
Abstract
BACKGROUND AND PURPOSE: Infants with very low birth weight are at high risk for cerebral lesions. Although supratentorial brain damage is a common radiologic finding, posterior fossa pathologies are rare. We studied the morphology of cerebellar involvement in a large series of 28 premature infants born before the 30th week of gestation to define typical patterns and identify possible risk factors for this pathology.
METHODS: Cranial sonograms were obtained in the early neonatal period. MR imaging was performed between the 2nd month and the 6th year of life. Morphologic patterns of cerebellar involvement were evaluated.
RESULTS: Three morphologic patterns of cerebellar involvement were recognized: (1) symmetric volume reduction of the cerebellar hemispheres, which were floating immediately beneath the tentorium, and a small vermis with preserved shape; (2) symmetrical reduction in hemispheric volume with an enlarged, balloon-shaped fourth ventricle and a small, deformed vermis; and (3) normal overall cerebellar shape with extensive reduction of its dimensions. A small brain stem with flattened anterior curvature of the pons and loss of supratentorial white matter was present in all patients.
CONCLUSION: Symmetric cerebellar volume reduction was found as a consequence of extreme prematurity. Selective vulnerability of the developing cerebellum in the window of 24–30 weeks of gestation, combined with several additive perinatal risk factors (eg, hemosiderin deposits) seems to lead to destruction of immature structures and developmental arrest. Therefore, the resulting condition is the consequence of disrupted cerebellar development.
Extreme prematurity poses a high risk of prenatal, perinatal, and postnatal brain damage. The common radiologic manifestations are periventricular leukomalacia and intraventricular hemorrhage of different degrees. Pathologies of the posterior fossa as a consequence of immaturity are reported (1–8) and their bearing on further development discussed (1, 6, 9). Reduction of cerebellar volume in infants with very low birth weight has been attributed to hemorrhage (4, 5), infarct (3,6), or atrophy (1, 3) or interpreted as crossed diaschisis (2).
The purpose of our study was to characterize the cerebellar morphology of infants with very low birth weight (<1500 g) born before the 30th week of gestation and to test whether this is compatible with the concept of developmental disruption. We present the imaging findings of 28 such infants who, in addition to supratentorial lesions, had pathology of the posterior fossa.
Methods
Patients
We examined 28 preterm infants with severely decreased cerebellar volume, as confirmed on MR imaging. The patients were born between June 1988 and April 2004 and were treated at three neonatal intensive care units. Their age at birth was 24–30 gestational weeks (mean, 26.6 weeks), and their birth weights were 574–1490 g (mean, 962 g). Table 1 shows the patients’ characteristics. (The perinatal risk factors and neurodevelopmental outcome of the patients will be the subject of another report.)
Patients’ characteristics: intraventricular hemorrhage (IVH), hemosiderin infratentorial only estimated in hemosiderin-sensitive sequences
In 18 patients, decreased cerebellar volume was diagnosed in the neonatal period. In nine, the initial diagnosis was made during routine sonography, whereas in the other nine, MR imaging done for various indications led to the diagnosis.
Review of all MR imaging studies of children younger than 5 years of age performed at our institution in the last 6 years revealed another 10 patients with comparable infratentorial pathologies who were also born prematurely.
Imaging
Routine cranial sonograms were obtained at the bedside by using a 7.5-MHz sector transducer (128 XP device; Acuson, Mountain View, CA). Initial scans were acquired in the patients’ first days of life, and at short intervals afterward. In 20 patients, sonograms were available for review, and in seven patients we had to rely on the sonography reports. In all 28 patients, cerebellar pathologies were confirmed on MR imaging.
Initial MR images were obtained between the 2nd month and the 2nd year of life and, in two patients at the ages of 5 or 6 years, by using a 1.5T machine and a circular head coil. Protocols differed but included at least T1- and T2-weighted sequences in two planes with a section thickness of 3–5 mm. Hemosiderin-sensitive T2* sequences were performed in 15 patients (TR/TE = 1343/20; flip angle, 30°).
In 11 patients follow-up MR images (n = 8) or CT scans (n = 3) were available. These were obtained 1–13 years after the patients’ first study. All consecutive MR imaging and CT studies were reviewed.
To characterize lesional patterns in detail, the following MR imaging findings were considered: size of the posterior fossa; brain stem morphology; size, configuration, and signal intensities of the cerebellar hemispheres and vermis; size and shape of the fourth ventricle; parenchymal changes in the cerebral hemispheres; size and configuration of the corpus callosum; width of the lateral ventricles; and hemosiderin in supratentorial and infratentorial areas.
