
Abstract
BACKGROUND AND PURPOSE: MR perfusion-weighted imaging (PWI) has been extensively used to quantify cerebral perfusion deficits after the onset of focal ischemia. The present study tested whether a relative measure of cerebral blood flow such as is obtained with PWI is sufficient to predict irreversible tissue damage following focal cerebral ischemia and reperfusion in the rat suture model.
METHODS: In rats, the middle cerebral artery was occluded (MCAO) for 1 hour followed by 1-hour reperfusion. Microspheres labeled with different tracers were injected into the left ventricle to permit measurement of blood flow at different time points: before MCAO, 30 minutes post-MCAO and 30 minutes postreperfusion. Absolute cerebral blood flow (CBF) was determined and relative CBF was calculated by comparing absolute CBF at each time point to baseline values before MCAO (relative CBFB) or to corresponding contralateral areas in the noninfarcted hemisphere (relative CBFC). Infarct size was assessed by 2,3,5-triphenyltetrazolium chloride staining.
RESULTS: Absolute CBF in vital tissue was 0.69 ± 0.07 mL/g/min. In partially and completely necrotic tissue, absolute CBF was 0.39 ± 0.05 mL/g/min and 0.30 ± 0.09 mL/g/min, respectively. Although there was a close inverse correlation between infarct volume and absolute CBF (r = 0.79), the correlations between infarct volume and relative CBFC were poor (r = 0.21).
CONCLUSION: The present study revealed that absolute CBF is superior to relative CBF in predicting irreversible tissue damage following ischemia and reperfusion.
MR perfusion-weighted imaging (PWI) has been extensively used to quantify cerebral perfusion deficits after the onset of focal ischemia (1, 2). To determine ischemic tissue at risk of potentially undergoing infarction, the literature suggests a critical flow level—expressed as percentage of that in the contralateral area in the noninfarcted hemisphere—of approximately 40%–55% (3, 4); however, controversies exist on the validity of PWI-derived blood flow ratios—ie, relative cerebral blood flow (CBF), especially in the case of reduced perfusion (5).
Experimentally, radioactive labeled microspheres permit the repeated measurement of absolute CBF even in small animals (6). The goal of the present study was to apply the microspheres technique to rats and measure absolute CBF in different cortical and subcortical areas during focal cerebral ischemia and subsequent reperfusion in an established model of endovascular middle cerebral artery occlusion (MCAO). Therefore, radioactive microspheres were directly injected into the exposed left ventricle. By comparing relative CBF with absolute CBF the present study examined whether relative CBF is as valid as absolute CBF in determining tissue at risk during focal cerebral ischemia.
Materials and Methods
Animal Model and Experimental Protocol
The study was approved by the district of Düsseldorf. Rats were anesthetized with ketamine (4 mg/100 g) and xylazine (1.5 mg/100 g), intubated, and ventilated. Core temperature was maintained at 37 ± 0.5°C. The femoral artery and vein were catheterized. Heart rate, aortic mean, and peak pressures were recorded for a 30-second period during each microspheres injection by a Millar micromanometer (Millar Instruments, Houston, TX).
The right middle cerebral artery (MCA) was occluded and reperfused via a transvascular approach, as described in detail elsewhere (7, 8). For application of radiolabeled microspheres (15 μm diameter, 141CE, 95Nb or 46Sc; NEN; Du Pont Co., Boston, MA), animals were intubated and ventilated by using a small-animal respirator. A thoracotomy was performed and the heart was exposed. For each measurement, approximately 2 × 105 microspheres in 0.2 mL saline were injected within 5 seconds directly into the left ventricle. The reference samples were collected from an aortic catheter beginning immediately before the microspheres injection and continued for 1 minute. A total of 1 mL blood was withdrawn at a rate of 1 mL/min by using a constant withdrawal pump (model 901A; Harvard Apparatus, Holliston, MA). The procedure for the determination of blood flow has been described elsewhere (6).
The study protocol consisted of 3 groups of male Sprague-Dawley rats weighing 290–350 g. In group A (n = 8), reperfusion was performed at 1 hour post-MCAO. Injection of radioactive-labeled microspheres was performed before MCAO, 30 minutes post-MCAO, and 30 minutes postreperfusion. To prevent a decline in hematocrit, blood was replaced by injecting heparinized blood from a donor animal during the time of withdrawal of the arterial reference sample into the femoral vein. Procedures for group B (n = 7) paralleled group A, but without blood donation. Procedures for group C (n = 3) also paralleled group A, but without MCAO.
