
Abstract
BACKGROUND AND PURPOSE: Measuring blood pressure (stump pressure) in the distal internal carotid artery during occlusion of the internal carotid artery is reportedly a reliable safety index with which to predict ischemia following permanent occlusion of the internal carotid artery. We compared the stump pressure during occlusion of the internal carotid artery with single-photon emission CT (SPECT) using technetium Tc 99m hexamethylpropyleneamine oxime (HMPAO).
METHODS: Twenty-seven patients underwent the balloon occlusion test. After occlusion of the internal carotid artery was performed by a balloon catheter, technetium Tc 99m HMPAO was injected, and then the balloon remained inflated for 15 minutes. The stump pressure was continuously monitored for those 15 minutes. After the balloon catheter was deflated and removed, SPECT was performed. Sixty-four symmetric pairs of regions of interest were set on both sides of the cerebral hemisphere. The radioactivity count ratio (L/n ratio) of the occluded side to the contralateral normal side was calculated. We defined hypoperfusion as an area with an L/n ratio <0.8. The minimun mean stump pressure (minMSP) during the balloon occlusion test and the pressure ratio of the minMSP to the mean systemic pressure were compared with the hypoperfusion area on SPECT.
RESULTS: The number of regions of interest with hypoperfusion was significantly (P < .001) greater in patients with a minMSP <40 mm Hg (mean [±SD] = 31.5 ± 13.7) than in patients with a minMSP ≥40 mm Hg (5.1 ± 4.0). The number of regions of interest with hypoperfusion was also significantly (P < .001) greater in patients with a pressure ratio <0.5 (26.7 ± 15.8) than in patients with a pressure ratio ≥0.5 (4.5 ± 3.5).
CONCLUSION: The minMSP during the balloon test occlusion reflects the extent of the hypoperfused area measured by SPECT using technetium Tc 99m HMPAO.
Occlusion of the internal carotid artery is often necessary to treat inoperable internal carotid aneurysms, stenotic or ulcerative carotid disease, and tumors invading the internal carotid artery (1–3). The balloon occlusion test of the internal carotid artery has been used to predict whether a patient can tolerate temporary or permanent occlusion of the internal carotid artery. Previous reports have proposed various techniques to predict the likelihood of ischemia following occlusion of the internal carotid artery, such as dynamic CT (4), measurement of cerebral blood flow, measurement of stump pressure, monitoring of somatosensory-evoked potentials (5), Doppler analysis (6), and perfusion MR imaging (7).
Measurement of cerebral blood flow has been performed by the intracarotid xenon-133 method (8, 9), stable xenon CT (10–16), single-photon emission CT (SPECT) (17–26), and positron emission tomography (PET) (27, 28). Measuring blood pressure (stump pressure) through the angiographic catheter in the distal internal carotid artery during occlusion of the internal carotid artery has also been reported as a safety index with which to predict ischemia following permanent occlusion of the internal carotid artery. In the present study, we compared the stump pressure during occlusion of the internal carotid artery with SPECT using technetium Tc 99m hexamethylpropyleneamine oxime (HMPAO).
Methods
Twenty-seven patients (13 men; 14 women; mean age, 60.7 years; age range, 19–75 years) underwent a balloon occlusion test following diagnostic cerebral angiography. Their clinical diagnoses comprised aneurysm of the internal carotid artery (n = 8), carcinoma of the thyroid gland (n = 2), meningioma of the skull base (n = 4), carcinoma of the hypopharynx (n = 4), carcinoma of the oropharynx (n = 1), carcinoma of the oral cavity (n = 3), tumor of the parotid gland (n = 2), giant cell tumor of the skull base (n = 1), lymph node metastasis (n = 1), and carotid body tumor (n = 1). All patients required treatment by internal carotid artery occlusion. Informed consent for the balloon occlusion test was obtained from all patients. No patient had neurologic abnormalities or abnormal findings on brain CT or MR imaging. Symptomatic patients during the initial occlusion of the internal carotid artery following diagnostic angiography were excluded.