Results
Imaging Results
Sonography.—
In all patients, structures of the posterior fossa were normal on initial sonograms (Fig 1A). Retrospective analysis of the follow-up scans revealed a decrease of cerebellar volume, which developed in the first 3 postnatal months (Figs 1 and 2). Although sonograms allowed for the diagnosis of reduced cerebellar volume, MR images enabled us to establish three morphologic types of impaired cerebellar development.
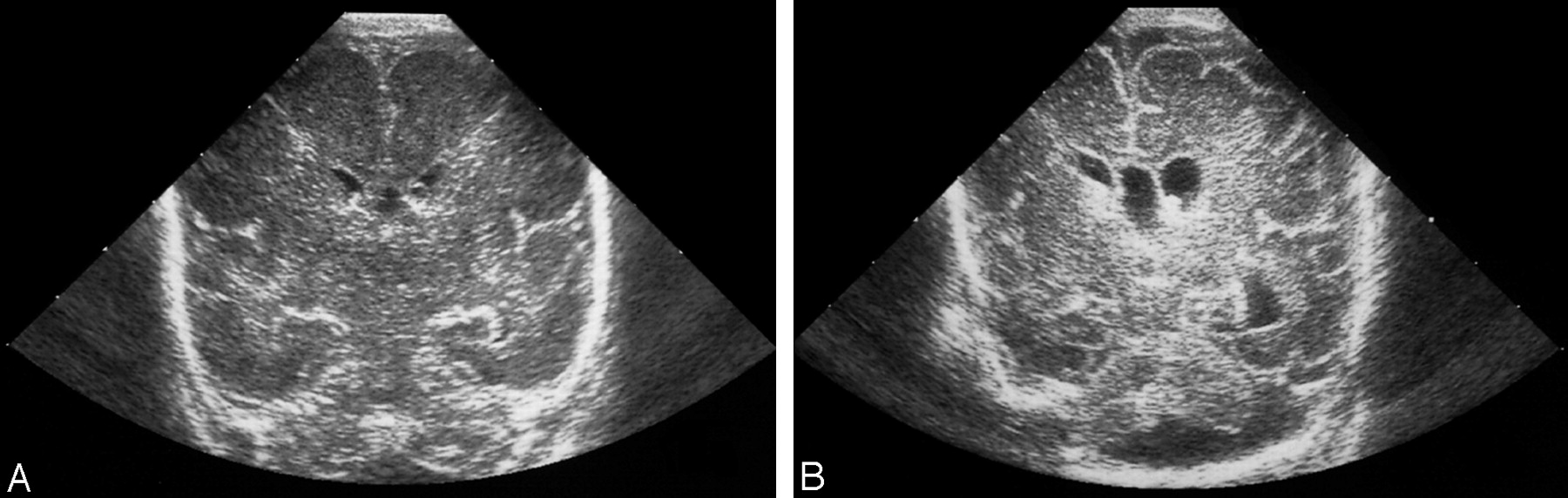
Coronal sonograms in a preterm neonate born at 27 + 5 gestational weeks.
A, Scan on day 1 of life shows normal cerebellar hemispheres.
B, Scan at 3 weeks shows reduced cerebellar volume.

Type 2 disrupted cerebellar development in a preterm infant born at 26 + 3 gestational weeks.
A–C, Sagittal follow-up sonograms obtained on days 57 (A), 86 (B), and 106 (C) of life show a vanishing cerebellar vermis with successive enlargement of the fourth ventricle.
D, MR image obtained at 15 weeks.
MR Imaging.—
Several distinctive features were seen in all patients (Table 2). Symmetric (26 patients) or asymmetric (two patients) reduction in cerebellar volume affected mainly the vertical dimensions with a near-normal transverse diameter. Dentate nuclei were not detected in any patient. The brainstem had reduced sagittal dimensions, and the anterior curvature of the pons was flattened (Fig 2D,3A). The steeply inclined tentorium corresponded to reduced sagittal dimensions of the posterior fossa (Figs 4A and 5A). Loss of supratentorial white matter and a thin corpus callosum were also present in all patients (Figs 3A and 4A).

Type 1 disrupted cerebellar development in a preterm infant born at 29 gestational weeks. T1-weighted MR imaging was performed at 7 months.
A, Sagittal image shows normal configuration of the fourth ventricle, a thin corpus callosum, and an inclined tentorium. The vermis is small but normally shaped. Dimensions of the brain stem are reduced.
B and C, Parasagittal (B) and (C) frontal images demonstrate small cerebellar hemispheres immediately beneath the tentorium.