At the end of the experiment, all animals were sacrificed for dissection of brain. Coronal brain sections (1 mm thick) were stained with 2,3,5-triphenyltetrazolium chloride (TTC) and photographed to obtain an independent measure of the ischemic injury. Ischemic lesion volumes were measured by summing the unstained areas of TTC-stained brain sections. To avoid overestimation of the infarction volume, as described by Lin et al (9), the corrected infarction volume (CIV) is given by:  where LT is the area of the left hemisphere in mm2, RT is the area of the right hemisphere in mm2, RI is the infarcted area in mm2, and d is the thickness of the sections.
where LT is the area of the left hemisphere in mm2, RT is the area of the right hemisphere in mm2, RI is the infarcted area in mm2, and d is the thickness of the sections.
The 3 central brain sections were dissected into different regions of interest: the MCA-supplied parietal, temporal, and piriform cortex, as well as the caudate putamen of each hemisphere according to Pacinos and Watson (10). On the basis of the extent of unstained brain tissue, all regions of interest were divided into 3 groups: (1) no tissue necrosis (ie, only vital tissue); (2) partial tissue necrosis (ie, <100% necrotic tissue in the examined region of interest; (3) complete tissue necrosis (ie, complete necrosis of the examined region of interest).
Radioactivity of brain tissue samples and the reference blood withdrawal samples were counted to calculate absolute CBF, as described in detail elsewhere (6). Hereby, absolute CBF was calculated for the different regions of interest in both hemispheres as well as a mean for vital, partially and completely necrotic tissue in the ischemic/reperfused hemisphere.
Relative CBF for each brain area at 30 minutes post-MCAO and 30 minutes postreperfusion was then assessed by relating absolute CBF to its respective baseline CBF-value before MCAO (relative CBFB) and to absolute CBF in corresponding contralateral areas in the noninfarcted hemisphere (relative CBFC).
Data Analysis and Statistics
Hemodynamic data during the time course of the experiment in groups A and B were compared by using a 2-way analysis of variance (ANOVA) for repeated measurements. When significant differences were detected, individual mean values were compared by using post hoc tests. Linear regression analyses between absolute CBF/relative CBF and infarct size (ie, the complete necrotic brain tissue) were performed in groups A and B. All CBF values were analyzed by using of ANOVA and the unpaired Student t test was used to detect CBF changes post-MCAO and postreperfusion. The level of significance was defined as P ≤ .05 (indicated with asterisks [*] in tables). The means and SDs are presented for all data.
Results
Hemodynamics
Physiologic parameters of groups A and B are shown in Tables 1 and 2. There were no significant differences with baseline conditions. During MCAO and during subsequent reperfusion, the mean and maximal aortic pressures decreased, whereas heart rate increased above baseline values. In both groups, pH, pCO2, pO2, and HCO3− were stable through time. In group B, hematocrit decreased significantly, from 40% to 27%. There were no significant differences between group A and sham group C (data not shown).
Physiologic parameters for animals of group A (MCA occlusion, blood replaced)
Physiologic parameters for animals of group B (MCA occlusion, no blood donation)
Infarct Size
The absolute infarct sizes in groups A and B were 102 ± 10 mm3 and 105 ± 37 mm3, respectively, with no significant difference between groups. None of the sham animals had infarcted brain areas.
Obstruction of Cerebral Arterioles after Repeated Application of Microspheres
Averaged relative CBF for both hemispheres in group C after the third application of microspheres was 104 ± 11%, 96 ± 19%, 109 ± 15%, and 110 ± 18% of baseline for the parietal, temporal, and piriform MCA-supplied cortex and the basal ganglia, excluding significant occlusion of cerebral arterioles secondary to repeated microspheres application.
Perfusion Alterations
Absolute and relative CBF measured in groups A and B are shown in Tables 3 and 4.
Cerebral blood flow alterations in animals of group A (MCA occlusion, blood replaced)
Cerebral blood flow alterations in animals of group B (MCA occlusion, no blood donation)
MCA-Supplied Cortex
At baseline, absolute CBF in the parietal cortex was lower than in the temporal cortex but higher than in the piriform cortex (P < .05).
After MCAO, all cortical areas had a significantly decreased absolute CBF; the temporal cortex suffered the greatest decline in CBF from baseline. At 30 minutes reperfusion, none of the cortical areas had a significant increase in CBF, though there was a slight tendency toward improved CBF in the temporal cortex.
