
Abstract
Summary: Endoluminal stent placement is safe and effective in the treatment of symptomatic ostial stenoses of the vertebral artery (VA) and proximal subclavian artery (SCA). However, determining the relative importance of an individual lesion on angiography is difficult when VA and SCA stenoses are concurrent. Pressure-sensing wires help in determining the functional significance of coronary artery stenosis. We present a case of ipsilateral VA and SCA stenoses in which a pressure-sensing wire was used in making interventional decisions.
Percutaneous angioplasty with or without stent placement is an alternative treatment for critical stenosis of the proximal subclavian artery (SCA) or vertebral artery (VA) that offers good procedural and long-term results (1–3). However, the indications for treating intermediate stenoses are still controversial. Angiography demonstrates only the morphology of the lesion, and observers may appreciate its severity differently (4). Furthermore, the hemodynamic effects of tandem intermediate lesions in the ipsilateral SCA and VA are additive and may be underestimated if only the diameters of the individual stenoses are considered.
A pressure-sensing angioplastic guidewire has been developed to evaluate the instantaneous hemodynamic status of the coronary artery, a well-established parameter in determining the functional significance of a coronary artery stenosis (5–7). To our knowledge, however, no report describes the use of this guidewire in VA or SCA angioplasty. We present a case of ipsilateral VA and SCA stenoses in which a pressure-sensing wire was used to make interventional decisions.
Case Description and Technique
A 75-year-old man with hypertension and coronary artery disease had recurrent syncopal episodes. Duplex ultrasonography of the neck revealed nearly absent flow in the left VA. The difference between his right and left brachial blood pressures was 30 mm Hg. Selective VA and SCA angiography revealed a lesion with 70% stenosis at the orifice of left VA, and 50%–60% lesion at the proximal left SCA (Fig 1). The right SCA and VA were patent. Both lesions were intermediate in severity, but the patient was symptomatic for VBI; therefore, we used a pressure-sensing wire to evaluate the actual hemodynamic effect.
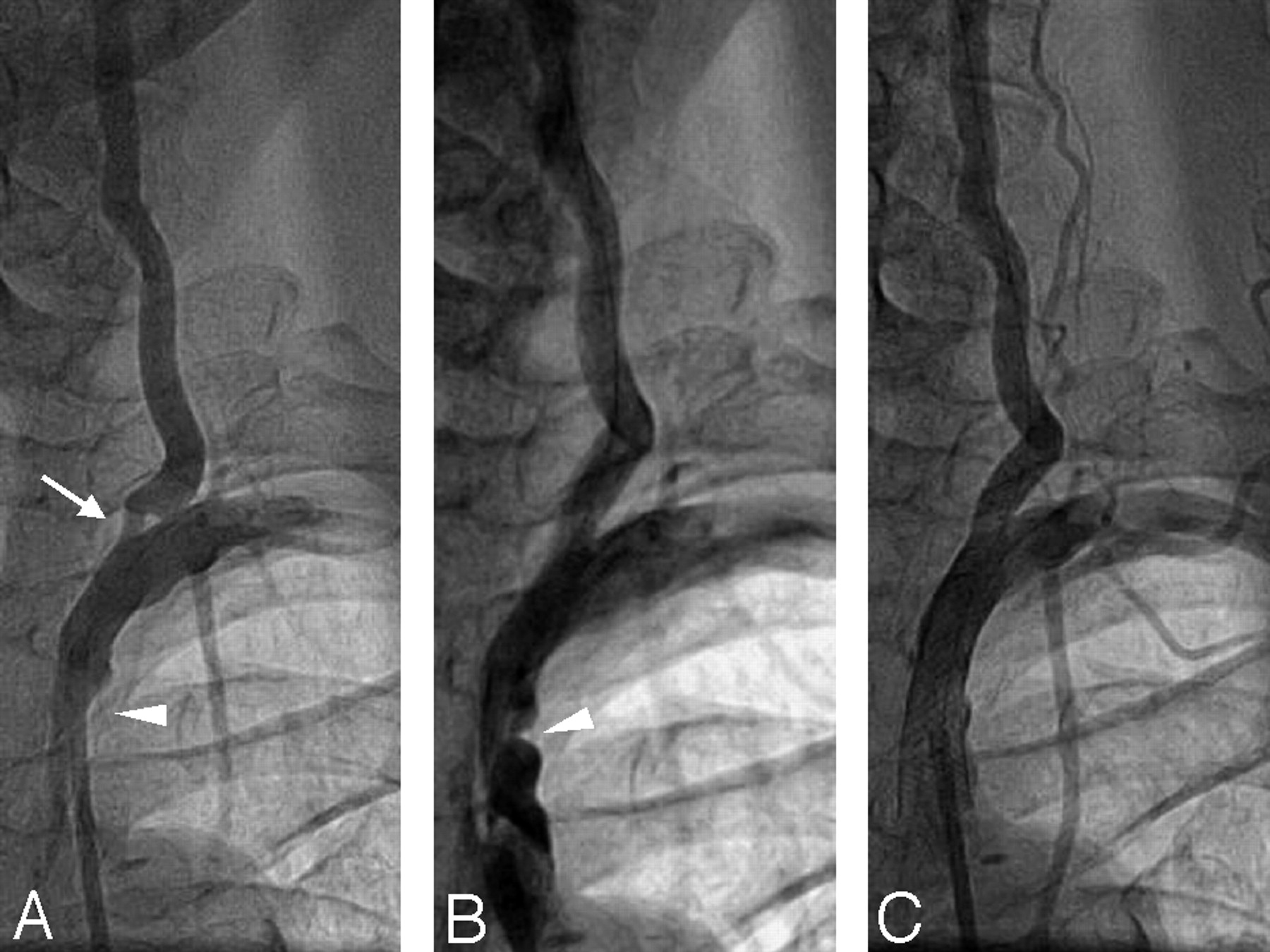
Angiograms.A, Stenosis at the proximal left SCA (arrowhead) and left VA ostium (arrow). B, After stent placement in the VA ostium. C, Final image after stent placement in the left SCA lesion.