After diagnostic cerebral angiography was first performed using a 5F catheter, a 5F or 7F double-lumen balloon catheter was placed into the internal carotid artery of the affected side. One lumen is used for inflation of the balloon, and the second lumen is a distal lumen beyond the balloon connecting to a pressure transducer and pressure monitor. Another 5F catheter was introduced into the common carotid artery of the affected side. After the balloon was inflated, the patient was neurologically examined for several minutes, and the balloon catheter was deflated. The balloon catheter was then inflated again, and angiography of the internal carotid artery of the normal side (n = 21) and vertebral artery (n = 13) was performed to evaluate the circle of Willis. To prevent embolic events during inflation of the balloon, we intermittently infused saline with heparin through the distal lumen beyond the balloon and through the catheter placed in the proximal common carotid artery.
Because technetium Tc 99m HMPAO cannot be injected in the angiographic suite by law, the patient was transported to the nuclear medicine department with the balloon deflated. Reocclusion of the internal carotid artery was performed under fluoroscopy. An intravenous injection of 740 MBq of technetium Tc 99m HMPAO was administered a few minutes after occlusion, and then the balloon remained inflated for 15 minutes. The stump pressure was continuously monitored for these 15 minutes. Systemic brachial blood pressure was also monitored using an automatic sphygmomanometer at 3-minute intervals. The balloon catheter was deflated and removed. SPECT was performed using a triple-head gamma camera (Multispect3, Siemens Medical Systems, Erlangen, Germany) equipped with fanbeam collimators. Data were acquired by 120 views and reconstructed using a Butterworth filter. Attenuation correction was performed by Chang’s method. The reconstructed section thickness was 4.9 mm for the transverse planes.
Sixty-four symmetric pairs of regions of interest were set manually on both sides of the cerebral surface including the cortices, lentiform nuclei, and thalami. Each region of interest was round and 10-mm in diameter. The radioactivity count ratio of the occluded side to the contralateral normal side was calculated and defined as L/n ratio. In the present study, we defined hypoperfusion as an area with an L/n ratio <0.8. The minimum mean stump pressure (minMSP) during the balloon occlusion test and the pressure ratio of the minMSP to the mean systemic pressure (measured at the same time as the minMSP) were compared with hypoperfusion areas on SPECT. The relationship between mean L/n ratio and minMSP was also compared.
Results
In total, the minMSP during occlusion of the internal carotid artery ranged from 21 to 86 mm Hg with a mean (±SD) of 47.3 ± 17.2. The L/n ratio ranged from 0.54 to 1.41 with a mean of 0.93 ± 0.16. Angiographic evidence of cross-filling through the circle of Willis was shown via the anterior communicating artery in 21 of 23 patients and via the posterior communicating artery in 12 of 15 patients. The minMSP in 5 patients without angiographic evidence of cross-filling via the anterior communicating artery or the posterior communicating artery (42.0 mmHg in average) was lower than that in the other patients (48.5 mm Hg in average); however, there was no significant difference between them.
