
Abstract
BACKGROUND AND PURPOSE: Endovascular transvenous embolization has been advocated as the treatment technique for dural carotid cavernous fistulas (dCCFs). Most centers use platinum coils primarily. The purpose of this study was to evaluate the technical aspects, efficacy, and safety of transvenous n-butyl cyanoacrylate (n-BCA) infusion in dCCFs as a primary alternative or adjunct to coil embolization.
METHODS: We retrospectively evaluated 14 patients with dCCFs who were treated at this institution from 1999 to 2004 by using n-BCA infusion alone or in combination with coils. The efficacy of treatment and safety aspects were studied in dCCFs of Barrow type B (4/14), C (2/14), and D (8/14). Six patients were treated with transvenous n-BCA infusion alone in the cavernous sinus, 7 with a combination of transvenous n-BCA and coil embolization, and one with transvenous n-BCA combined with transarterial polyvinyl alcohol (PVA)–particle embolization of the feeding arteries.
RESULTS: An angiographic obliteration and clinical cure was achieved in all patients. Technical complications were nonsymptomatic and included spillage of an n-BCA droplet into a middle cerebral artery branch retrograde through the arteriovenous fistulas in one patient and perforation of the inferior petrosal sinus during microcatheter placement in another. A third patient developed temporary palsy of the sixth cranial nerve a few days after the treatment.
CONCLUSION: In this small series, the use of n-BCA either alone or in conjunction with detachable coils was a safe and effective technique for the treatment of symptomatic patients presenting with complex dCCFs.
Arteriovenous (AV) fistulas account for 10%–15% of all intracranial arterial vascular malformations (1), of which carotid cavernous fistulas (CCFs) are a subgroup. Barrow et al classified CCF as direct (type A) or indirect (types B–D) (2). Most carotid cavernous fistulas are of type A and are usually high-flow CCFs caused by trauma and/or aneurysm rupture. The remainders are of dural type, which Barrow et al classified as types B, C, and D, depending on the dural feeders arising from the internal carotid artery (ICA), the external carotid artery (ECA), or both, respectively. Dural CCFs (dCCFs) are usually low-flow fistulas and are thought to be acquired lesions resulting from sinus thrombosis leading to venous congestion with subsequent development of abnormal AV shunts through recanalized dural veins (3).
Therapy depends mainly on the presenting clinical symptoms and venous drainage pattern. Options include observation, which may have a chance of success (4, 5), manual compression of the common carotid artery (CCA), which has been reported to have variable success (6), and arterial embolization of the ECA and ICA feeders with polyvinyl alcohol (PVA) particles, which has a high chance of recanalization (7). Transvenous coil embolization of the cavernous sinus (CS) is well established as a treatment option. In complex dCCFs, however, angiography acquired immediately after the embolization may not show an obliteration of the fistulas (8, 9). Surgical obliteration or a surgical-combined-endovascular approach as well as stereotactic radiosurgery is rarely indicated, though reported (10–12).
Endovascular treatment of dural AV fistulas entails the disconnection of the dural venous outflow path from the arterial supply. In dCCFs this is accomplished by gaining access to the CS and obliterating the sinus or a segment that represents the venous outflow of the fistula(s). Although a transarterial therapy is an option, transvenous embolization of CCFs is a standard primary approach because of its safety, ease of access, and high rate of permanent occlusion (13). Transvenous access of the inferior petrosal sinus (IPS) is readily available even if thrombosed and is frequently used (14–20). Alternative access via the superior ophthalmic vein (SOV) by using a direct approach or facial vein as well as a direct transorbital puncture of the cavernous sinus, is also available when the IPS/SPS (superior petrosal sinus) approach is unsuccessful (21–28). Other less frequently used approaches are through the vein of Labbé, retrograde into the sphenoparietal sinus and into the CS, or by using surgical access to the CS (29, 30).
The purpose of this study was to evaluate the technical aspects, efficacy, and safety of transvenous n-butyl-cyanoacrylate (n-BCA) embolization of dCCFs as a primary alternative or adjunct to coil embolization.
Methods
From 1999 to 2004, 14 patients with dCCFs were treated at our institution by use of a transvenous infusion of n-BCA alone or in combination with coils. The average age of the patients was 63 years (range, 35–93 years). Six patients were men and 8 were women. Table 1 summarizes the patient characteristics, methods of treatment, and approach. Primary presenting symptoms included proptosis, chemosis, ophthalmoplegia, decreased visual acuity, and pain. Four patients had a bilateral type D dCCF. A solely transvenous approach was used in 11 patients (9 via the IPS only, one direct superior ophthalmic vein [SOV] approach after failed IPS access, and one via femoral and then jugular vein to the SOV); a combined arterial and venous route was used in the remaining 3 patients. The venous approach was attempted only after obtaining a complete cerebral angiogram, including selective ECA injections. Procedures were performed preferably with conscious sedation or general anesthesia when patient tolerance was likely to be suboptimal.