Like absolute CBF, relative CBFC and CBFB also decreased significantly after MCAO (P < .05). Although absolute CBF in the temporal and piriform cortex were in the same range, relative CBFC showed a large difference, with 20 ± 18% compared with 63 ± 33% in group A and 30 ± 15% compared with 72 ± 36% in group B. After reperfusion, the parietal and temporal cortex had a significantly increased relative CBFB and CBFC (P < .05).
Basal Ganglia
At 30 minutes post-MCAO, there was no significant decrease in absolute or relative CBF in the basal ganglia of the hemisphere at risk. After reperfusion, there was a slight tendency toward improved absolute and relative CBF.
Blood Flow in Viable and Necrotic Tissue
At 30 minutes post-MCAO, areas of the hemisphere at risk that revealed no tissue necrosis had an average absolute CBF of 0.69 ± 0.07 mL/g/min (group A) and 0.71 ± 0.10 mL/g/min (group B). Partially necrotic areas had an average absolute CBF of 0.39 ± 0.05 mL/g/min (group A) and 0.39 ± 0.09 mL/g/min (group B). Completely necrotic areas had an average absolute CBF of 0.30 ± 0.09 mL/g/min (group A) and 0.32 ± 0.14 mL/g/min (group B).
Average relative CBFC values in viable areas of the hemisphere at risk of groups A and B were 65 ± 8% and 68 ± 12%, respectively, in partially necrotic tissue 46 ± 6% and 50 ± 14%, respectively, and in completely necrotic tissue 34 ± 9% and 39 ± 15%, respectively. Average relative CBFB values in viable areas of the hemisphere at risk were 76 ± 14% and 76 ± 19%, respectively, in partially necrotic tissue 55 ± 10% and 56 ± 17%, respectively, and in completely necrotic tissue 46 ± 12% and 50 ± 20%, respectively.
Relationships between Absolute CBF/Relative CBF and Tissue at Risk
The relationships with absolute CBF/relative CBFC at 30 minutes post-MCAO and percent infarct size (ie, infarct size as fraction of total brain size) are shown in Figs 2A and -B.

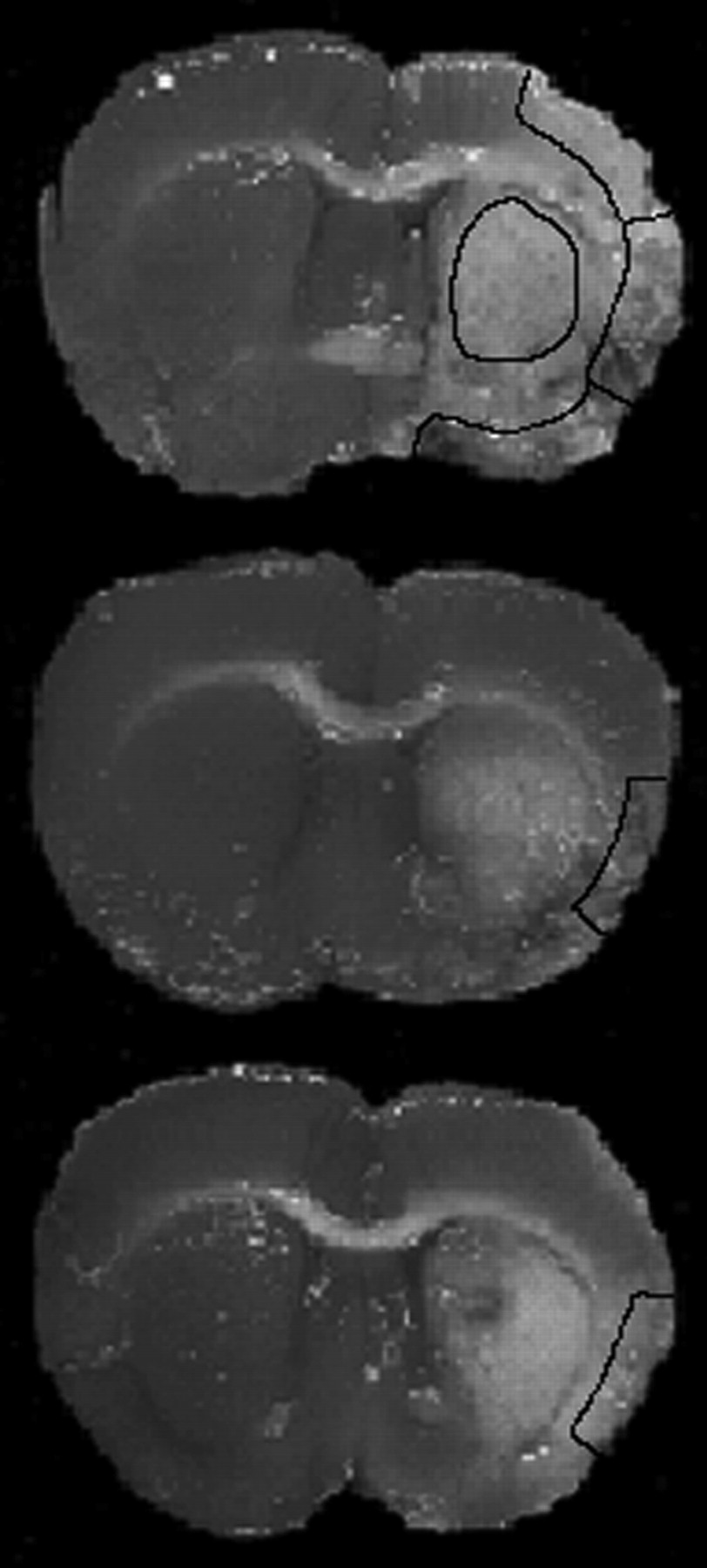
TTC-stained brain sections on the level of the optic chiasm. The white or grayish tissue is unstained and is equivalent to necrotic tissue. The upper section demonstrates a complete infarction of the MCA-supplied territory. Borders of the parietal, temporal, and piriform cortex are outlined as well as the basal ganglia. The middle section demonstrates partial necrosis of the temporal cortex, whereas the lower sections demonstrate complete necrosis.

Relationships between absolute CBF and relative CBFC at 30 minutes post-MCAO and infarct size in groups A (A) and B (B) (expressed as percentage of total brain size). Hkt indicates hematocrit.