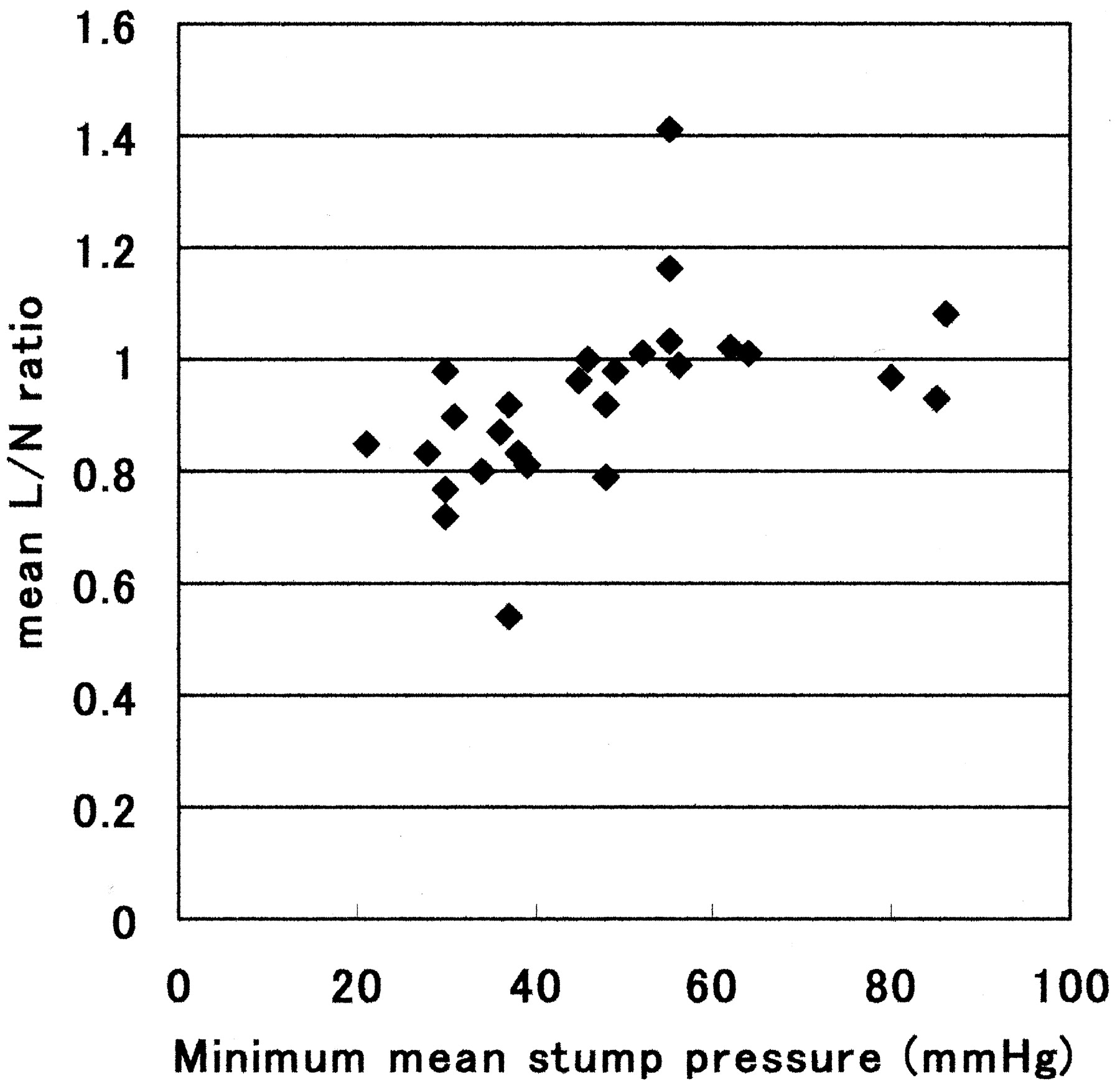
The relationship between the number of regions of interest with hypoperfusion and minMSP is shown in Fig 1. There was a significant correlation between them (P < .005 by Spearman rank correlation). The number of regions of interest with hypoperfusion was significantly (P < .001 by the Mann-Whitney U test) greater in patients with a minMSP <40 mm Hg (mean = 31.5 ± 13.7) than in patients with a minMSP ≥40 mm Hg (5.1 ± 4.0) (Figs 2, 3, 4). If the cut-off value of the minMSP is set at 50 mm Hg, the P value is 0.0024. The relationship between the number of regions of interest with hypoperfusion and the pressure ratio of minMSP to the mean systemic pressure is shown in Fig 5. The number of regions of interest with hypoperfusion was significantly (P < .001 by the Mann-Whitney U test) greater in patients with a pressure ratio <0.5 (26.7 ± 15.8) than in patients with a pressure ratio ≥0.5 (4.5 ± 3.5) (Fig 6). If the cut-off value of the pressure ratio is 0.4 or 0.6, the P value is 0.0019 or 0.0409, respectively. Figure 7 shows a significant positive relationship between mean L/n ratio and minMSP (linear regression analysis; y = mean L/n ratio, x = minMSP; y = 0.71 + 0.005x; r = 0.497, P = .0084).