Patients with dural carotid cavernous fistulas: clinical data and endovascular techniques
The IPS was always the first method of approach, because it is easily and safely accessed. A 6F guide catheter (Envoy; Cordis Neurovascular, Miami Lakes, FL) was navigated via a transfemoral venous access over a 0.035-inch Terumo glide wire (Boston Scientific, Natick, MA) into the origin of the ipsilateral dilated IPS. In case of an occlusion (2 patients), the access was obtained by using a drilling type action with a 0.035-inch Terumo glide wire with stepwise advancement of a 4F or 5F Terumo glide catheter into the CS (Fig 1). Once the guide catheter was placed within the IPS or the lateral-posterior part of the CS, a retrograde venogram was obtained to evaluate the venous drainage. Subsequently, a microcatheter (Prowler 10, Prowler 14, or Prowler Plus; Cordis Neurovascular) was navigated over an Agility 10, Agility 14 (Cordis Neurovascular), or Transend 14 (Boston Scientific/Target, Fremont, CA) microwire by using roadmap and placed within the CS adjacent to the primary location of the fistula(s). In case platinum detachable coils (Guglielmi detachable coils; Boston Scientific/Target; DCS/Orbit, Cordis Neurovascular; Hydrocoils, MicroVention, Aliso Viejo, CA) were to be placed within the origin of the SOV, the microcatheter was further advanced to the desired position. If the fistulas were bilateral, the microcatheter was navigated into the contralateral CS either through the anterior or posterior dilated intercavernous connection. A 5F catheter, which was used for the transarterial diagnostic angiography, was placed within the dCCF major feeding artery (ECA or ICA) and left there throughout the endovascular procedure. The catheter, which was attached to a continuous heparinized saline drip, was used to obtain control angiograms during the n-BCA infusion or coil placement and to obtain roadmaps for both guide and microcatheter placement. If the catheter was left in the arterial system, the patient’s activated clotting time (ACT) was maintained at 250–300 seconds by