
Abstract
BACKGROUND AND PURPOSE: Dissection and retraction of the sylvian fissure can cause venous insufficiency and may be an important contributor to postoperative edema or hemorrhage after clipping of a middle cerebral artery (MCA) aneurysm. The incidence of changes in the superficial middle cerebral vein (SMCV) and adjacent veins and whether such changes increase the amount of edema or hemorrhage on postoperative CT is the focus of this study.
METHODS: Pre- and postoperative angiograms of 100 consecutive patients with MCA aneurysms treated by craniotomy and clipping were compared to determine the postoperative incidence of changes involving the SMCV. CTs from the normal and abnormal postoperative venous groups were compared to determine the amount of edema or presence of parenchymal hemorrhage.
RESULTS: Postoperatively, 31 (31%) SMCVs were altered, 20 to a minor or moderate degree. Eleven cases were pronounced. In 9 (9%) cases, the SMCV was completely obscured or failed to fill on postoperative angiography. More edema (observer 1, P < .0002; observer 2, P < .0006) and small brain parenchymal hemorrhages (observer 1, P < .00003; observer 2, P < .00001) were found on the postoperative CT images of the group whose SMCVs were altered than those that were unchanged.
CONCLUSIONS: Neurosurgeons and neuroradiologists should be attentive to changes in the SMCV and adjacent venous structures to optimize outcomes of procedures involving the sylvian fissure.
The neurosurgical approaches most commonly used to access supratentorial, deep intracranial structures are the pterional and orbitozygomatic approaches. With careful retraction to separate the frontal and temporal lobes, these approaches may be used to clip middle cerebral artery (MCA) aneurysms. To increase anterior exposure, the pterional approach can be extended to an orbitozygomatic approach. Despite careful surgical dissection, placement of retractors, and separation of brain structures, more superficial venous structures may be compromised.
We have observed significant areas of edema in the region of the sylvian fissure in some patients who have undergone clipping of MCA aneurysms, even when their arterial structures were intact, vasospasm did not occur, and retractors had been placed carefully. Compared with their preoperative examination, these patients’ venous structures exhibited local changes on postoperative angiograms. We suspected that changes in venous drainage may have contributed to an increase in edema and small hemorrhages around the surgical site as seen on postoperative CT imaging.
The purpose of this study was therefore 2-fold. First, we assessed the incidence of changes in venous structures around the sylvian fissure after MCA aneurysms were clipped. Second, we evaluated whether such changes significantly contributed to the edema or hemorrhages seen on postoperative CT compared with patients with intact venous pathways.
Materials and Methods
From June 1998 to December 2003, 240 consecutive patients with MCA aneurysms were treated. Of those 240 patients, 100 patients met all inclusion criteria, had no exclusion criteria, and were included in the study. Postoperative angiograms and CTs were also reviewed retrospectively. Exclusion criteria included coiling of aneurysms, intraoperative angiograms obtained in place of conventional angiograms; severe vasospasm; occluded MCA branches; large temporal, frontal, or basal ganglia hematomas; inadequate venous phase on angiograms; giant aneurysms with pre-existing brain edema; and peripheral mycotic or berry aneurysms higher in the fissure. The exclusion criteria were intended to eliminate confounding variables that could affect the amount of edema on postoperative CT or that could diminish the quality of angiograms for interpretation of venous phases.
Two staff neuroradiologists (B.D., R.W.) compared patients’ pre- and postoperative angiograms to determine the incidence of changes in the superficial middle cerebral vein (SMCV) after surgery. Only cases that both observers agreed had changed significantly were considered positive. They categorized SMCVs as small, medium, or large (Fig 1) and noted whether the veins were single, paired, or multiple. Hypoplastic SMCVs with small veins draining to other systems were classified as small. The venous phase on postoperative angiograms was used to classify abnormal SMCVs as absent, focal occlusion, or attenuated and to identify the location of the attenuation. Small branch occlusions and loss of adjacent frontal or temporal veins were also recorded. All postoperative angiograms were obtained within a week of surgery.