Graph shows the relationship between the minimum mean stump pressure and number of regions of interest (ROIs) with hypoperfusion. There was a significant correlation (P < .005 by Spearman rank correlation).

Graph shows that the number of regions of interest (ROIs) with hypoperfusion was significantly (P < .001 by Mann–Whitney U test) greater in patients with a minMSP <40 mm Hg (31.5 ± 13.7) than in patients with minMSP ≥40 mm Hg (5.1 ± 4.0).

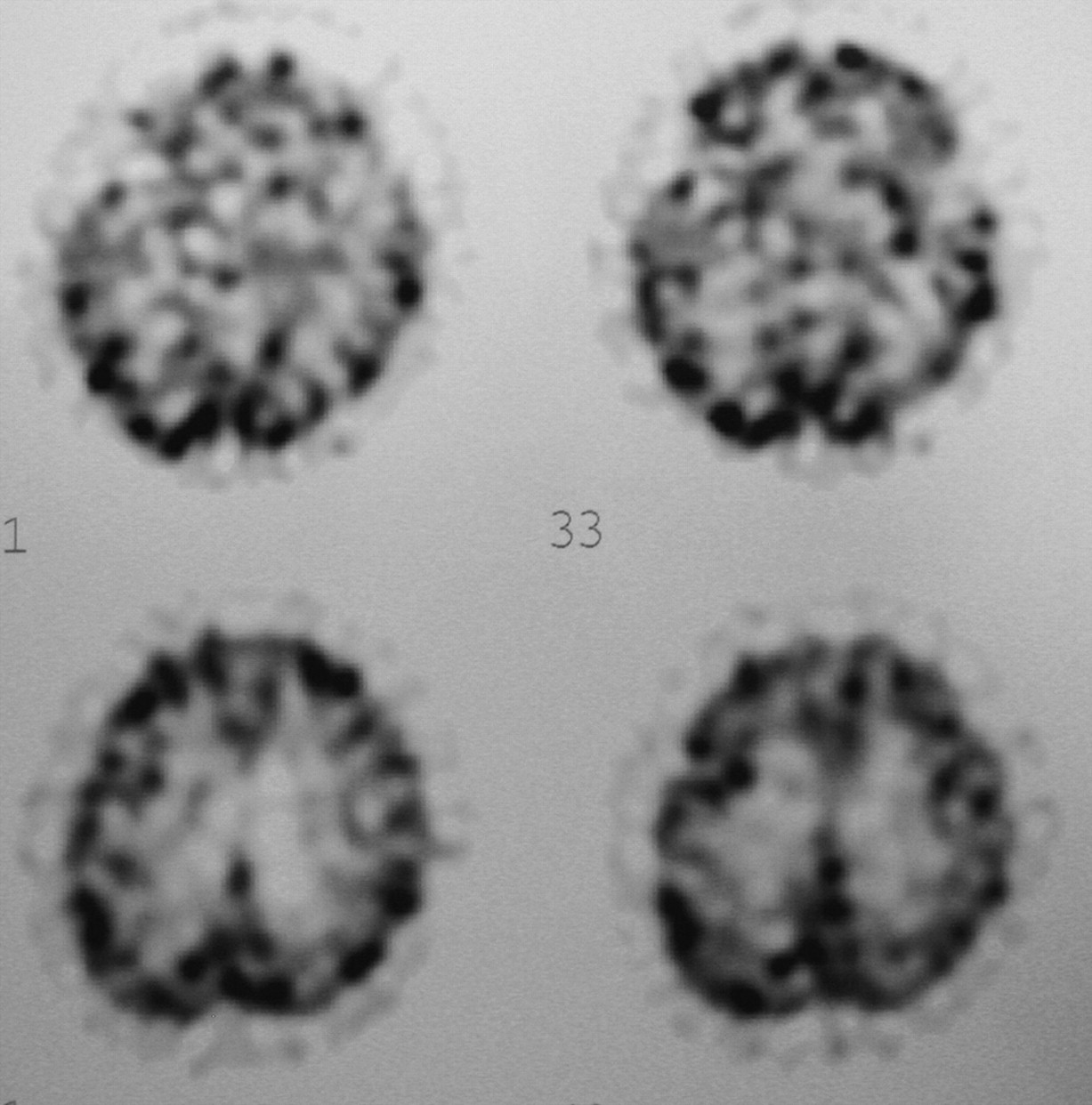
In a 73-year-old man with hypopharyngeal carcinoma on the left side, the minMSP was 30 mm Hg during balloon test occlusion of the left internal carotid artery. SPECT using technetium Tc 99m HMPAO showed hypoperfusion of the cerebral hemisphere on the left side.

