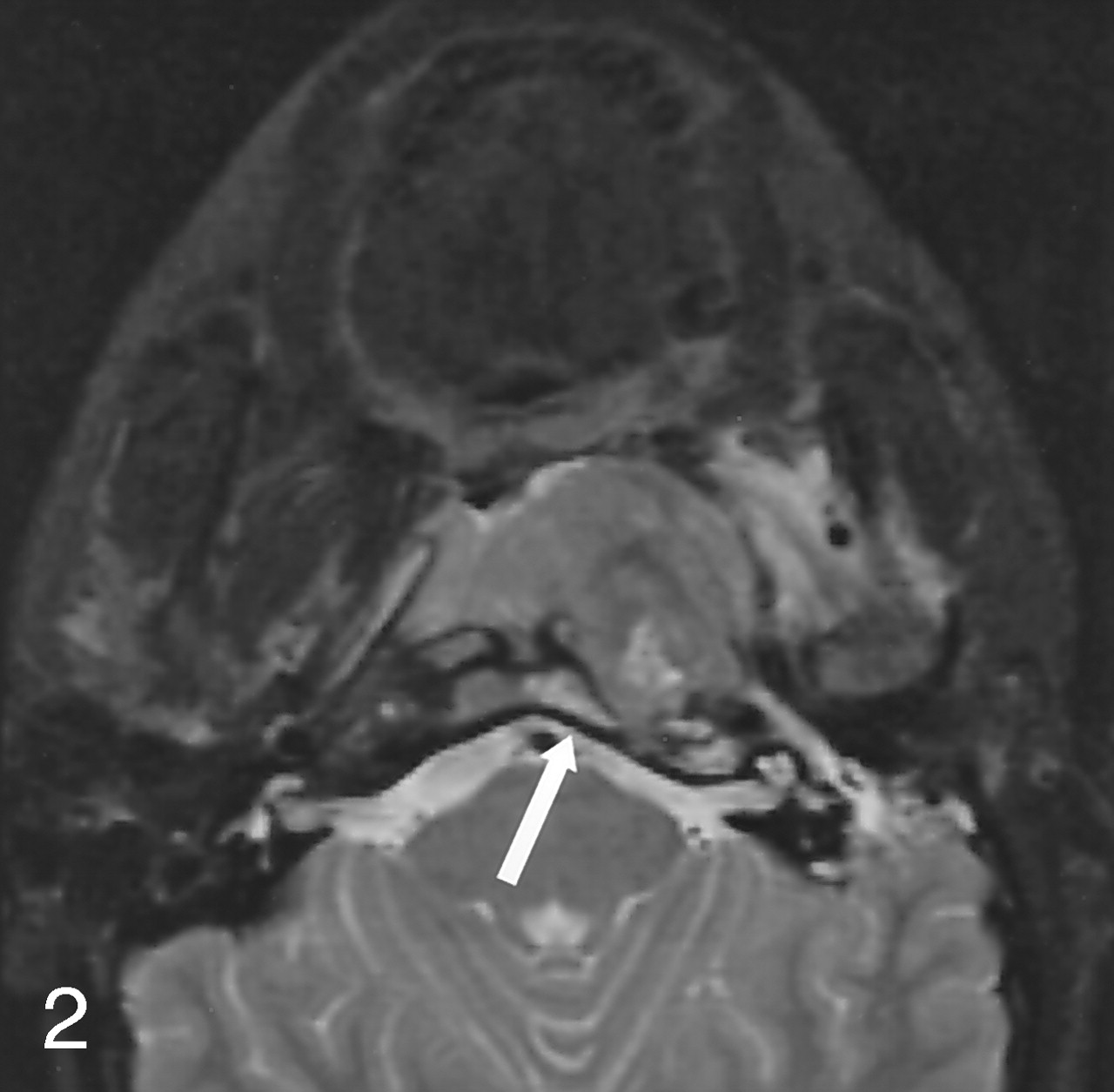
Central skull base invasion. Note high signal in the left aspect of the clivus on this axial, T2 weighted fat saturation MRI image. (TR = 2000, TE = 105).

Tumor extending into and widening the right petroclival fissure (arrows). Soft tissue (A) and (B) bone windows CT neck with contrast.