Assessment of superficial middle cerebral vein (SMCV) size. A, Two small paired SMCVs (arrow). B, Moderate-size single SMCV (arrow). C, Large SMCV (white arrow) and small temporal branch (black arrow) draining into larger SMCV.
Next, the frequency of hemorrhage and the amount of edema were determined on the patients’ postoperative CTs. The section level with the maximal amount of edema was selected, and 2 perpendicular measurements were obtained. The area was calculated by using the formula for the area of an ellipse (πAB/4). The 2 neuroradiologists (A.P., C.R.B.), who were blinded to the results of the angiograms, independently measured the amount of edema and noted the presence or absence of parenchymal hemorrhage. All CTs were obtained within 4 days of surgery.
The null hypothesis was that both groups (changed and intact SMCVs on angiography) would have similar amounts of edema or hemorrhage on their postoperative CT scans. The alternate hypothesis was that altered or absent SMCVs would be associated with an increase in the amount of edema or hemorrhage on their postoperative CTs. The cross-sectional area of edema, a continuous variable, was compared in the group with an intact SMCV to that of patients whose SMCV had changed by a 1-tailed t test with unequal variance. The presence or absence of hemorrhage, a nominal variable, was compared between the 2 groups by a 1-tailed, 2 × 2, Fisher exact test.
Results
Compared with their preoperative angiogram, the SMCV was altered on the postoperative angiograms of 31 patients (31%). Nine SMCVs (2 large, 5 moderate, and 2 small) were absent or obscured (Fig 2). Postoperatively, 2 SMCVs partially failed to fill though portions of the vein were present. In 7 cases, the SMCV was predominantly intact with a focal area of occlusion, high-grade stenosis (Fig 3), or longer segment of attenuation (Fig 4). The 13 least-affected SMCVs were small and showed mild or moderate regions of attenuation, or small branches of the SMCV were occluded.

Large SMCV with distal occlusion. A, Three large branches with smaller branches join to form the SMCV. B, Mid and distal portions of the SMCV do not fill (arrow).

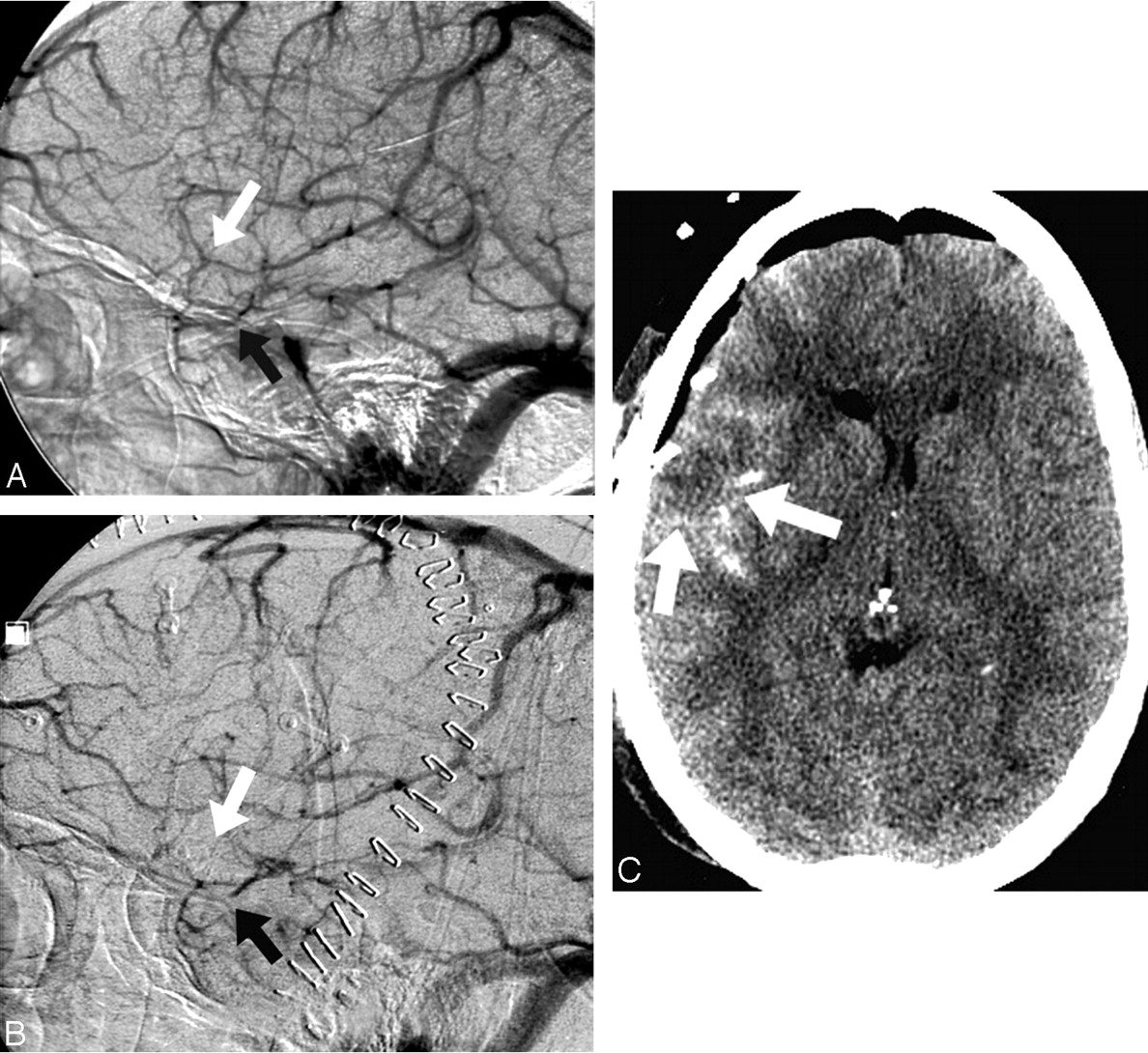