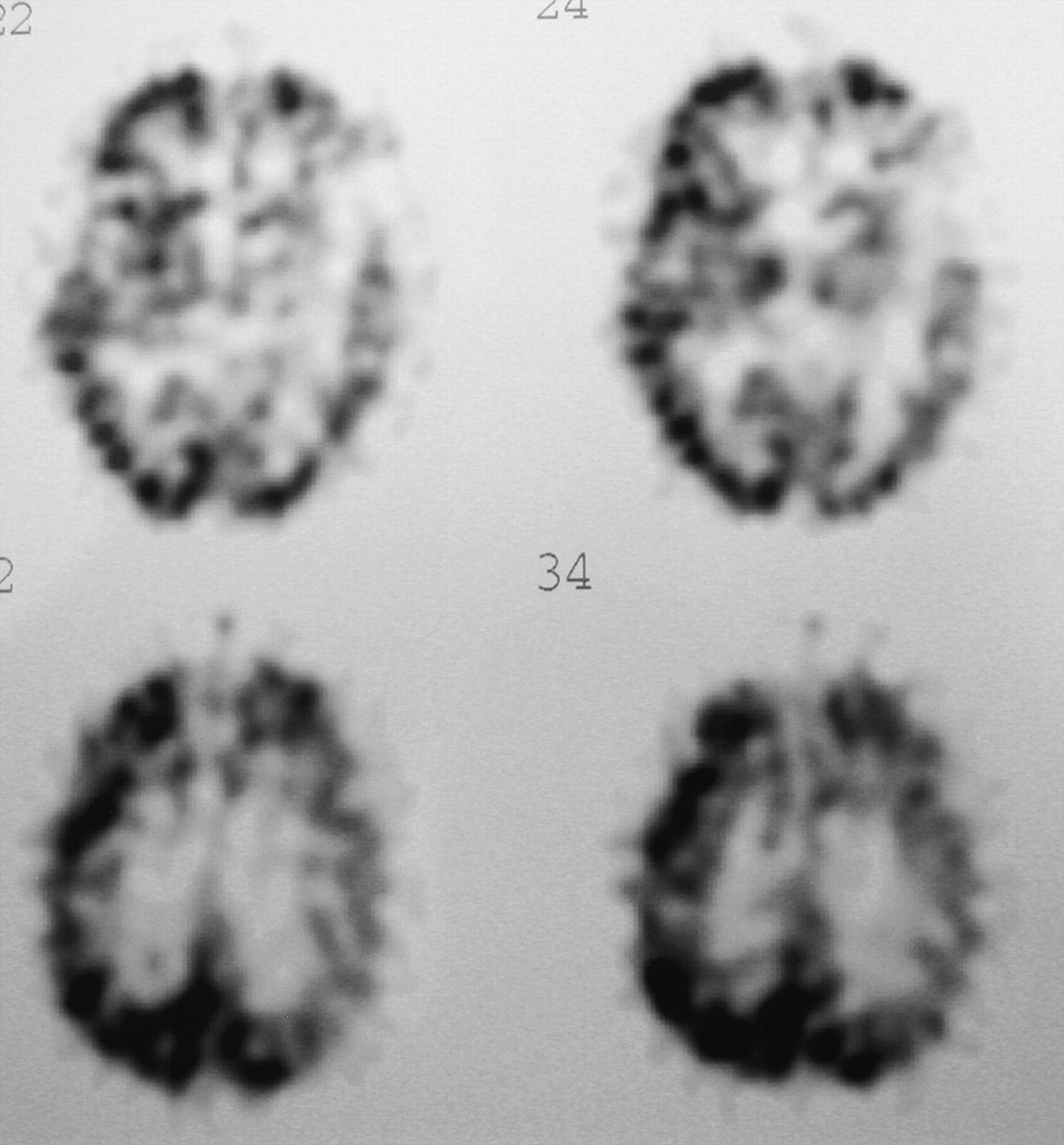
In a 64-year-old man with meningioma invading the left internal carotid artery, the MSP was 64 mm Hg during balloon test occlusion of the left internal carotid artery. SPECT using technetium Tc 99m HMPAO showed no hypoperfusion areas of the cerebral hemisphere on the left side.