Type 2 disrupted cerebellar development.
A, Sagittal T2-weighted image shows a balloon-shaped fourth ventricle; a longitudinal, small vermis; and remarkable kinking of the brainstem.
B and C, Parasagittal T2-weighted (B) and frontal T1-weighted (C) images show small cerebellar hemispheres laterally located in the posterior fossa.

Type 3 disrupted cerebellar development in a preterm infant born at 26 + 4 gestational weeks. T2-weighted images show a skeletonized appearance of the cerebellum.
A, Sagittal image.
B, Parasagittal image.
Common morphological features of disruptive cerebellar development
Morphologic Patterns
Although decreased cerebellar volume was the most common feature, the MR appearance varied widely, as different parts of the cerebellum were variably involved. On the basis of the morphologic patterns, we recognized three types of cerebellar volume loss (Table 3).
Special morphological features of cerebellar disruptive development
Type 1.—
Twelve patients had type 1, which was characterized by marked, symmetric reduction in volume. This predominantly affected the cerebellar hemispheres, which were positioned superiorly in the posterior fossa, immediately beneath the tentorium (Fig 3B and -C). Volume reduction was mainly due to extensive loss of white matter. The cerebellar vermis was smaller than usual but without widening of the fissures. Its shape was preserved in most patients, though, in some, the lower aspect of the vermis was smaller than the upper aspect. The fourth ventricle had a normal configuration in eight patients (Fig 3A). In four, the foramen of Magendie was widened, leading to upward displacement of the vermis. Apart from the different shapes of the fourth ventricle, all patients had an uniform lesion pattern. Images obtained with hemosiderin-sensitive sequences revealed hemosiderin deposits in the posterior fossa in three of four patients.
Type 2.—
Nine patients had type 2, with the salient feature of an enlarged, balloon-shaped fourth ventricle and bulging of the foramina of Luschka (Figs 2 and 4). On midline sagittal images, the fourth ventricle lacked its characteristic outline. The cerebellar vermis was markedly reduced in size and lost its shape, remaining as a small longitudinal structure (Fig 2D). The cerebellar peduncles appeared elongated; the small hemispheres were more laterally in the posterior fossa than they were in type 1 (Fig 4C). Hemosiderin in the posterior fossa was found in all five patients for whom hemosiderin-sensitive images were available. Secondary enlargement of the fourth ventricle after vermian shrinkage was demonstrated on follow-up sonography (Fig 2). Damage of the vermis was irreversible despite repeated neurosurgical shunt placement (Table 1).
Type 3.—
Four patients were combined to form a third distinct group. Although the overall shape of the cerebellum was preserved, its dimensions were dramatically reduced. The outstanding features were altered signal intensity of the cerebellum on T2-weighted images, which gave it a skeletonized appearance (Fig 5). In comparison to the supratentorial brain tissue, the cerebellum showed reversed contrast, with gray matter being hyperintense and cerebellar white matter being hypointense. Involvement of the pons was less pronounced in type 3 than in the other types. Two of four MR images obtained with hemosiderin-sensitive sequences showed hemorrhagic residuals in infratentorial areas.
Unclassified.—
The three remaining patients presented with shrunken cerebellar hemispheres containing hemosiderin and cystic pontine and vermian lesions (patient 26, Fig 6). One patient (patient 27) had unilateral cerebellar infarction, which could be followed up with sonography to definite diminution, and one (patient 28) had marked, asymmetric reduction of the cerebellar hemispheres.

Unclassified pattern in a preterm infant (patient 26) born at 24 + 6 gestational weeks. Images show different blood breakdown products in the posterior fossa, shrunken cerebellar hemispheres, and cystic pontine (arrow) and vermian lesions.
A, Sagittal T1-weighted image.
B, Axial T2-weighted image.
C, Axial T2*-weighted image.
D, Coronal T1-weighted image.
Other Findings
All 28 patients had various grades of intraventricular hemorrhage (Table 1). In type 1, <50% of patients developed posthemorrhagic ventricular dilatation, and only one-third required invasive procedures. In all but one of the other patients, posthemorrhagic hydrocephalus led to neurosurgical intervention.
In 11 patients who underwent repeated MR imaging or CT investigations, no progressive cerebellar atrophy (as compared with findings on initial MR images) was visible.