Although there were close correlations between infarct size and absolute CBF at 30 minutes post-MCAO in groups A and B (r = 0.79 and r = 0.90), correlations between infarct size and relative CBFC were poor (r = 0.21 and r = 0.17 in group A; r = 0.20 and r = 0.17 in group B). In addition, there were close correlations between infarct size and absolute CBF at 30 minutes postreperfusion in groups A and B (r = 0.66 and r = 0.74, respectively) and only poor correlations between infarct size and relative CBFC or CBFB (r = 0.28 and r = 0.24 in group A; r = 0.18 and r = 0.16 in group B).
Discussion
The aim of this study was to quantify absolute and relative CBF by using radiolabeled microspheres in cortical and subcortical areas during focal cerebral ischemia and subsequent reperfusion. In addition, we tested whether relative CBF is sufficient to predict the development of irreversible tissue damage during cerebral ischemia.
As result, the present study revealed that absolute CBF is superior to relative CBF in predicting irreversible tissue damage following ischemia and reperfusion.
In recent years, several groups have developed methods of transient or permanent MCAO in rodents by insertion of a suture filament into the internal carotid artery to occlude the origin of the MCA resulting in complete infarction of the MCA-supplied territory (8, 11). These methods have been widely applied in the rat to study a variety of ischemia-related questions, such as local CBF alterations during ischemia and reperfusion by autoradiographic measurements (11, 12) and MR imaging (1, 13).
Apart from 14c-iodoantipyrine and radiolabeled or colored microspheres, other techniques provide only relative CBF measurements. Although 14c-iodoantipyrine autoradiography is a reliable quantitative method for evaluation of absolute local parenchymal perfusion (16), it has the methodologic limitation of evaluating absolute CBF distributions only at a single time point (12, 15).
The microspheres technique provides information on blood flow between and within organs and allows serial measurement of absolute CBF by intra-arterial or intracardial injection of either colored or radioactive-labeled spheres. The disadvantage of this technique, especially in small animals, is the amount of blood for withdrawal of arterial reference samples resulting in a significant decline in hematocrit (in this model, 41%–27%). To overcome this problem, blood from a donor animal was injected simultaneously during the time of withdrawal of the reference sample. As a result, hematocrit was kept at baseline levels (41%–42%). By comparing absolute CBF and infarct size of animals with constant and with decreased hematocrit after MCAO and reperfusion, we found no statistically significant difference between the 2 groups.