Graph shows the relationship between the number of regions of interest (ROIs) with hypoperfusion and the pressure ratio of the minMSP to the minimum mean systemic pressure.

Graph shows that the number of regions of interest (ROIs) with hypoperfusion was significantly (P < .001 by Mann–Whitney U test) greater in patients with a pressure ratio <0.5 (26.7 ± 15.8) than in patients with a pressure ratio ≥0.5 (4.5 ± 3.5)
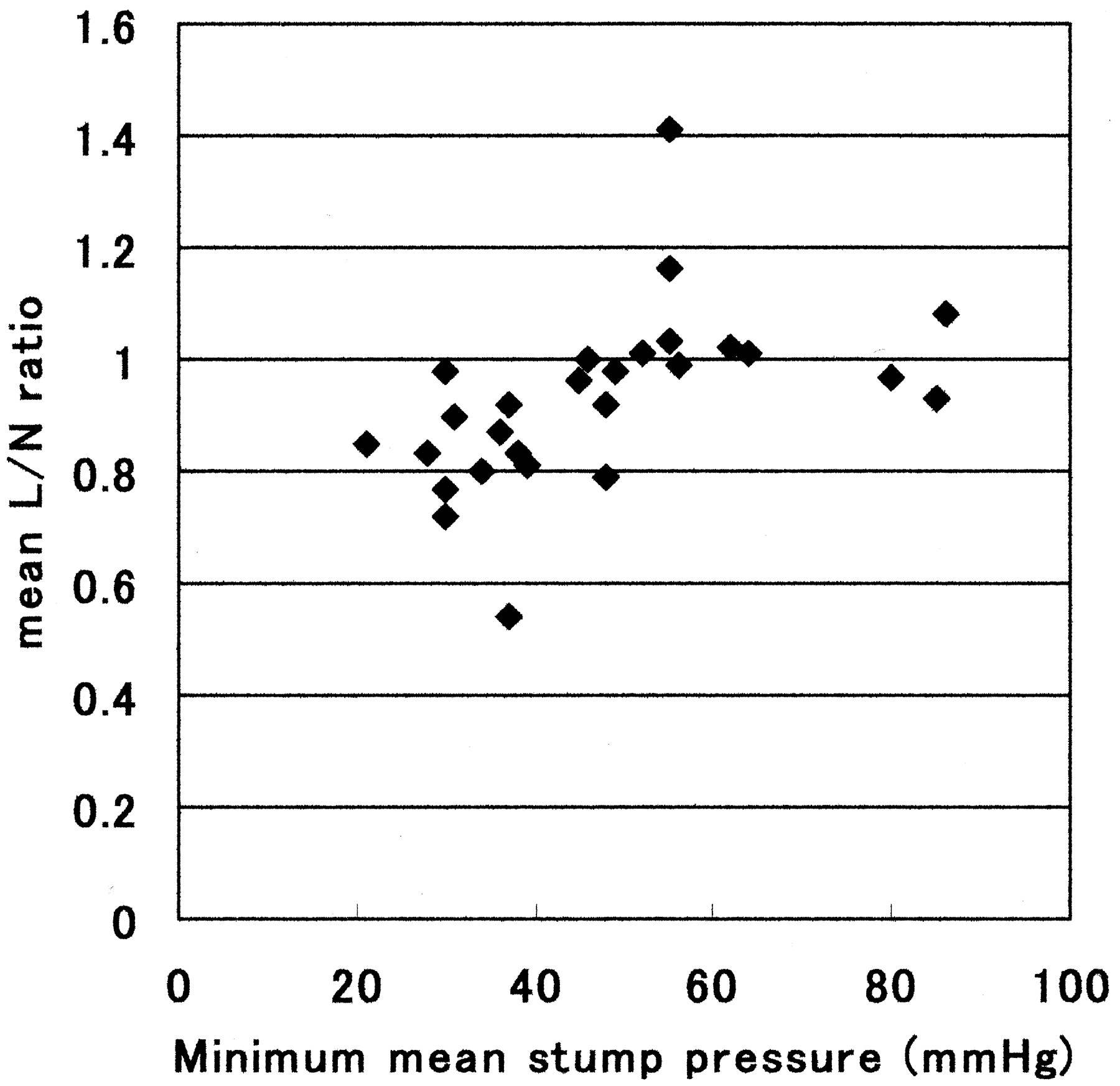
Graph shows the relationship between the minMSP and the mean L/n ratio (the radioactivity count of the occluded side / the radioactivity count of the contralateral normal side). There was a significant positive relationship (linear regression analysis; y = mean L/n ratio, x = minMSP; y = 0.71 + 0.005x; r = 0.497, P = .0084).
There were 6 patients who showed a gradual decrease of MSP after occlusion. The number of regions of interest with hypoperfusion in these 6 patients (25.5 ± 21.9) was not significantly greater than that in other patients (14.4 ± 13.7). However, 4 of these 6 patients showed a minMSP <40 mm Hg.
In 5 of 14 patients who underwent surgery, ligation of the internal carotid artery with bypass surgery (n = 2) and transient occlusion of internal carotid artery (n = 12) were performed. Infarction appeared in 1 of 2 patients who underwent ligation of the internal carotid artery after bypass surgery between the middle cerebral artery and common carotid artery. In that patient, the MSP during the balloon test occlusion was 38 mm Hg, and 28 regions of interest had hypoperfusion on SPECT.
Discussion
Patients with aneurysms of the internal carotid artery or tumors invading the internal carotid artery at the neck or base of the skull often require permanent sacrifice or transient occlusion of the internal carotid artery. SPECT has been widely available for evaluating cerebral blood flow, and the use of SPECT for the balloon test occlusion has been reported (17–26). Technetium Tc 99m