using intravenous heparin as a bolus. To reduce existing high-flow within the fistulas and the CS, an arterial embolization was carried out with n-BCA or PVA particles before a transvenous n-BCA infusion (patients 1, 5, and 8; Table 1). Thus, a 5F diagnostic catheter was exchanged for a 6F Envoy guide catheter and a Prowler 10 or Prowler 14 was navigated in a coaxial technique over a microwire for the arterial embolization.
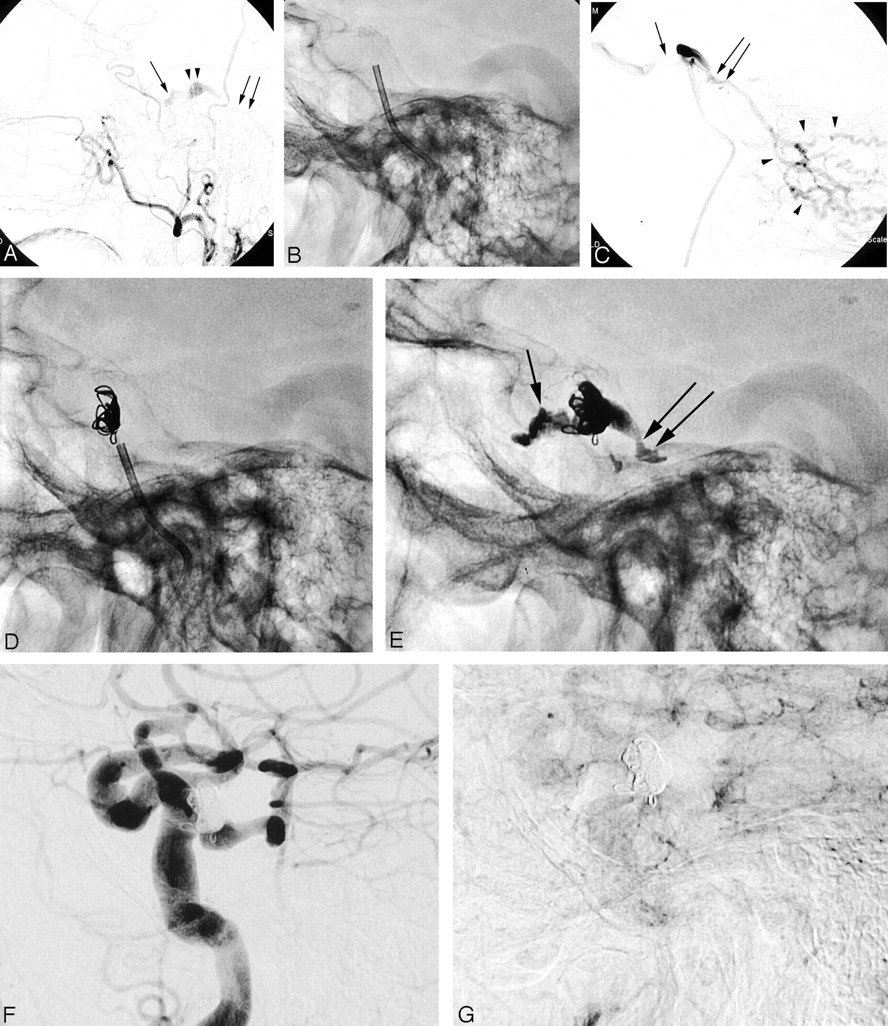
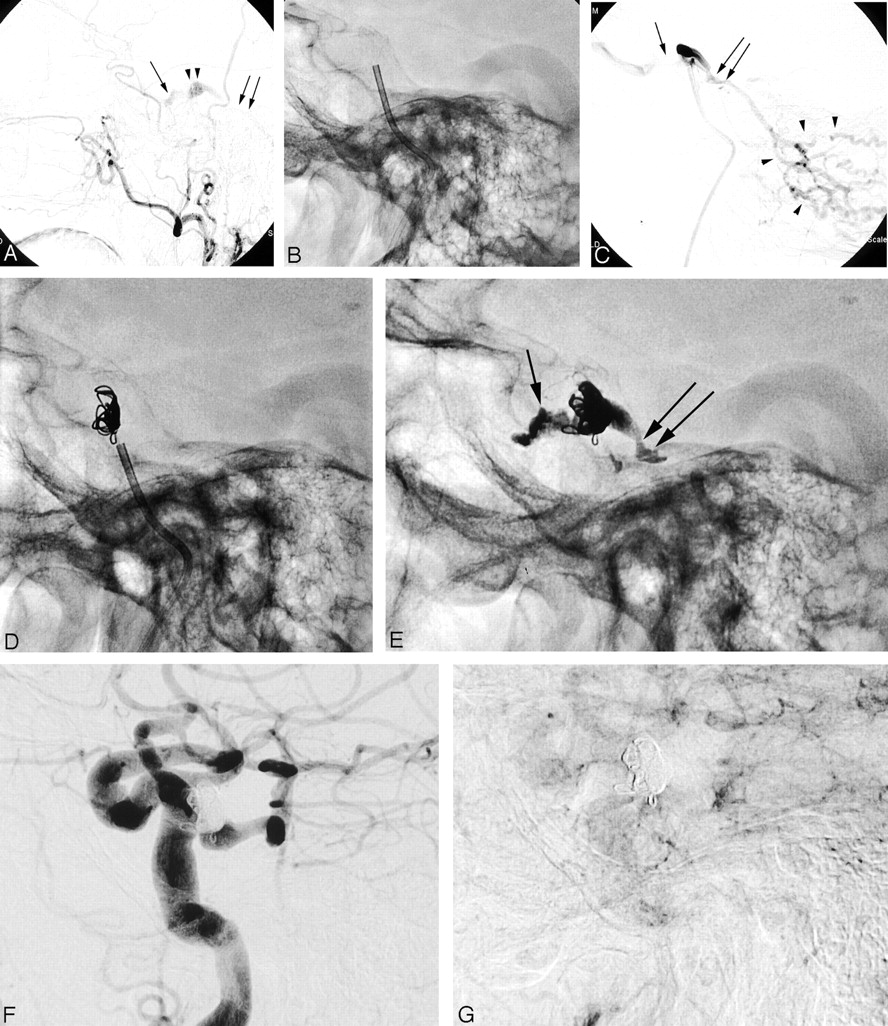
Ninety-one-year-old woman (case 10 [Table 1]), 2 months after radiation therapy for nasopharyngeal carcinoma develops a slowly progressive right orbital swelling, chemosis, proptosis, and ophthalmoplegia. Angiogram shows a CCF with mixed dural artery supply via both ECA (type C, ref. 2). There is a retrograde venous drainage via the right ophthalmic vein and right cerebellar cortical veins. A transvenous n-BCA embolization combined with coils was carried out with successful dural CCF obliteration and complete clinical recovery.
A, Right lateral ECA angiogram shows incomplete filling of the CS (arrowheads) and SOV (straight arrow). Discrete retrograde filling of the congested anterior cerebellar vein is noted (double arrows). Note there is no filling of the IPS.
B, Placement of a 5F guide catheter over a wire through the obliterated IPS into the posterior-lateral segment of the CS.
C, Right lateral CS venogram shows a proximal stenosis of the congested SOV (arrow) as source for the clinical symptoms and filling of cerebellar cortical veins (arrowheads) via proximal superior petrosal vein (double arrow). Note the guide catheter is occlusive within the IPS.
D, Lateral radiograph shows several coils placed in the CS for flow reduction and to protect acrylate spillage into SOV and anterior cerebellar veins.
E, Lateral radiograph shows coils and n-BCA-Ethiodol cast of the entire CS segment depicted in panels A and C, proximal SOV (arrow), and the superior petrosal vein (double arrow).
F and G, Early- and late-phase right lateral CCA angiograms show CCF obliteration.