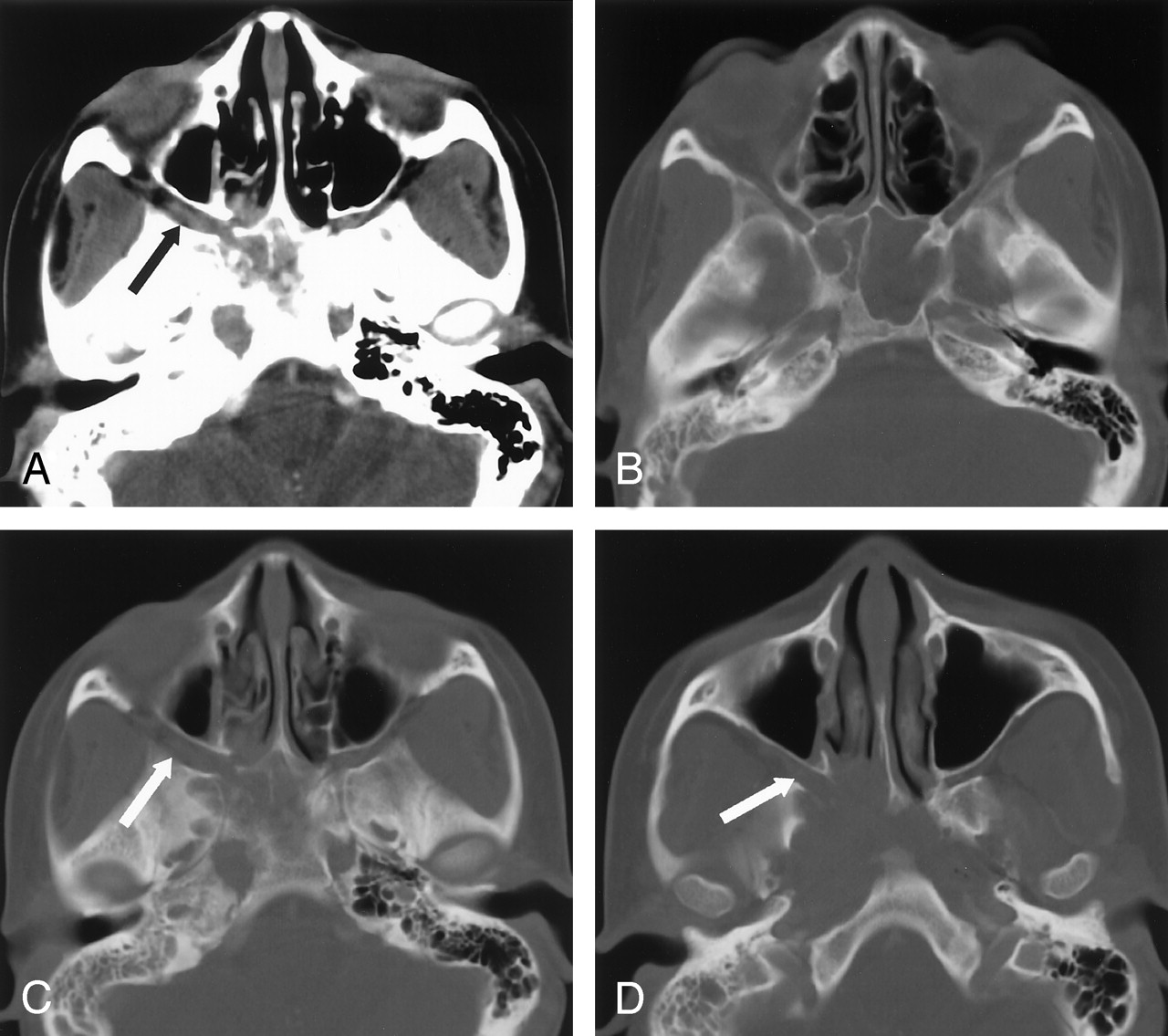
Gross parapharyngeal space invasion was present in just over one half of our patients (Fig 4). More subtle involvement of the parapharyngeal space may be difficult to appreciate, especially if the radiologist does not have NPC on the list of differential diagnoses. Norton et al (12) have suggested that violation of the nasopharyngeal plexus that appears as an enhancing line around the pharyngobasilar fascia may be indicative of an infiltrative tumor. Tumor can also extend to the pterygopalatine fossa causing widening that is easy to detect on CT (Fig 5) and MRI. This finding is however, not common and occurred in less than 20% of our patients. Finally, on rare occasions the tumor can spread into the masticator space to involve the muscles of mastication (Fig 6).

Invasion of the right parapharyngeal space fat. Axial contrast enhanced neck CT.

Tumor extension into and widening of the right pterygopalatine fossa (arrow) seen on soft tissue window image (A) and three consecutive bone window images (B-D) CT neck with contrast.