HMPAO is converted to a hydrophilic compound and remains fixed in the brain (10). The brain activities of technetium Tc 99m HMPAO reflect cerebral blood flow within a few minutes after injection. In the present study, the balloon remained inflated for 15 minutes after injection, which is long enough to evaluate cerebral blood flow. On the other hand, measuring the stump pressure during the balloon test occlusion is easy to perform.
Several authors have reported the relationship between stump pressure and cerebral blood flow during the balloon test occlusion (17, 21–23, 26). Kurata et al (22) and Morishima et al (23) reported that the mean ratios of the initial MSP to the preocclusion mean arterial pressure of 60% is useful as an index of symmetrical cerebral blood flow on SPECT using technetium Tc 99m HMPAO. As they reported, the MSP has a tendency to fall immediately after occlusion. This was also indicated by Baker et al (10), who compared the change in MSP during the balloon test occlusion with cerebral blood flow measured by stable xenon CT. However, they reported that the MSP often gradually increased after occlusion.
In the present study, 6 patients showed a gradual decrease of MSP after occlusion. Previous studies used the average of MSP, the initial MSP, or the final MSP during the balloon occlusion test. We used the minMSP during the balloon test occlusion because the minMSP during the balloon occlusion test might be closely related to the risk of ischemia. The minMSP could be found by monitoring stump pressure throughout the 15-minute period. The minMSP did not often occur initially or finally after occlusion. The usefulness of systolic or diastolic stump pressure should be further studied. We compared the ratio of the minMSP to the mean systemic pressure measured at the same time as the minMSP with hypoperfusion areas on SPECT and found that a pressure ratio of more than 50% was a useful index of symmetrical cerebral blood flow.
