
Abstract
BACKGROUND AND PURPOSE: Percutaneous vertebroplasty in the upper cervical spine is a challenging procedure, and little is known about its therapeutic outcome. The purpose of this study was to assess the risks and benefits of percutaneous vertebroplasty for metastatic involvement of the axis.
METHODS: From January 1994 to August 2004, 12 patients (mean age, 52.3 years) underwent percutaneous vertebroplasty via an anterolateral approach using fluoroscopic guidance for metastatic lesions involving the C2 vertebral body; pain intensity was scored on a scale ranging from 0.0 (no pain) to 10.0 (maximum pain intensity). Eight patients (66.7%) were followed up (mean, 6.9 months); 5 of them had percutaneous vertebroplasty indicated for pain control and spine stabilization and 3, for spine stabilization only.
RESULTS: The mean volume of cement injected was 2.9 ± 0.7 mL (range, 2.0–4.0 mL) with a mean vertebral filling of 60.7 ± 14.6% (range, 25–80%). Cement leakage was detected in 7 treated vertebrae (58.3%). Pain improvement was achieved in 4/5 patients (80%). Spine stability was observed in 7 patients (87.5%), but 1 patient (12.5%) presented with a secondary spine deformity in association with partial vertebral filling. Two postprocedural clinical manifestations (16.7%) were observed: 1 patient (8.3%) had a transient occipital neuralgia and another (8.3%) had an ischemic stroke. Mortality and morbidity rates at mean follow-up were 0.0% and 12.5% (1 patient), respectively.
CONCLUSION: Percutaneous vertebroplasty of C2 metastases by an antero-lateral approach is an effective option in the treatment strategy of patients with metastases to C2. Nevertheless, it is a challenging procedure and may carry regional and even intracranial risks due to the proximity to the vertebral artery.
During the past few years, medical progress has resulted in the increase of survival rates among cancer patients, despite an increase in metastatic lesions. Among the different tumors, bone metastasis is the second most common site of metastases, and secondary spine lesions can be found in approximately 30% of cancers (1). Spinal involvement in malignancies can be painful or associated with neurologic manifestations. In some instances, symptoms can be grave, especially in cases of spinal cord compression by a pathologic fracture in the cervical spine.
In metastatic spinal disease, percutaneous injection of polymethylmethacrylate into a vertebral body lesion (percutaneous vertebroplasty) is accepted as an important tool for pain control and is effective in approximately 90% of the patients (2–4). Besides increasing strength and stiffness of the vertebral body, percutaneous vertebroplasty is important for the prevention of further vertebral collapse and spinal cord compression (5, 6), both of which can be life-threatening when metastases occur in the upper cervical spine (7).
Percutaneous vertebroplasty can be performed in the upper cervical spine either by a direct transoral (8–10) or an anterolateral approach (3); from a technical point of view, either approach is much more difficult compared with that of transpedicular percutaneous vertebroplasty in the thoracic and lumbar spine because of potential dangerous complications related to the spinal cord, jugular vein, cranial nerves, carotid artery, and vertebral artery.
To our knowledge, no clinical studies have evaluated the feasibility, safety, and efficacy of percutaneous vertebroplasty for the C2 vertebral body. The aim of the present study was to evaluate the risk and benefits of percutaneous vertebroplasty for the treatment of C2 metastasis by using an anterolateral approach.
Methods
Population Data
The radiologic and clinical records of patients with C2 metastases who underwent percutaneous vertebroplasty at our institution between January 1994 and August 2004 were retrospectively reviewed. Before the procedure, all patients gave informed consent, and our institutional review board did not require further approval for the use of patients’ records and images. For this study, 12 patients were included (7 men and 5 women; age range, 28–73 years; mean age, 52.3 years). Primary tumors were breast (n = 5, 41.7%), pheochromocytoma (n = 3, 25.0%; Fig 1), lung (n = 1, 8.3%), thyroid (n = 1, 8.3%), bladder (n = 1, 8.3%), and unknown (n = 1, 8.3%). Seven patients (58.3%) had multiple spine metastases, and 3 of them (25%) had more than 2 levels involved in the cervical spine. Percutaneous vertebroplasty was performed when pain was not controlled by conservative treatment and was related to the spinal lesion or when the vertebra was at risk of collapse.