Focal attenuation of SMCV. A, Large single SMCV. B, Focal attenuation of midportion of SMCV (arrow). The entire extent of the vein fills.

Small SMCV occlusion. A, Unequal-sized and paired branches form a small SMCV. B, Almost the entire extent of the SMCV is obscured or fails to fill (arrow).
Of the 100 postoperative CT scans, 47 showed significant regions of edema in the frontal and temporal lobes in the region of the sylvian fissure as recognized by at least one observer. Twenty-four of those 47 with edema demonstrated postoperative alteration of the SMCV. Twenty-three of the patients with postoperative edema on the CT scans had intact SMCVs. Therefore, 77% of cases with altered SMCVs displayed edema, and only 33% with intact SMCVs displayed edema on the postoperative CTs. The area of edema was also usually smaller, if the veins were intact. The mean area of edema on the CT scans of the patients whose SMCV had changed was 5.22 cm2 according to observer 1 and 4.05 cm2 according to observer 2. In the group whose SMCV was unchanged, the mean area of edema was 1.28 cm2 according to observer 1 (P < .0002) and a mean of 1.00 cm2 according to observer 2 (P < .0006). Thus, the hypothesis that changes in the SMCV after surgery are associated with an increased amount of edema on postoperative CT was supported.
The severity of postoperative changes to the SMCV correlated with the amount of edema on postoperative CT scans. Severely affected veins were present in 11 cases, with a mean area of edema of 10.8 cm2. The veins were absent or predominantly nonfilling. Seven postoperative SMCVs had moderate changes with focal or diffuse areas of attenuation, but predominantly filled. The moderately affected SMCVs had a mean region of edema of 5.2 cm2. The least-affected veins had a mean area of edema of 1.8 cm2. Those 13 cases had regions of mild attenuation or small branch occlusions.
In both groups, all postoperative hemorrhages were small or involved minimal areas of hemorrhagic staining. Observer 1 noted 12 small hemorrhages in the patients with altered SMCVs and 3 in patients with intact SMCV (P < .00003). Observer 2 noted 9 small hemorrhages in the former and none in the latter (P < .00001).