Before intervention, heparin 5000 U was administered; the patient’s activated clotting time was maintained between 250 and 300 seconds. A 7F guiding catheter (Mach 1 JR4; Boston Scientific, Maple Grove, MN) was advanced close to the ostium of left SCA. A 0.014-in. pressure-sensing angioplastic guidewire (PressureWire, Radi Medical Systems, Uppsala, Sweden) was advanced across the SCA and VA stenoses into the distal cervical VA. The tip of the guidewire was adjusted with the pressure sensor placed five vessel diameters distal to the VA ostial stenosis. The guidewire was then pulled back into the tip of the guiding catheter while the pressure was recorded continuously. The gradient of mean arterial pressure across the ostium of the VA was 18 mm Hg (distal VA pressure of 60/34 mm Hg [mean, 49 mm Hg], SCA pressure of 95/52 mm Hg [mean, 67 mm Hg]). The gradient of mean arterial pressure across the proximal SCA stenosis was 23 mm Hg (aortic pressure of 128/63 mm Hg [mean, 90 mm Hg]).
The pressure-sensing guidewire was then re-advanced into the distal VA. The distal VA pressure measured by using the guidewire and the aortic pressure measured at the tip of the guiding catheter were displayed simultaneously. Fractional flow reserve (FFR) was defined as the ratio of the mean arterial pressure distal to the stenosis (Pd) to the mean aortic pressure measured from the catheter (Pa), as follows: FFR = Pd/Pa. (5). FFR is a lesion-specific index of stenotic severity that can be calculated by means of simultaneous measurement of the arterial pressures proximal and distal to the lesion. An FFR less than the cutoff value of 0.75 generally indicates hemodynamic significance in terms of coronary intervention. In the patient, the FFR of the VA was 0.45 before treatment (Fig 2), and intervention was considered justifiable.

Tracings of the pressure-sensing guidewire during angioplasty show instantaneous pressure waves and mean arterial pressures detected by using the guiding catheter proximal to the left SCA lesion (red curves) and distal to the left VA lesion (green curves).Yellow curves are instantaneous FFRs (0.45, 0.88, and 0.92).A, Before treatment. B, After stent placement in the VA ostium. C, After stent placement in the VA ostium and proximal SCA.
Using the pressure-sensing guidewire, we deployed a 4 × 12-mm stent (Express 2; Boston Scientific, Galway, Ireland) directly in the VA ostial lesion at 14 atm. A good angiographic result was achieved, and the FFR of the left VA increased to 0.88 (Figs 1 and 2). A 8 × 21-mm carotid Wall stent (Boston Scientific) was then deployed in the lesion in the proximal left SCA. Dilation was performed with a 6 × 20-mm balloon catheter (Gazelle; Boston Scientific) inflated to 18 atm. The angiographic result was optimal, and the FFR of the left VA further increased to 0.92 (Figs 1 and2). The patient was discharged home the next day and was regularly followed up at the clinic, without any recurrent symptoms of VBI.