The washout of contrast material within the CS as seen on the transarterial angiogram or the venogram helped to prepare the appropriate n-BCA/Ethiodol (Trufill n-BCA, Cordis Neurovascular) mixture for embolization. The n-BCA/Ethiodol mixture was varied according to flow rate and anticipated needs in polymerization times (31–33). Concentrations used included the following: 1 : 2, 1 : 3, and 1 : 4 (n-BCA : Ethiodol). The single-column technique was used in all n-BCA infusions, with injection time up to several minutes. For a controlled n-BCA infusion and to prevent pressure build-up in the microcatheter during infusion, the microcatheter was gently withdrawn during the injection. In case of a bilateral CCF, the CS was embolized via the anterior or posterior intercavernous approach and by using gentle withdrawal of the microcatheter during continuous controlled n-BCA infusion with casting of both CS (Fig 2).

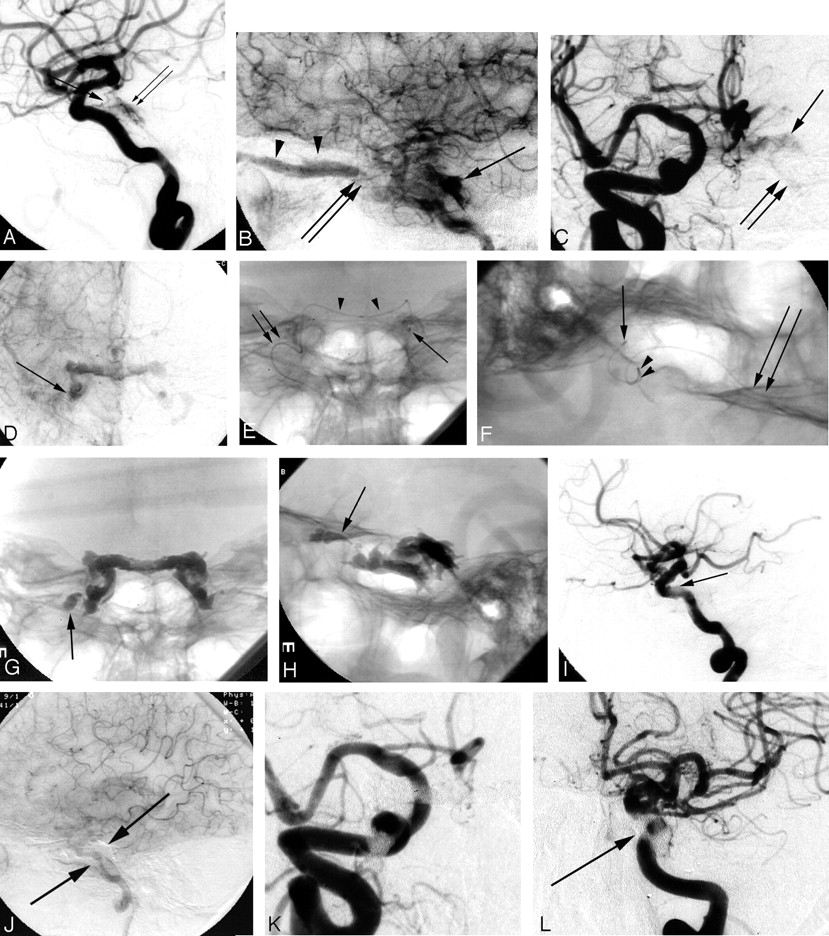
Eighty-seven-year-old woman (case 4, Table 1) presented with progressive ophthalmoplegia, decreased visual acuity, and chemosis. Angiogram shows a CCF with bilateral mixed dural artery supply both via the external and internal carotid arteries (type D, ref. 2), congestion of both cavernous segments with retrograde flow in both SOV. A transvenous embolization was carried out by using n-BCA with complete CCF obliteration and cure of symptoms.
A–D, Early- and late-phase right lateral and frontal ICA angiograms show slow contrast filling (A, thin double arrow) through dural branches of the ICA (A, arrow) including capsular arteries of McConnell at the floor of sella turcica. Retrograde filling of the SOV (arrowhead) with origin stenosis (B and C, double arrows). Note delayed contrast washout (B–D, arrows) of the CS bilaterally.
E and F, Frontal and lateral radiographs show the microcatheter in the left cavernous segment (arrow) before n-BCA infusion. Microcatheter was navigated through the SOV (double arrow) and the anterior intercavernous connection (arrowhead).
G and H, Frontal and lateral radiograph show the n-BCA-Ethiodol cast within the CS bilaterally. Some embolic material spillage is seen in the right proximal SOV through the stenotic segment (arrow). Note the radiolucent structures within the glue cast represent the internal carotid arteries.
I–L, Left lateral early and late phase ICA angiograms (I and J) and right and left frontal angiogram show CCF obliteration. Note artifacts related to the embolic material (arrows).