We excluded symptomatic patients following initial occlusion of the internal carotid artery. If symptomatic patients undergo sacrifice of the internal carotid artery, they then require bypass graft or anastomosis surgery to supply blood flow to the distal portion of the internal carotid artery without brief occlusion of the internal carotid artery.
Okudaira et al (14) measured MSP and cerebral blood flow using stable xenon CT during balloon test occlusion with and without acetazolamide activation and found a significant correlation between the increase in cerebral blood flow caused by acetazolamide and MSP. They also found no cerebral blood flow increase when MSP was <40 mmHg, and they noted that 40 mmHg appeared to be the lower autoregulatory limit. Although the methodology of their investigation was quite different from ours, it is interesting that the lower threshold of MSP during occlusion of the ICA was the same as that in the present study. In the present study, we defined hypoperfusion as an area with an L/n ratio <0.8. Although this value of the ratio is controversial, in previous reports concerning the balloon test occlusion, most authors qualitatively evaluated technetium Tc 99m HMPAO as an indicator of ischemic change.
Knudsen et al (17) performed SPECT using technetium Tc 99m HMPAO during carotid cross-clamping and found correlation between the stump pressure and asymmetry in the middle cerebral arterial territory semiquantitatively calculated by SPECT. Although they did not clearly define the lower threshold of the stump pressure, the figure in their report suggested that cases with a stump pressure <40 mm Hg had hemispheric asymmetry of more than 10%. A change in asymmetry with carotid clumping exceeding 10% is significant (17, 25).
Sugawara et al (25) reported the usefulness of SPECT using technetium Tc 99m ethylcysteinate dimmer during the balloon test occlusion, and their criterion for moderate or severe hypoperfusion was an L/n ratio of <0.9. The definition of hypoperfusion in the present study, an L/n ratio <0.8, is more rigid, though the semiquantitative evaluation of technetium Tc 99m HMPAO applied in the present study is simple and does not yield an absolute cerebral blood flow value. Evaluation of absolute cerebral blood flow value by other methods such as 133Xe-SPECT, Iodine-123 iodoamphetamine-SPECT, and H215O-PET might produce more accurate results.
Angiographic evaluation of the circle of Willis appears necessary for the collateral circulation; however, it cannot measure the collateral blood flow quantitatively. The stump pressure during occlusion of the internal carotid artery may quantitatively reflect the degree of collateral flow via the circle of Willis. In the present study, the minMSP in 5 patients without angiographic evidence of cross-filling via the anterior communicating artery or posterior communicating artery (42.0 mm Hg on average) was lower than that in the other patients (48.5 mm Hg on average).
Whether measuring stump pressure can be omitted by performing SPECT remains controversial. Although stump pressure cannot yield the location of risk for hypoperfusion, SPECT can give us the location of hypoperfused areas during the balloon test occlusion. It may not actually be necessary to measure stump pressure during balloon test occlusion when SPECT can be performed. However, the results of the present study would be useful at surgery because only stump pressure can be used as an index to predict ischemia when a transient occlusion is performed at surgery. In addition, stump pressure should be monitored in patients whose SPECT does not show significant hypoperfusion before surgery. This study is still preliminary and should be performed in a greater number of patients.
Conclusion
Patients with a minMSP of ≥40 mm Hg and patients with a pressure ratio of ≥0.5 show relatively symmetric cerebral perfusion on SPECT using technetium Tc 99m HMPAO during the balloon test occlusion. The minMSP during the balloon test occlusion reflects the extent of the hypoperfused area measured by SPECT using technetium Tc 99m HMPAO.
References
- Received December 19, 2004.
- Accepted after revision March 27, 2005.
- Copyright © American Society of Neuroradiology
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.