47-year-old man with a multimetastatic pheochromocytoma.
A and B, Saggital and coronal CT reconstructions show an osteolytic involvement of the C2 vertebral body with a thinned posterior wall.
C and D, Saggital and coronal CT reconstructions, obtained after percutaneous vertebroplasty, show a homogeneous distribution of cement within the vertebral body with an extension toward the dens. Note cement leakage in soft tissues on the right side (arrow).
Neurologic deficit was a contraindication for percutaneous vertebroplasty, but soft-tissue extension, posterior wall destruction, and vertebral collapse of more than two-thirds of the original height were not considered contraindications. Patients with multiple compression fractures and C2 metastases were treated when the patient complained of pain at the cervical level and when pain elicited by spinal palpation corresponded to a C2 lesion. A C2 lesion was considered at risk of collapse when there was a compression fracture or a lytic lesion involving more than 50% of the vertebral body. Nine patients (75%) underwent percutaneous vertebroplasty for pain control and stabilization, and 3 patients (25%), for spine stabilization without major pain.
Pre- and Postprocedural Imaging
All patients were evaluated before the procedure by CT and MR imaging to determine if there was cortical breakthrough or extravertebral extension or to determine the type of lesion (osteolytic, osteoblastic, or mixed) and to quantify the degree of vertebral collapse. After the treatment, CT images were obtained to assess extravertebral leakage of polymethylmethacrylate and the degree of vertebral filling, which was calculated as the percentage of the vertebral body filled by the cement, as seen on CT images.
Procedure
All procedures were performed in an angiography suite with a C-arm digitalized x-ray system (Angiostar, Siemens, Erlangen, Germany) by the same operator (JC). Before the procedure, all patients were premedicated with intravenous antibiotic therapy (2 g of cefazolin or a combination of clindamycin [1200 mg] and gentamicin [2 mg/kg] in case of allergy). Noninvasive ventilation was administered with a generic mask, and patients were in a supine position under sedation (1 mg/kg per hour of propofol and/or 30 μg of alfentanil chlorohydrate). After preparation of the patient’s skin, we administered a local anesthetic (5 mL of lidocaine hydrochloride 1%), and a right anterolateral access was used to insert a 14-gauge, 10-cm-long bevelled needle (Escoffier, Thonon, France) into the lesion under continuous lateral fluoroscopy. A moderate hyperextension of the neck was required to allow this approach. After reaching the anterior vertebral wall, we rotated and advanced the needle, to be placed in the middle of vertebral body, by an alternate lateral and anteroposterior fluoroscopic monitoring (Fig 2A). Twenty milligrams of polymethylmethacrylate powder (Surgical Simplex P Radiopaque, Howmedica, Rutherford, NJ) was mixed with 5 mL of liquid polymer and opacified with 2 mg of tungsten powder; then when the mixture had the consistency of a paste, it was injected slowly to achieve a homogeneous vertebral filling under continuous lateral fluoroscopy. If a polymethylmethacrylate leakage was detected, the injection was stopped and resumed after a few seconds, after changing the direction of the bevel and the position of the needle tip. A biopsy was not routinely performed before cement injection.