Discussion
A variety of etiologic factors are considered to lead to cerebellar pathologies in infants with very low birth weight. The typically symmetric loss of cerebellar volume, comparable to what we encountered in most of our patients, has been interpreted as “cerebellar atrophy in a familial cerebellar syndrome” (10) and “cerebellar hypoplasia” in preterm children with periventricular leukomalacia (7). The marked symmetry of the reduced cerebellar volume, which all of our types had in common, makes a local event like hemorrhage or infarction unlikely. The morphologic patterns may point to several etiologies and interactions of various pathologic mechanisms. A similar morphologic pattern was found in type 1 and 2, predominantly characterized by loss of white matter. By comparison, the remarkable feature of inversed contrast of gray matter and white matter in type 3 seemed to represent a different entity reminiscent of cerebellar alterations in metabolic disorders, such as congenital disorders of glycosylation syndrome (11, 12). A mechanism such as laminar necrosis of the cerebellar cortex—better known in the cerebral cortex—could be thought to result in a picture like that of type 3 (13).
Selective Vulnerability
Because cerebellar pathologies similar to what we found are not observed in children born after the 32nd gestational week, the disruption may be related to developmental steps that take place in the growing cerebellum at 24–32 gestational weeks. During this period, the layering pattern of the cerebellar cortex changes dramatically. Mitotic activity proceeds in the superficial external granular layer, which is the cradle of internal granular layer neurons. Inward migration of external granular neurons guided by Bergmann radial glial fibers through the molecular and Purkinje neuron layer leads to the formation of the internal granular layer (14, 15). At this transitory five-layer stage, various classes of young neurons in the cerebellar cortex share complex interrelationships (16). Purkinje cells, which enlarge and develop the dendritic trees during this period (16–18) depend on synaptic interactions with Bergmann glial cells, as an important factor for their ordinary development (19, 20). The differentiation of the cerebellar glia starts by the end of the 25th gestational week (16). The sequence of development differs between the various parts of the cerebellum: The vermis is characterized by early differentiation (16) and a later growth spurt in gestational weeks 34–41 (21), and Purkinje cells show maturation that is more advanced in the vermis than in the hemispheres (18). Disruption of these fundamental steps of cerebellar development has devastating consequences.
During this period, selective vulnerability to damage is also due to regulatory alterations of excitotoxic and apoptotic mechanisms, with high susceptibility to any disturbance (22–26). Inordinate activation of afferent pain pathways and hemosiderin deposits may change excitatory glutamate-containing neurotransmitter circuits and cause overfunctioning or prolonged blockade of glutamate and N-methyl d-aspartate receptors; the changes consequently affect immature neurons with a preexisting apoptotic tendency (22, 25). Decreased reaction of two cerebellar glutamate transporters—EAAT4 specific to Purkinje cells and GLAST, which is mainly expressed in Bergmann glia—has been demonstrated in the presence of subarachnoid hemorrhage in preterm neonates (27); however, increased responsiveness of the developing cerebellum to injury during this time is not limited to a specific noxious agent, as impaired cerebellar development has also been found after cytomegalovirus infection, radiomimetic toxins, and ionizing radiation (28, 29) and after hypoxia in the chick model (19). Of note, different reactions to a cell precursor toxin can be demonstrated in different cell types (30).
Hemosiderin
Hemosiderin deposits in the posterior fossa were detected in 12 of 15 patients in whom hemosiderin-sensitive sequences were performed. Primary cerebellar hemorrhage as possible reason for the hemosiderin deposits was not detected, but all patients had supratentorial intraventricular hemorrhage. MR images in both adults and children with superficial cerebellar siderosis reveal unexpected consecutive cerebellar atrophy (31–34). Histopathology shows loss of the Purkinje cells and granular layer at the crown of the gyri and a granular pigment in the subependymal glia (35). These findings suggest that hemosiderin deposits on the cerebellar surface may be a cause of damage to the underlying structures. This damage may be especially pronounced in the immature cerebellum of preterm infants. The high incidence of olivopontocerebellar pathologies and increased glial reaction reported in preterm infants with subarachnoid hemorrhages in the posterior fossa consolidates this hypothesis (36, 37). In this context, the role of oxidative stress and of oxygen radical mediated damage to biologic material for prenatal maldevelopment is discussed (38, 39). In particular, the morphology of type 2 (Table 3) could be explained by hemosiderin-associated cell loss due to the presence of hemosiderin in both the fourth ventricle and in the subarachnoid space.
Differential Diagnoses
In a number of our patients, their condition was first diagnosed as a variant of the wide morphologic field of the Dandy-Walker continuum (40–42). Differentiation was possible on the basis of the position of the tentorium and the missing enlargement of the posterior fossa (Table 2), which are obligatory criteria of the classic Dandy-Walker malformation (41).