Intermittent conventional angiography via the arterial system was performed while briefly suspending the n-BCA infusion to confirm progressive occlusion of the fistula (Fig 3). To avoid a SOV occlusion, infusion of n-BCA was preceded by selective placement of coils at the SOV origin or the sphenoparietal sinus in 7 patients (Fig 3). In 6 patients a transvenous n-BCA of the CS was carried out, whereas in one patient the transvenous n-BCA injection was combined with transarterial PVA-particles embolization. Seven patients were treated by using a combination of fibered GDC, Trufill pushable coils/Orbit detachable coils (Cordis Neurovascular), or Hydrocoils and transvenous and/or transarterial n-BCA infusion (Table 1). Clinical follow-up ranged from 6 months to 36 months; cure was defined as complete resolution of the presenting symptoms during the observation period. A 6-month follow-up angiogram was obtained in 4 patients, with 2 patients having a discrete and early filling of the CS immediately at the conclusion of the endovascular procedure.

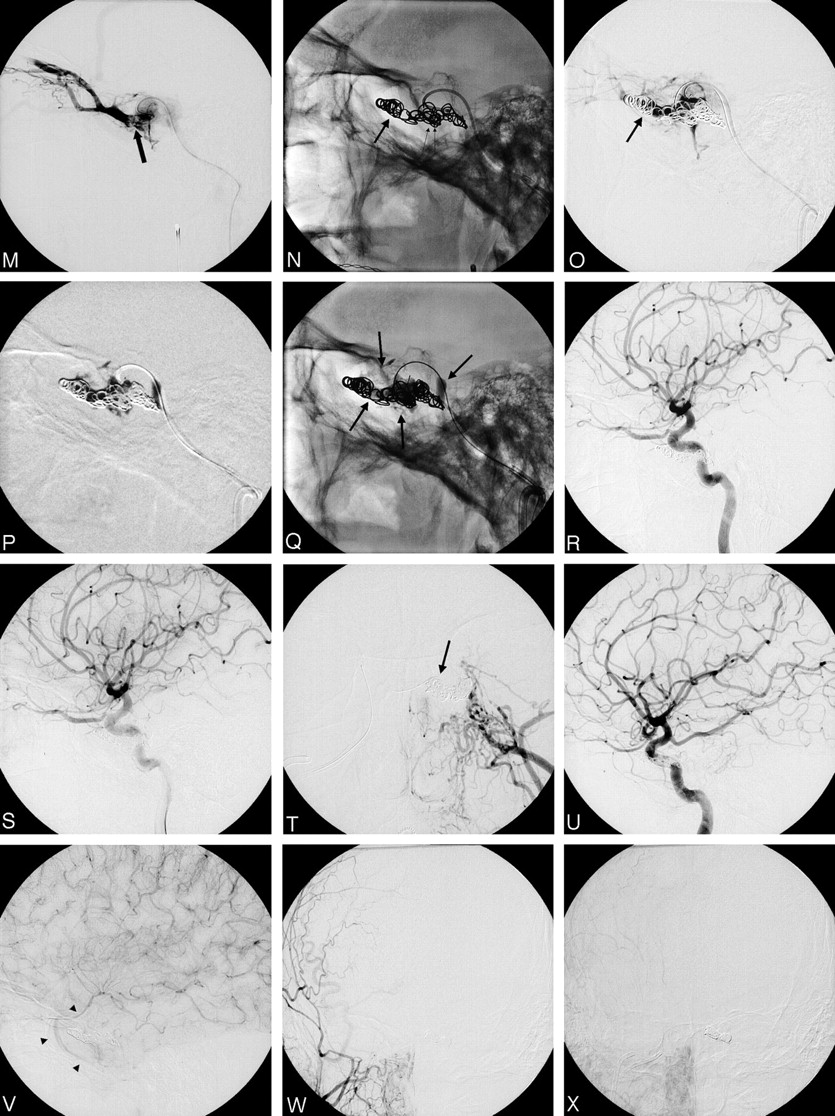
Forty-four-year-old man (case 14 [Table 1]) develops a slowly progressive bilateral chemosis and proptosis. A transvenous n-BCA embolization combined with platinum coils was carried out with successful CCF obliteration and clinical recovery.
A–J, Early and late right ICA lateral (A and B), right ECA frontal (C and D), left ICA frontal and lateral (E–I), and left ECA frontal (J) angiograms show a CCF with mixed bilateral (left > right) dural artery supply via both ECA and ICA (A, B, E, F, G, arrows, Type D-2, ref. 2). There is an early venous drainage via both IPS (D, arrows; I, double arrow), both SOVs (right > left; I, small arrowheads), and the right sphenoparietal vein (F, H, I, arrowheads). Marked dilation of the right CS segment as compared with the left (F and H, small arrows) with prominent “radiolucent” ICA boundaries (F and J).
K and L, Superselective catheterization of the left CS segment through the right IPS and microcatheter tip placement into the anterior-medial segment (arrow). The microcatheter injection shows retrograde filling of both congested SOVs (small arrowhead and small arrows) and the right sphenoparietal vein (arrowheads).