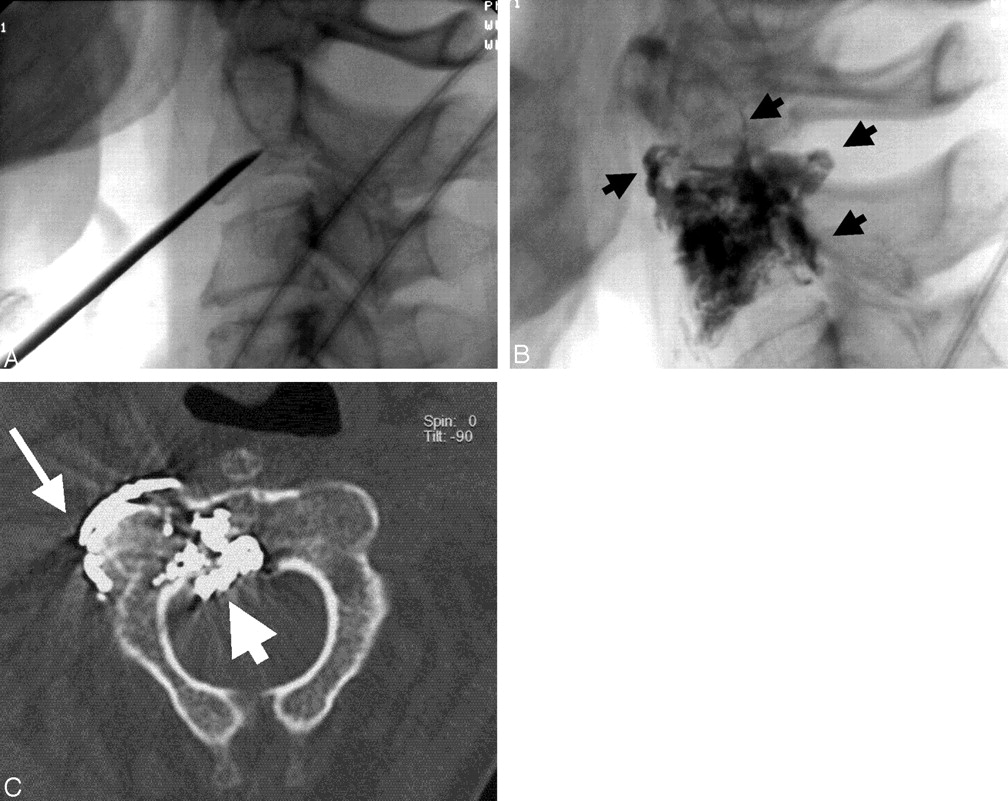
Breast cancer with multiple spinal involvements.
A, Lateral radiograph obtained after placement of the needle shows its oblique trajectory and the approach to C2. Note that the needle is placed at the central part of the vertebral body.
B, Lateral radiograph, obtained after percutaneous vertebroplasty, shows a satisfactory opacification of the vertebral body but also a cement leakage (arrows).
C, Axial CT scan, obtained after percutaneous vertebroplasty, shows cement leakage in the epidural space (short arrow), as well as leakage close to the C1-C2 joint (long arrow). The latter caused a transient occipital neuralgia.
Clinical Follow-Up
All patients had clinical and radiographic reevaluation within 1 month after the procedure, and follow-up ranged from 1 to 18 months (mean time, 6.9 months). The pain intensity in the previously symptomatic region was graded with a semiquantitative scale ranging from 0.0 (no pain) to 10.0 (maximum intensity) on a 10-point pain scale. Pain relief was “excellent” when the pain was completely resolved or had diminished by 75% or more. Pain relief was “good” when the pain had diminished by 50–74%. Pain relief was “moderate” when the pain had diminished by 25–49%. Pain relief was “poor” when the pain had diminished less than 25%. Patients were permitted to stand up 6 hours after the procedure and then were discharged the next day. Narcotic drugs were maintained with the previous doses for 48 hours after the procedure. Thereafter, the patients were permitted to gradually discontinue their medical treatment according to the decrease in pain. Pain was considered improved when pain relief was excellent or good and the narcotic drugs were completely stopped.
The spine was considered stable when no modification in the curvature of the cervical spine or in the height of vertebral body was observed during the follow-up, as seen on CT scans or on cervical spine x-rays.