Discussion
During conventional neurosurgical and endovascular procedures, both arterial and venous structures need to be preserved (1, 2). Even when retractors are placed with care during a pterional or orbitozygomatic craniotomy, splitting the fissure and microsurgical dissection expose adjacent venous structures to the risks of injury or occlusion. The vessels most susceptible to such injuries are the SMCV and bridging cortical veins (Fig 5). The deep middle cerebral vein and adjacent inferior frontal bridging veins are also vulnerable. The most easily recognized and consistently present vein in the region identified by angiography is the SMCV.

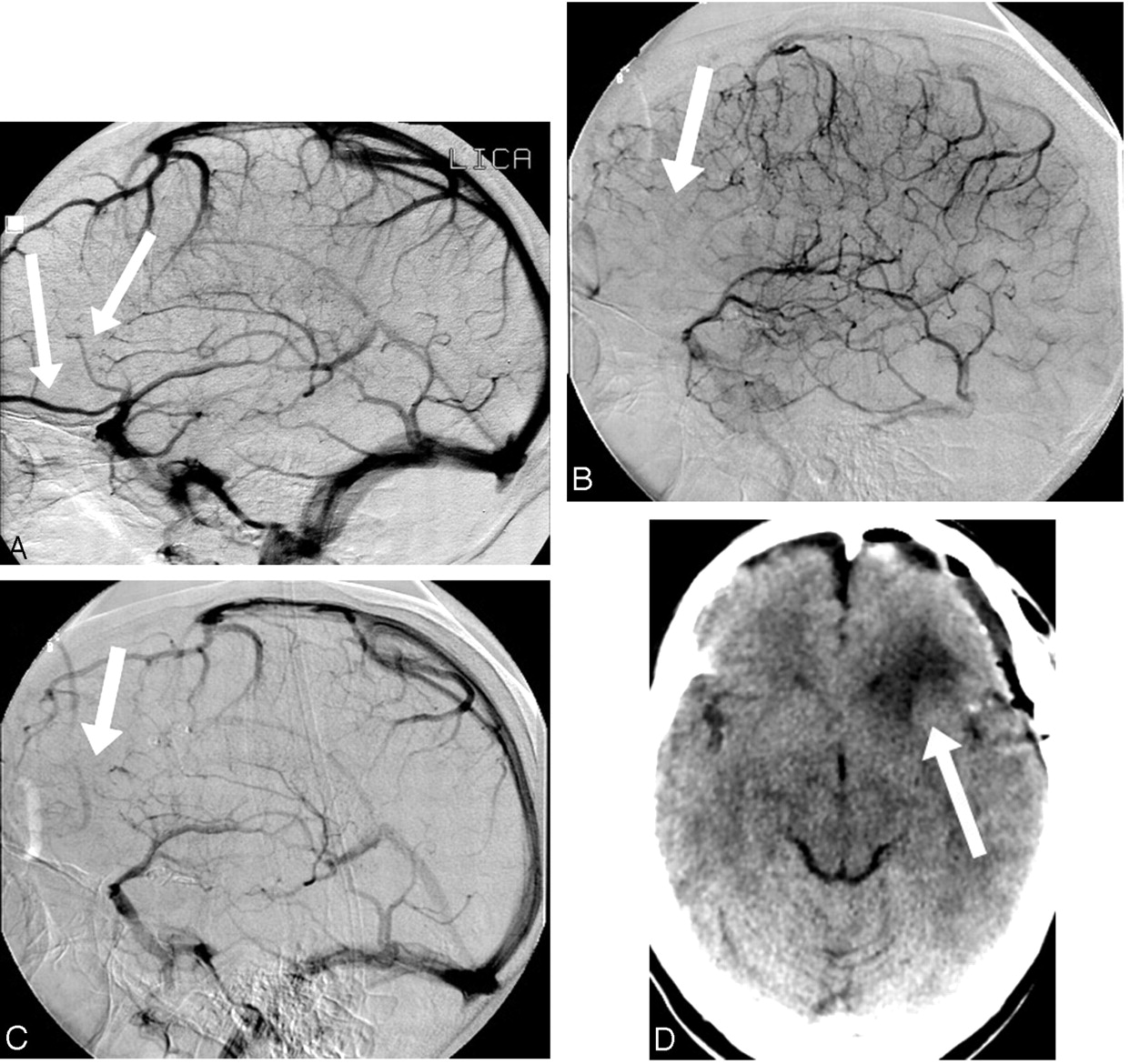
Occlusion/nonfilling of frontal lobe veins. A, Multiple large branches from the frontal (arrows) and temporal lobes coalesce to form a large SMCV trunk. B, Early venous phase shows no filling of veins and oligemic region of brain (arrow). C, During the late venous phase, the cortical veins (arrow) of the frontal lobe also fail to fill. D, CT scan shows deep frontal lobe and subcortical white matter edema. The attenuation of the cortical gray matter appears to be normal. The arterial structures are intact.