(Continued)M, The microcatheter tip is placed further into the left common ophthalmic vein (arrow).
N, Placement of platinum coils into the common ophthalmic vein (arrow) and cavernous sinus to reduce flow in CS and protect acrylate spillage.
O, Microcatheter control angiography shows filling of the cavernous sinus and the common ophthalmic vein (arrow), but sparse filling of SOV.
P and Q, Acrylate infusion under plain roadmap with casting of the cavernous sinus. Note n-BCA is contained within the coil mass, no spillage into SOV (arrows).
R–X, Bilateral ICA and ECA early and late control angiography shows CCF obliteration with antegrade filling of the sphenoparietal vein and slow outflow (V, arrowheads).
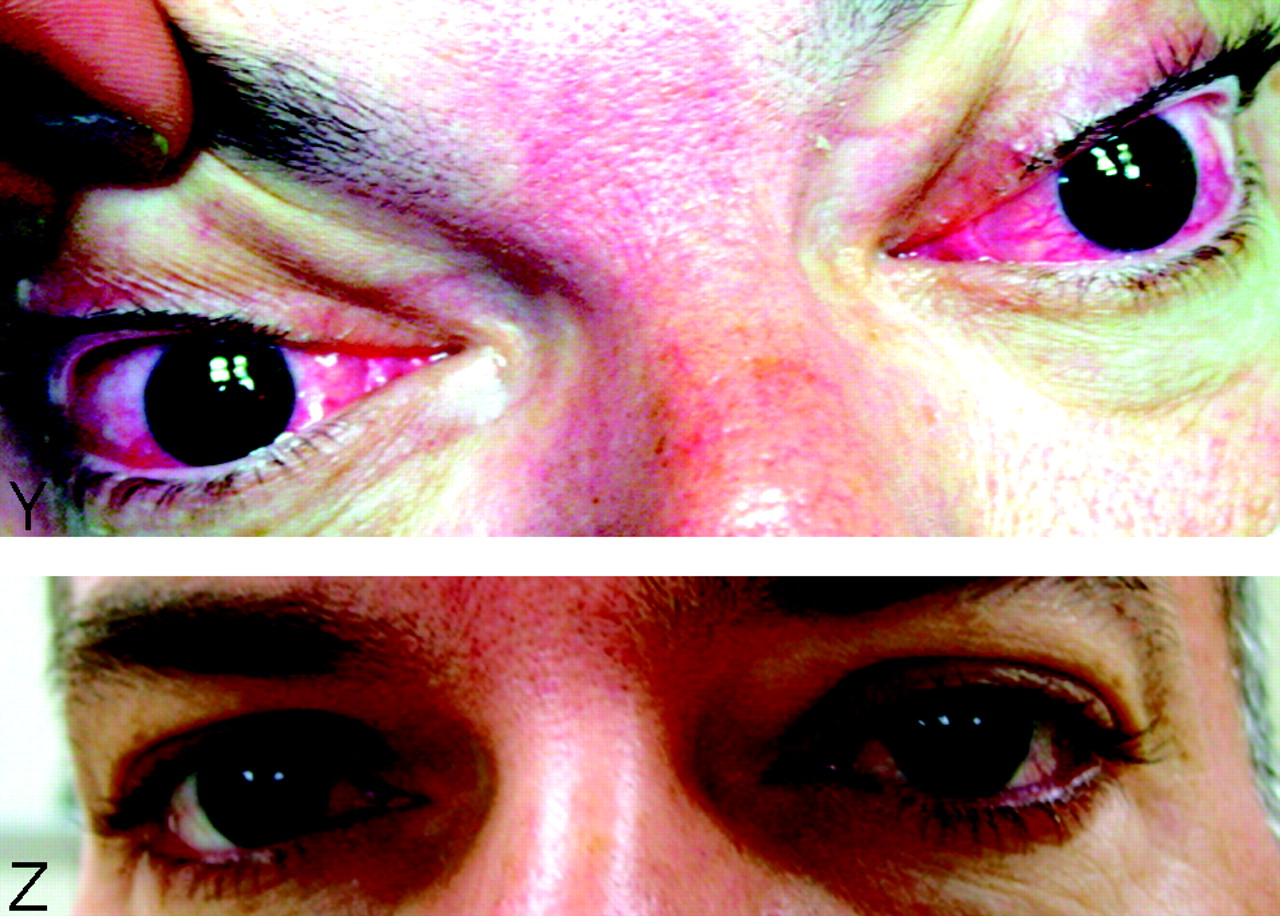
(Continued) Y and Z, Chemosis and conjunctivitis before treatment. Near-complete resolution 2 weeks after CCF obliteration.