Results
Percutaneous vertebroplasty was successfully performed in 1 session for all cases. The amount of polymethylmethacrylate injected per vertebral body varied between 2.0 and 4.0 mL (mean, 2.9 ± 0.7 mL) and the vertebral filling ranged from 25–80% (mean, 60.7 ± 14.6%).
Clinical Outcome
Clinical follow-up was available for 8 (66.7%) of 12 patients: 5 of them had percutaneous vertebroplasty indicated for pain control and spine stabilization; and 3 for spine stabilization without major pain. Pain improvement was achieved in 4/5 (80%) patients: excellent in 3 (60%) and good in 1 (20%).
Spine stability was observed in 7 patients (87.5%), but 1 patient (12.5%) presented with a progressive subluxation of C1-C2 with an increase in pain level and then underwent surgery for spinal cord compression. This patient was considered to have no benefit from percutaneous vertebroplasty, although he initially had excellent pain relief.
Technical Incidents and Complications
Postprocedural CT imaging was available in all patients, and extravasation of polymethylmethacrylate was detected in 7 treated vertebrae (58.3%) and localized as follows: paraspinal soft tissues including leakage along the needle track (n = 6, 50%), epidural venous plexus (n = 6, 50%), and paraspinal veins (transverse foramina [n = 3, 25%] and intervertebral foramina [n = 3, 25%]).
Clinical complications were observed in 2 patients (16.7%). One patient had an occipital neuralgia presumably due to a polymethylmethacrylate leakage close to the C1-C2 joint, which resolved completely with antiinflammatory medication after few days (Fig 2). Another patient had cerebellar symptoms and lateral homonymous hemianopsia after the procedure. MR imaging revealed acute cerebellar and occipital infarction, but no abnormalities were identified on MR angiography, either on the vertebral arteries or on the basilar trunk. CT of the cervical spine showed a polymethylmethacrylate leakage into the transverse foramina in the projection of the vertebral artery. CT of the brain was not performed. These symptoms regressed partially during follow-up.
Mortality and morbidity rates at mean follow-up were 0.0% and 12.5% (1 patient), respectively.
Discussion
The upper cervical spine (C1 and C2) is part of a complex biomechanical system (craniocervical junction) that participates in the cranial movement in different planes: extension, flexion, rotation, lateral bending, axial loading, and distraction (7, 11). The cranio-cervical junction comprises the upper cervical spine, the basiocciput, the foramen magnum, and the ligamentous and vascular and neural structures (7).
Many neural and vascular structures pass through the upper cervical spine on their way to support functions throughout the body; therefore, lesions in this area are potentially very serious. Pain is the most common presenting symptom of lesions in this region, but there may be neurologic symptoms (paresthesias, motor weakness, and gait disturbance) from an associated myelopathy; brain stem, cranial, and spinal nerve dysfunction; or a vascular insufficiency secondary to brain stem or spinal cord ischemia (7).
Systemic malignancies can involve the upper cervical spine by either by a direct extension (nasopharyngeal cancer) or metastases, resulting in compression of neurovascular structures or spine instability. Treatment selection is based on the location, stability, and compressive nature of the lesion. Surgery is retained whenever a compression or instability is presented, but the surgical approach (transoral, retropharyngeal, lateral, posterior, or combined) will depend on the site of the lesion and the surgeon’s preference (7, 12, 13).
Even in very experienced hands, surgical treatment of upper cervical metastases is very challenging from a technical point of view; also, the patient’s general medical status can compromise surgical outcome (7, 12, 13).
In some institutions, percutaneous vertebroplasty is considered an important tool for pain reduction and stabilization secondary to metastatic involvement of the spine because it is minimally invasive with a low rate of complications (2–4). The treatment of malignancies by percutaneous vertebroplasty can be proposed as part of the local treatment in association with surgery or radiation therapy or in association with a systemic therapy (hormonotherapy, chemotherapy, biphosphonates, and radioactive iodes) (2).