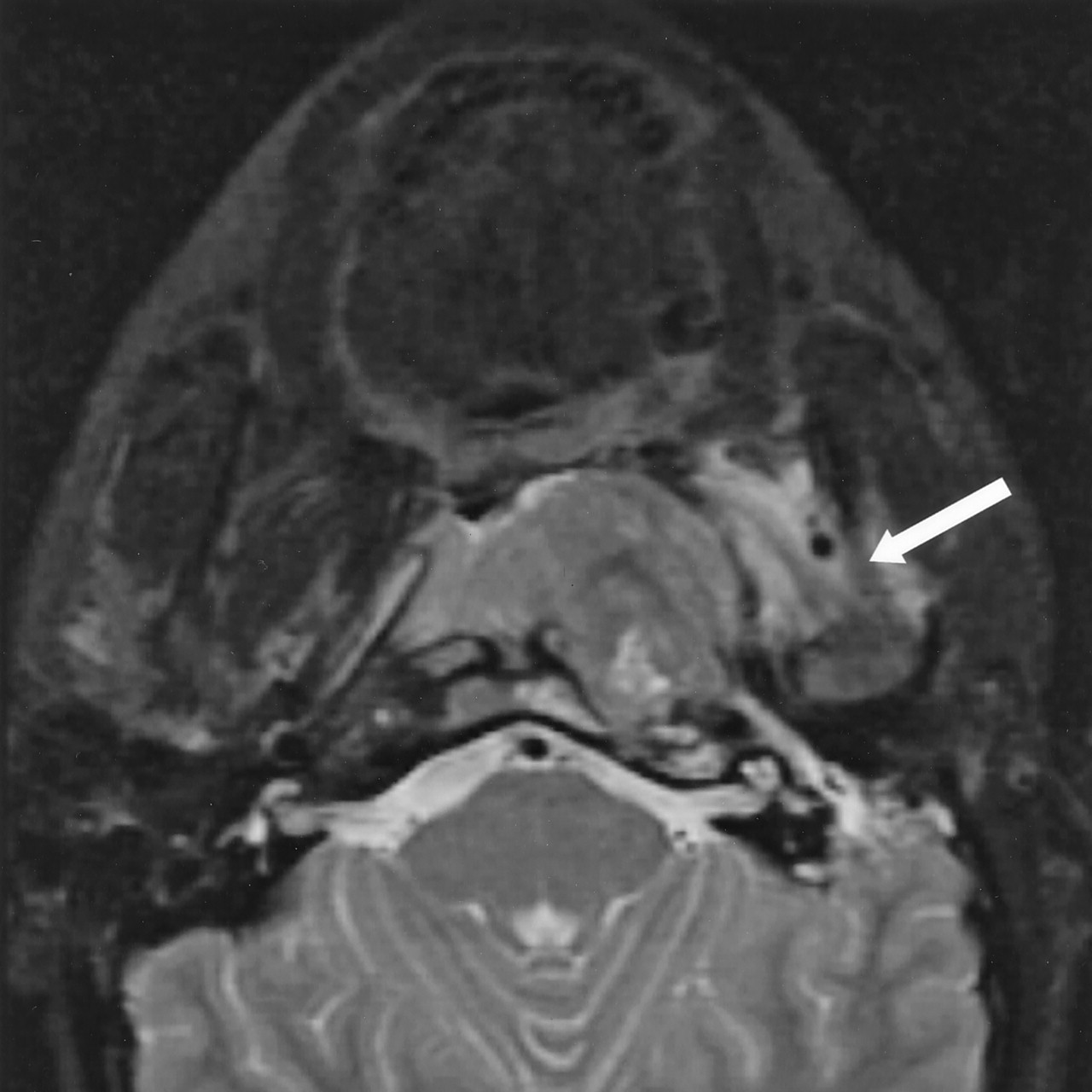
Tumor invading the left masticator space. Axial T2 weighted fat saturation MRI image. (TR = 2000, TE = 105).
The presence of an asymmetric nasopharyngeal mass in itself may not necessarily arouse the suspicion of NPC in children. However, as we have pointed out, the index of suspicion for NPC should be higher if any of the associated radiographic features can be demonstrated.
Conclusion
Pediatric NPC is generally not suspected clinically until late into the disease process. Awareness that NPC can occur in children should prompt careful evaluation for distinctive radiographic features. Earlier diagnosis may then direct the patient to timely appropriate therapy when these key radiographic features are present and recognized.
Footnotes
Presented in part at the 40th Annual Meeting of The American Society of Neuroradiology, Vancouver, BC, May 2002.
References
- Received August 12, 2004.
- Accepted after revision November 11, 2004.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.