Results
Of 6 patients who were treated with n-BCA infusion alone, 5 underwent immediate obliteration of the dCCF. One patient had tiny residual ICA dural feeders that thrombosed, as seen on follow-up angiography at 1 week and at 6 months. Seven of 8 patients who were treated with a combination of n-BCA and coils had an angiographic obliteration of the dCCF at the time of therapy. Immediately postprocedure, one patient had an early and discrete filling of the CS but showed obliteration on the 6-month follow-up angiogram. A complete resolution of the initial presenting symptoms was observed within a few days to weeks. Of the 14 patients treated, a temporary worsening of clinical symptoms was experienced in one patient, followed by progressive spontaneous improvement. Six-month follow-up angiogram in 4 patients, including those 2 patients with initial incomplete occlusion, showed obliteration and no recanalization of the dCCF.
The initial IPS approach failed in one patient (case 1, Table 1), and a cannulation of the SOV through the external jugular-facial vein could not be performed, because of a tight stenosis of the SOV at the CS junction. In a second attempt, the posterior part of the fistula was occluded through the IPS by using n-BCA infusion. Subsequently, residual feeders off the middle meningeal artery were embolized with PVA particles in an attempt to obliterate the anterior component; however, obliteration could not be achieved. A direct access of the SOV via the facial vein was attempted, but failed. Residual filling of the fistula with drainage to the narrowed SOV was present. A successful direct SOV puncture was performed and the CS catheterized. The remnant anterior part of the CS was then obliterated with n-BCA. A single n-BCA droplet was flushed through forceful injection via fistulas into the ICA and subsequently into the distal middle cerebral artery (MCA) territory without any clinical sequelae. Glue was noted to have adhered to the wall of the M4 segment of the MCA, which remained patent but slightly narrowed. The patient was kept on aspirin and Plavix (clopidogrel) for 6 weeks. A 6-month follow-up angiography showed obliterated dCCF and a patent MCA branch. The patient has been asymptomatic now for >3 years.
Patient 3 underwent a successful obliteration of the bilateral dCCF with n-BCA via one of the IPSs and an intercavernous approach. One week after the procedure, the patient developed bilateral worsening of ophthalmoplegia and cranial nerve (CN) VI palsy, proptosis, and chemosis. Angiography showed no filling of the fistula. We attributed the symptoms to the occlusion of the entire CS, which the patient probably did not tolerate. The patient was treated conservatively and slowly recovered back to normal in several months. Patient 5 had an inadvertent perforation of the IPS during microcatheterization of the CS. The leakage was treated conservatively with heparin reversal and remained without any sequelae. Subsequently, the SOV was cannulated via the facial vein, with complete occlusion of the fistula by using n-BCA. In our early experience we observed in one patient (case 4 [Table 1]) a reflux of n-BCA into the proximal SOV without a clinical sequela (Fig 2). Subsequently, in our later practice, coils were placed into the origin of the SOV or the sphenoparietal sinus and in one patient into the origin of the superior petrosal vein to avoid any n-BCA spillage into the SOV or the retrograde draining cortical veins and anterior cerebellar veins, respectively, while embolizing the CS (Figs 1 and 3).
Discussion
Transvenous embolization of CCF was pioneered by Mullan and Hosobuchi in the late 1970s (34, 35). Since then, with the improvement of angiographic techniques and equipment, the transvenous endovascular approach has become a standard primary treatment (14). The therapeutic goal entails disconnection of venous outflow from the feeding arteries at the level of the AV fistulas. In case of a dCCF, the occlusion of the ipsilateral CS or a segment thereof remains the goal for cure. Commonly used embolic agents include detachable platinum coils, 50% dextrose solution, high-grade alcohol, n-BCA, particles, and silk (7, 11, 14). The risks of embolization of CCF depend predominantly on the arterial supply and the venous drainage. A review of the literature on dCCF reveals that most centers use (fibered) platinum coils as the primary therapeutic embolic agent (14, 18, 19). We found reports from only one center, which used n-BCA as the primary embolic agent (14, 36). The advantage of detachable coil systems is that they are potentially retrievable. Coil placement can, however, be limited by the complex architecture or the small size of the affected CS, as in several of our cases, but still symptomatic dCCF (9). Also, incomplete occlusion or recanalization may be observed with the use of fibered coils, especially in bilateral dCCF or multiple fistula sites with a complex dilated CS (9). Recanalization may also be related to proximal obliteration of arterial feeders, or insufficient transvenous obliteration of the draining CS (9). We have seen patients presenting for retreatment after previously reported successful complete coil embolization of the CS for dCCF at other institutions. This may be related to clot lyses after initial thrombosis of the CS or parts thereof and/or reopening of secondary dural branches. To avoid an insufficient thrombosis and an incomplete obliteration as seen with coil embolization, a tight packing of the CS has been suggested. Although tight packing may avoid a recurrence, it can potentially cause iatrogenic CN palsy (37, 38). More recently, Koebbe et al described dehydrated ethanol infusion into the cavernous ICA with distal temporary balloon occlusion in complex dCCF (11). The authors reported successful CCF obliteration in only 3 of 6 patients. In the remaining patients, radiosurgery followed the endovascular treatment. Although there were no complications observed in this small series, risk of brain or CN injury, or damage to the ICA has been discussed (11, 39).