Some lesions at the C2 level have been treated by percutaneous vertebroplasty by using a transoral route, which is considered to be more straightforward (8–10). The upper cervical spine has also been treated with percutaneous vertebroplasty using an anterolateral approach, which requires extension of the head to elevate the mandible allowing an easier approach to the C2 vertebral body (2, 3). Initially, the carotid artery is located by palpation, and the carotid space is displaced laterally by the operator’s hand; then the needle is placed approximately 1 cm below the angle of the mandible anterolaterally to the visceral space. The needle is advanced carefully in an oblique (posterior, cranial, and medial) direction until contact is made with the anterior wall of C2. The needle tip is engaged into the C2 vertebral body from its inferior and lateral part; then, it is advanced to the middle of the vertebra by successive rotations of the needle bevel under an alternate lateral and front fluoroscopic view (Fig 2A). During the passage of the needle toward C2, the needle crosses progressively the parapharyngeal, retropharyngeal, and prevertebral spaces and care should be taken to avoid injury of the submandibular gland, the structures of the carotid space (jugular vein, carotid artery, and cranial nerves), and the oropharyngeal wall.
Although it appears more challenging, we prefer the anterolateral approach for percutaneous vertebroplasty in the upper cervical spine because there is a decreased risk of infection and the procedure can be performed under sedation with noninvasive ventilation, avoiding intubation in patients whose clinical condition is compromised and whose cervical spine is potentially unstable. Our series confirms that percutaneous vertebroplasty of C2 metastases by an anterolateral approach is feasible when performed by adequately trained physicians; nonetheless, it can be challenging in cases of severe vertebral collapse because hyperextension of the spine is not always possible and needle insertion is especially difficult because of the angle of the mandibula, requiring a further oblique orientation of the needle.
On the basis of our results, we believe that percutaneous vertebroplasty by an anterolateral route is an effective procedure, ensuring pain improvement in most cases (80%). Our findings are in accordance with previous clinical data regarding percutaneous vertebroplasty in metastatic spinal disease in which long-term pain relief occurred in up to 76% of the cases (2–4).
Long-term spine stability was observed in all cases except one, in which a small amount of cement was injected, resulting in a vertebral filling of 25%, and spine instability was noted during the follow-up due to a subluxation of C1-C2. When a vertebral filling is not satisfactory, it is important to perform close imaging follow-up to determine spine stability. In case of instability, a new procedure (percutaneous vertebroplasty or surgery) should be attempted.
Clinical complications after percutaneous vertebroplasty in the C2 vertebral body were detected in 2/12 cases (16.7%). In 1 patient with C2 neuralgia (Arnold’s neuralgia) and a polymethylmethacrylate leakage close to the C1-C2 joint, the symptoms resolved completely after a few days. Regarding the case with multifocal ischemia on the posterior circulation, we could not determine if the embolic mechanism resulted from a polymethylmethacrylate leakage or from a thromboembolism due to a vasospasm secondary to lidocaine injection close to vertebral artery. This patient had a hypervascular metastasis (pheochromocytoma), and he could have potentially presented with a retrograde migration of polymethylmethacrylate through the tumoral vascular network into the arterial feeders, as Casasco et al described (14) for percutaneous intratumoral embolization for hypervascular tumors of the skull base.
The complication rate of the procedure in the C2 level is high and may be very serious if compared with that of percutaneous vertebroplasty for malignancies in general (5%), and this may be related to the special biomechanical and anatomical features unique to the region. Despite that, it can be an interesting tool for the treatment of patients with axial metastases, whose clinical status does not allow long and aggressive treatment and where the goal of the treatment is sometimes more palliative than curative.
Conclusion
In conclusion, percutaneous management of C2 metastases by an anterolateral approach is a useful option in the treatment strategy of patients with axial metastases. Nevertheless, it is a challenging procedure that may carry a risk to neighboring structures, such as the vertebral arteries, with potential intracranial complications.
References
- Received January 31, 2005.
- Accepted after revision February 3, 2005.
- Copyright © American Society of Neuroradiology
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.