The venous drainage pattern of the sylvian fissure varies tremendously (3–6). Typically, the SMCV drains anteriorly and caudally (distal portion near skull base) along the fissure toward the skull base. It then turns medially and courses along one of several possibilities. It may join the anterior portion of the cavernous sinus. It may envelop in the lateral wall of the cavernous sinus between the layers of dura and exit via the superior petrosal sinus or an emissary foramen. It may drain independently through its own emissary or basal foramen. It may join the sphenoparietal sinus near its junction with the cavernous sinus. Occasionally, it joins the basal vein of Rosenthal in conjunction with the deep middle cerebral vein. The SMCV also may drain directly posteriorly at the level of the skull base to the superior petrosal sinus or transverse sinus adjacent to the tentorium. The SMCV may be hypoplastic or vary in size. It may drain to adjacent cortical veins over the frontal lobe, Trolard plexus, or vein of Labbé and, hence, anteriorly, superiorly, or posteriorly on the surface of the brain.
Although their conclusion is not espoused by most neurosurgeons, Kageyama et al (7) previously suggested in their insightful study that venous occlusion is the single most important factor contributing to morbidity in patients undergoing the pterional approach for aneurysm surgery. In their series, the SMCV was the most important and superseded all other causes of morbidity. Of their 100 consecutive patients, 24 had “obscuration” of the SMCV; however, occlusions of the frontal bridging veins also occurred. Most edema was noted in the frontal lobes. They concluded that venous ischemia was a more significant cause of morbidity than retractors, vasospasm, or arterial infarcts, which highlights the importance of preserving veins during aneurysm surgery.
In only 9 of our cases (9%) were the veins completely obscured or unable to be visualized; 2 of these veins were small, 5 were moderate, and 2 were large before surgery. A significant part of the vein failed to fill in another 2 (2%) of our cases, but portions of the SMCV remained. Minor or moderate changes to the vein were present in another 20 cases, but most of the veins were clearly visible. The minor changes and most moderate changes to the SMCV likely did not contribute to adverse clinical outcomes, though edema was present in some cases (Fig 6).
Occluded and very small SMCV and small temporal branch are associated with a small region of brain edema. A, Very small SMCV (white arrow); temporal branch (black arrow). B, Nonfilling of tiny SMCV (white arrow) and distal occlusion of temporal branch (black arrow). C, Small temporal lobe region of edema appears to correlate well with small vessel occlusions (arrows).
Several factors may account for the marked differences between these 2 series. Differences in surgical techniques or improvement in microsurgical techniques in the 12-year interval between studies likely plays a key role. The elimination of confounding variables and scrupulous attention to angiographic technical issues in the present study are also probably involved. Absence of MCA branches or severe vasospasm can cause faint and subtle filling of the SMCV or marked delays in the filling of venous structures, which could be mistaken for nonfilling of the vein.
Postoperative edema on imaging studies after a craniotomy for aneurysm clipping may be attributed to a variety of causes. Brain edema after a pterional approach for MCA aneurysm clipping may be related to MCA branch occlusions, severe vasospasm, use of retractors, venous infarcts and ischemia, brain parenchymal hemorrhages with aneurysm rupture, emboli from aneurysms, temporary surgical occlusion of vessels, and mass effect on the brain by giant aneurysms.