Provided the CS can be accessed via the venous route, a liquid embolic agent such as n-BCA—and potentially in the future, Onyx (MTI, Irvine, CA)—is advantageous in that a fistula can be obliterated with a single infusion, regardless of the size or, the anatomic variability and complexity of the CS. It can also be used as an adjunct to coils, which can help to properly direct the n-BCA infusion and prevent spillage into important inflowing draining veins such as SOV or cortical veins. Coils can also be used to decrease flow in higher flow fistulas for controlled infusion. Forced injection may entail the risk of retrograde spillage of liquid agents via the AV fistula into the ICA. In patient 1, a single droplet was flushed into the distal MCA territory during the injection of n-BCA and layered the arterial wall, without any occlusion. This patient was maintained on antiplatelet agents to prevent thrombosis; a CT did not show any evidence of infarction, but a single n-BCA droplet within a distal MCA branch. The patient has been asymptomatic for now >3 years; however, the ICA can and may need to be protected by using a temporary balloon occlusion in case an AV connection between the infused CS and the ICA is found. Before the planned n-BCA infusion, a venography and forced injection of contrast into the CS through the in-place microcatheter is mandatory to depict the fistulas. Another potential source of venous infarction can be a reflux into cortical veins via the sphenoparietal sinus anastomosis. A preprocedural cerebral arteriogram with a focused review of the draining veins, particularly vein of Labbé, vein of Trolard, and temporal cortical veins, is essential to avert such complications. Reflux into the proximal SOV is also undesirable, because there is a potential for occlusion of the episcleral venous drainage. There is a theoretical risk of CN palsy related to n-BCA—induced inflammatory response in the CS. We did not, however, experience any adverse reaction in our series or find any reports of CN palsy in the literature. Another potential disadvantage of glue embolization is that, if occlusion of the CCF is not achieved, subsequent access through the same venous approach may be difficult. Thus, extra care needs to be taken when there is only one access to the CS, such as in a direct SOV puncture when other access paths have been exhausted. We suggest frequent angiograms via the main supplying ECA or ICA during n-BCA infusion to rule out any filling of the CS. Complete or segmental obliteration of the affected CS, which is the goal of the transvenous obliteration, is well tolerated by most of the patients. In our series, however, one of the patients (case 3 [Table 1]) experienced worsening of CN VI palsy a few days after the treatment but gradually recovered from the symptoms. As described elsewhere, this may have resulted from a complete thrombosis of both parts of the CS, with increased mass effect (11). As in our patient, a particular higher risk may be related to embolization of both parts of the bilateral type of dCCF. Although most of our patients are heparinized during the intervention to keep the ACT values at approximately 250–300 seconds, antiplatelet agents or anticoagulation were not used following the procedure, except in patient 1.
Other potential advantages of n-BCA infusion in dCCF include the relative cost advantage and efficiency of occlusion. Although a vial of n-BCA at the authors’ institution is approximately 1.5–2 times the price of the least-expensive detachable coil, it would be unusual to obtain a fistula obliteration by using <2 coils, particularly if an angiographic obliteration is attempted. Once the microcatheter is correctly placed in the CS, n-BCA is infused in a single injection, causing obliteration, whereas for coils, each coil has to be introduced and detached separately within the CS, thereby greatly adding to the time taken for obliteration of the fistula. Our experience with n-BCA in the treatment of complex CCFs shows that liquid embolic agents are very safe and efficacious for primary transvenous therapy. On gaining experience with glue polymerization time, the ratio of n-BCA to Ethiodol can be estimated. A controlled infusion with a single-column technique can obviate the need for other therapies. This approach reduces the risk of incomplete CCF obliteration, as occasionally seen with fibered platinum coils. Control angiography through the arterial system during n-BCA infusion can prevent “overinfusion” with its potential risk.
Conclusion
In this small series the use of n-BCA injected from a transvenous approach, either alone or in combination with coils, was found to be a rapid, safe, and effective treatment for a variety of dCCFs.
References
- Received July 15, 2004.
- Accepted after revision April 8, 2005.
- Copyright © American Society of Neuroradiology
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Mid- and long-term outcomes of carotid-cavernous fistula endovascular management with Onyx and n-BCA: experience of a single tertiary center
- Intracranial Dural Arteriovenous Fistulae: Clinical Presentation and Management Strategies
- Surgical access on the superior ophthalmic vein to the cavernous sinus dural fistula for embolization
- Use of Onyx for Transarterial Balloon-Assisted Embolization of Traumatic Carotid Cavernous Fistulas: A Report of 23 Cases
- Onyx 18 embolisation of dural arteriovenous fistula via arterial and venous pathways: preliminary experience and evaluation of the short-term outcomes
- Brain Aneurysms and Arteriovenous Malformations: Advancements and Emerging Treatments in Endovascular Embolization