Discussion
Interventional angiologists desire a real-time index of the physiologic significance of an arterial stenosis, especially in patients with an ambiguous angiographic presentation. The pressure-sensing guidewire is an 0.014-in. angioplastic wire that is fully compatible with interventional procedures. Its design includes a high-fidelity electronic-circuitry pressure sensor located 3 cm proximal to the flexible tip of the wire. With its thin profile and low probability of damping, pressure recordings obtained distal to tight stenoses are reliable. The pressure-sensing guidewire can also detect minute differences in intravascular temperature, and it allows for the calculation of coronary flow reserve by using the thermodilution method (8). The operating pressure range of the sensor is −30 to 300 mm Hg, and its temperature range is 15°C–42°C.
In this case, we recorded pressures while the guidewire was being pulled back to determine the pressure gradients across the stenoses at the ostium of the VA and at the proximal SCA. The gradients were 18 and 23 mm Hg, respectively, and were both significant. The overall 41-mm Hg decrease in mean arterial pressure from the aorta to the distal VA was even more impressive and clearly demonstrated the need for treatment. The pullback maneuver also enables reproducible demonstration of the exact location of stenosis, as in the coronary vasculature (9).
FFR was defined as the ratio of the maximum blood flow in the presence of a stenosis to the normal maximum flow of the artery (ie, if no stenosis were present) (5). Because flow is the ratio of driving pressure to resistance, FFR can be represented as follows: FFR = [(Pd − Pv)/Rmin]/[(Pa −Pv)/Rmin], wherePd represents mean arterial pressure distal to the stenosis,Pa represents the mean aortic pressure, Pv represents venous pressure, and Rmin represents minimal constant resistance (10). According the work of Pijls and De Bruyne (10), if venous pressure is not increased (as is usually the case), the formula can be simplified to FFR = Pd/Pa.
The normal value of FFR is 1.0, which is not affected by variations in heart rates, blood pressure, or myocardial contractility (11). In coronary stenosis, the calculation of FFR by using pressure measurements has been validated in animals and in humans (12–14). An FFR of less than 0.75 generally indicates hemodynamic significance in terms of coronary intervention. Because the coronary circulation is a high-resistance system, Rmin may be achieved during coronary intervention with induced maximal arteriolar vasodilation by using potent vasodilator agents (eg, adenosine, papaverine). This induced hyperemia may further decrease the FFR and help in identifying coronary lesions responsible for exercise-induced myocardial ischemia with a normal baseline FFR (15). We did not induce hyperemia to the vertebrobasilar circulation in our patient, as the overall baseline FFR was already low. In addition, the vascular resistance of the cerebral circulation was low and remained constant. Thus, the influence of resistance on FFR in the extracranial vascular system could be neglected even without induced vasodilation. Future research is needed to establish guidelines for FFR measurement in the VA or SCA, including a standard protocol for vasodilator-induced cerebral hyperemia.
From the experience of coronary intervention, an acceptable endpoint for angioplasty should be an FFR of greater than 0.90 with a good angiographic result (14). In our patient, the overall FFR increased to 0.88 after VA stent placement. According to reported experience with serial angioplasty of tandem lesions in the same vessel (16), the FFR of the proximal lesion can be estimated by using the posttreatment FFR of the distal stenosis after successful angioplasty of the distal lesion. Therefore, though we did not measure the individual FFRs for the VA and SCA after VA stent placement, the FFR of the SCA alone should be 0.88 in our case. Stent placement was still performed, as the pretreatment pressure gradient was high (23 mm Hg) across the SCA lesion and the overall FFR actually increased to 0.92. Studies to establish the treatment indications for individual stenosis in patients with serial or tandem lesions in the ipsilateral SCA and VA are needed.
Conclusions
In this patient, use of the pressure-sensing guidewire was safe and provided an objective indication of the physiologic significance of stenoses in the VA and SCA. Further experience is needed to determine the importance of this information.
References
- Received January 9, 2005.
- Accepted after revision March 2, 2005.
- Copyright © American Society of Neuroradiology
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.