The exclusion criteria were intended to limit the variables that could affect the amount of edema on postoperative CT. Brain retraction was used in all patients. All patients underwent surgery soon after their initial subarachnoid hemorrhage, and most CTs were obtained either the day of or day after surgery, which would minimize the potential effect of vasospasm. Cases with significant vasospasm on subsequent angiograms were excluded from the study.
Brain parenchymal edema is usually a manifestation of brain injury. Venous infarcts are frequently associated with both edema and hemorrhage but may not necessarily be associated with complications similar to those associated with arterial infarcts. Long-term studies (8) evaluating the clinical effect on patients with presumed moderate or large areas of venous ischemia after SMCV injury and nonvisualization on postoperative angiograms are limited.
Studies of cerebrovenous occlusive disease usually pertain to dural sinus thrombosis (9–11). Reports and studies isolated to cortical vein thrombosis are far less common (12); however, the underlying pathophysiologic changes that cause the brain alterations are similarly caused by elevated venous pressures. The basic pathophysiologic changes are not clear, but they appear to entail elevated pressures that may stimulate either an increase or decrease in cerebral blood flow (CBF) depending on the severity and duration of elevated venous pressures. With more severe involvement, there may be alteration of the blood-brain barrier and accumulation of interstitial fluid causing vasogenic edema. Accompanying reductions in regional CBF may also cause cytotoxic edema with mixed diffusion scans with both restricted diffusion and increased diffusion regions. Diffusion scans may also display only restricted components or increased components of diffusion, whichever is dominant (9, 10). MR imaging features of venous ischemia or pressure elevation initially display regional mass effect. Hyperintense signal intensity on T2-weighted sequences may involve either white or gray matter or both in approximately 50%–60% of cases and parenchymal hematomas in 30%–40% (10).
Longer-term imaging and clinical-follow up of cases are limited. Persistent MR findings include regional mass effect as long as 2 years after clinical onset (11), hemosiderin staining, hyperintensity on T2-weighted sequences, volume loss, and evidence of prior infarction. In general, venous injuries have less dire outcomes than do equal-size arterial injuries or hemorrhages. Mullins et al (10) were able to classify 3 clinical outcome groups by MR and clinical criteria: (1) cases with restricted diffusion and without seizures had persistent hyperintense regions on longer-term follow-up T2-weighted sequences and had worse clinical outcomes; (2) cases with restricted diffusion and with seizures resolved their imaging abnormalities and had better clinical outcomes; and (3) a larger number of cases had increased diffusion (vasogenic edema), which resolved and had better outcomes.
Animal laboratory studies and human intraoperative studies have documented the importance of preserving veins. During surgery, Kanno et al (13) demonstrated temporary reduction in regional blood flow and nerve action potentials in humans with temporary cortical venous occlusions following the application of surgical clips. Kasama and Kanno (14) tested the effects of cortical venous occlusion and prolonged use of retractors in dogs and monkeys. When cortical veins were ligated in the region of the brain where retractors were used, the incidence of subcortical hematomas was 60%. By contrast, only 13% of the animals developed hematomas with the prolonged use of retractors alone.
Aneurysms are increasingly treated with endovascular coils, which may decrease the number of pterional craniotomies performed and thereby the risk of injury to venous structures; however, for MCA aneurysms, which are frequently complex with branches arising from the walls, surgery will likely remain the primary treatment. The risk of injury to the SMCV is also pertinent when a pterional craniotomy is performed and the sylvian fissure is split to access deep portions of the brain. The results of this study are applicable to other procedures involving this region (15) because the risk to the SMCV is similar. Hence, preservation of the SMCV and adjacent venous structures will remain a relevant topic.