Morphologic discrimination of disrupted cerebellar development in preterm infants from pontocerebellar hypoplasia and pontoneocerebellar hypoplasia is complex. In particular, type 1 was almost indistinguishable from pontocerebellar hypoplasia in terms of the pons, the width of the posterior fossa, and the shape of vermis and hemispheres. As in the diverse phenotypes of genetic pontocerebellar hypoplasia, the amount of pontine flattening in our cases varied (8, 43).
Moreover, temporary overlap is observed in the development of both pathologies. Although pontocerebellar hypoplasia has been observed to develop in utero at gestational weeks 22–33 (44, 45), we found similar morphologic changes at corresponding ages after premature birth. Using sonograms, we followed the vanishing of cerebellar volume in the first postnatal months (Figs 1 and 2). These findings suggest that, if normal developmental steps cannot take place, either because of genetically determined factors or as a consequence of noxious agents, the resulting morphology is similar.
Simonati et al (46) considered sporadic pontocerebellar hypoplasia to be the result of impaired maturation at gestational weeks 20–28, probably due to abnormal functioning of genes involved in the patterning of CNS structures. Further evidence suggests a variable pathophysiologic and etiologic background of pontocerebellar alterations in this distinct developmental period. Acquired pontocerebellar hypoplasia has been reported after fetal drug exposure (47, 48), with septicemia in a premature infant (12), and in the donor of a twin to twin transfusion syndrome (49). Vascular undersupply is suggested as a cause of pontoneocerebellar hypoplasia (45, 50).
Despite the morphologic resemblance, the typical clinical features of pontocerebellar hypoplasia (ie, spinal muscular atrophy, respiratory insufficiency, and contractures in type 1 and dyskinesia and early-onset epilepsy in type 2 [28, 51]), and the degenerative course with death mostly in the first years (51–53) were not present in our patients.
Reduced cerebellar volume as a complication of prematurity seems to represent a process encompassing destructive disorder and developmental arrest. Damage of structures during their formation may lead to mimicry of true malformations (8). As destructive events interfere with the development of genetically normal primordia (8,54, 55), the term disruption is appropriate to describe the observed pathology. A preponderance of the one or the other process may lead to different morphologies that are mirrored in the described three morphologic patterns.
Although the clinical presentation of affected children and the mode of genesis are similar, the morphologic classification into three types is important to allow for their adequate recognition and differential diagnosis. Differentiation of type 1 from pontocerebellar hypoplasia is important in terms of genetic counseling because of the nonhereditary nature of the former. Type 2 bears similarity to an entrapped fourth ventricle, but it does not improve after shunt surgery. Type 3 is reminiscent of patterns seen in metabolic disorders, such as congenital disorders of glycosylation syndrome.
Severe reduction in cerebellar volume after prematurity is documented in small series of patients (1–7). Although reports differ with respect to lesion symmetry and etiologic considerations, they agree in gestational ages. Additional lesions of the supratentorial white matter are described sporadically.
We present what we believe is the largest series of patients with disrupted cerebellar development as a complication of premature birth. The large number of retrospective diagnoses made after this entity was identified suggests that the incidence of disrupted cerebellar development is higher than reported so far.
Conclusion
Severe reduction in cerebellar volume with symmetric involvement of both hemispheres and variable changes of the vermis was observed as a consequence of extreme prematurity in preterm infants with a birth weight <1500 g. Because these changes are recognized as sequelae of developmental failure, as well as of acquired damage, we propose the term disruptive cerebellar development, which may appear in three morphologic types. Detailed description of these patterns will facilitate their differentiation from other congenital or acquired conditions. Several risk factors (especially selective vulnerability at 24–30 gestational weeks and presence of hemosiderin) were identified, but none could be singled out to be solely responsible for the described pontocerebellar changes. In assessing cerebellar atrophy in children, the patients’ history should be explored with special reference to extreme prematurity to enable its differentiation from other cerebellar pathologies.
References
- Received November 2, 2004.
- Accepted after revision January 31, 2005.
- Copyright © American Society of Neuroradiology
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Longitudinal neonatal brain development and socio-demographic correlates of infant outcomes following preterm birth
- Preterm birth impedes structural and functional development of cerebellar Purkinje cells in the developing baboon cerebellum
- Accuracy of ultrasound in assessing cerebellar haemorrhages in very low birthweight babies
- New MR Imaging Assessment Tool to Define Brain Abnormalities in Very Preterm Infants at Term
- Ultrasonically detectable cerebellar haemorrhage in preterm infants
- Injury to the Developing Cerebellum: Mechanisms and Consequences