Our study indicates a high degree of correlation (observer 1, P < .0002; observer 2, P < .0006) between changes in the SMCV after the surgical treatment of MCA aneurysms and underlying edema in the brain and small hemorrhages (observer 1, P < .0003; observer 2, P < .00001, respectively). Presumably, these findings also correlate with brain injury. Both radiologists and neurosurgeons must strive to detect and decrease the incidence of this outcome.
Angiograms may show anatomic variations of SMCVs that may predispose, or alternatively, lessen the risk of injury during surgery (16–18). Intraoperative angiograms are often obtained during this type of procedure because of the complexity of the MCA. When used, intraoperative angiography should include a lateral view when possible with a venous phase to document patency of the SMCV after the aneurysm is clipped. This portion of the study is often overlooked. In general, postoperative venous injuries or changes compared with a patient’s preoperative status are under-reported. SMCVs also may have pre-existing large collateral branches that may decrease the risk of venous infarction (Fig 7) and could therefore alter the course of surgery.

Distal occlusion of large SMCV. Brain is protected by collateral branch. A, A large collateral branch is connected to the vein of Labbé (small black arrows). Distal SMCV is depicted by white arrow. B, Occlusion of veins distally (white arrow) is protected by collaterals (black arrows). C, Postoperative CT scan is unremarkable, without significant brain edema or hemorrhage.
With retraction, dissection, and movement of the brain, anatomic variations may predispose venous structures to injury with less opportunity to mobilize the brain when the SMCV is affixed along the dura or anastomotic sites or emissary foramina. CT angiography and venography have helped to identify venous variations or anomalies (19) that may complicate surgeries in the region of the fissure. Preoperative identification of large veins around the margins of aneurysms or in the surgical field of other targeted surgical masses or lesions may improve the likelihood of their being preserved.
Neurosurgeons may modify their procedures to reduce the risk of traction of venous structures associated with mobilization of the brain (20–22). Skeletonization of the draining veins may allow venous structures to better withstand movement of the brain and traction. Freeing the dura around venous attachments may safely allow further mobilization of veins and a reduction in traction.
Limitations of the Study
Our study is limited by the inherent biases associated with a retrospective study. Edema or small hemorrhages in the underlying brain usually correlate with brain injury; however, venous injuries may not have the dire consequences associated with arterial injuries. Long-term follow-up studies on the clinical relevance of venous injuries are limited. For practical purposes involving imaging, this study primarily focused on the SMCV and adjacent venous structures, which are the most easily recognized veins in the area at angiography. Injury to deeper venous structures is equally important but more difficult to detect angiographically. Hence, the extent of venous injuries was probably not fully recognized by our study. Our institution is a tertiary referral center and a large number of patients from referring centers are admitted with prior CTs. Pre-existing areas of edema or small hemorrhages are possible confounding issues for the study; however, this factor would have affected both groups equally.
Conclusions
Most changes to the SMCV after surgery for MCA aneurysm clipping are mild or moderate. Although unlikely to be clinically relevant, such changes may be more common than believed. Moderate or large veins were occluded less frequently than small veins but tended to be associated with more edema or small hemorrhages. In our series, the incidence of complete nonvisualization or obscuration of the SMCV after surgery (9%) was significantly lower than in an earlier report (24%). Changes in the SMCV and adjacent venous structures strongly correlated with the amount of edema and presence of small hemorrhages in the underlying brain on follow-up CT. Increased awareness of the risk to local venous structures caused by pterional craniotomies, splitting of the fissure, and surgical dissection is appropriate. Venous injuries are underreported. Monitoring of venous variations prospectively by CT or conventional angiography may decrease the rate of surgical complications. Intraoperative angiography should assess the patency of veins when possible and not be limited solely to examining the patency of arterial structures. Postoperative CT angiography or conventional angiography also may show venous patency and aid in clinical management.
Acknowledgments
We thank Heidi Jahnke, RN, for her work and collection of patients’ names from the data base and the Neuroscience Publications office of Barrow Neurologic Institute for their assistance in preparing the manuscript.
References
- Received December 10, 2004.
- Accepted after revision March 2, 2005.
- Copyright © American Society of Neuroradiology




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}