On the basis of former studies (7), we chose different MCA-supplied cortical areas (parietal, temporal, and piriform cortex) as regions of interest because of their known heterogeneity in blood flow in baseline conditions and good leptomeningeal collateral blood supply after MCA occlusion. In addition, the basal ganglia due to their absent collateral blood supply were analyzed. Although during baseline conditions there were no statistically significant differences in regional blood flows between both hemispheres, absolute CBF in the piriform cortex was only 31% of CBF measured in the parietal cortex, which reflects the broad heterogeneity in cortical blood flows. These results are in line with other reports demonstrating local heterogeneity in cerebral blood flow in the rat by using 14c-iodoantipyrine (3, 12).
Heterogeneity in local cerebral blood flow persisted during MCAO, in rats with both normal and reduced hematocrit. Memezawa et al (12) reported absolute CBF of 0.3–0.6 mL/g/min and Takagi et al (16) of 0.42 ± 0.23 mL/g/min and 0.11 ± 0.05 mL/g/min, in the parietal and temporal cortex during MCAO by using autoradiography. The same authors reported CBF of 0.32 mL/g/min in the ischemic penumbra, ie, tissue at risk at 30 minutes after vessel occlusion. These findings are similar to our absolute CBF measurements: partially necrotic areas had a CBF of 0.39 ± 0.05 mL/g/min.
As a new imaging technique, PWI has been used extensively to demonstrate cerebral perfusion deficits after the onset of focal ischemia in the rat suture model (1, 2). Perfusion-induced signal intensity loss is dependent on the volume and transit of the contrast agent that perfuses the region. Ischemic areas are identified by either a lesser degree of signal intensity loss, a delay in the arrival of the bolus, or an increase in the transit time of the bolus. In an attempt to quantify CBF, tracer kinetic theory has been applied to signal-intensity changes during first-pass bolus tracking (17, 18); however, controversies exist on the validity of these methods, especially during focal cerebral ischemia (2, 5). Nevertheless, the high spatial resolution of the MR technique and its ease of use seem to compensate for some partial volume effects.
The present study shows that for determination of tissue at risk—ie, partially necrotic tissue around the core of completely necrotic tissue—the determination of relative CBF is not sufficient. Although there were close correlations between infarct size and absolute CBF at 30 minutes after MCAO, correlations between infarct size and relative CBF were poor.
Although the validity of infarct size determined by TTC staining after 1 hour of MCAO followed by 1 hour of reperfusion has not been rigorously confirmed by electron microscopy, other studies have used TTC staining to determine necrosis within such timeframe (19). In addition, it should be acknowledged that any single time-point CBF measurement is of limited value in predicting outcome, because the classic ischemic penumbra concept has both a time and magnitude component—ie, severe ischemia for a short period of time may be less deleterious than moderate ischemia for an extended period of time (3, 4).
In the present study, recovery of absolute CBF after 1 hour of permanent MCAO was remarkably heterogeneous: after 30 minutes of reperfusion, absolute CBF in the parietal and piriform cortex, as well as in the basal ganglia of the infarcted hemisphere, decreased as much as 22%; the temporal cortex had a tendency toward an increase in aCBF.
These results are in line with another study in which temporal absolute CBF increased to approximately 30% after 30 minutes reperfusion with a high degree of interanimal variability (12). Partial microcirculatory stasis with subnormal cerebral flow indices after short periods of ischemia followed by reperfusion is frequently described as no-reflow phenomenon: as much as 15% of the capillaries in ischemic tissue remain occluded at least 2 hours after reperfusion, probably because of microembolization or ischemia-induced swelling of perivascular glia cells with subsequent compression of brain arterioles (20).
In the event of spontaneous or therapeutically induced reopening of brain vessels, prediction of definite infarct size by absolute CBF appears feasible, because the present study shows that there is a close correlation between absolute CBF and tissue at risk, not only in the acute phase of cerebral ischemia, but also early during reperfusion.
In conclusion, the use of radiolabeled microspheres for measuring absolute blood flow alterations in the rat suture model after MCAO and subsequent reperfusion revealed broad heterogeneity in local blood flows; in these conditions, absolute CBF is superior to relative CBF, especially when trying to determine tissue potentially undergoing necrosis.
References
- Received February 6, 2005.
- Accepted after revision April 20, 2005.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Predicting experimental success: a retrospective case-control study using the rat intraluminal thread model of stroke
- Congenic Fine-Mapping Identifies a Major Causal Locus for Variation in the Native Collateral Circulation and Ischemic Injury in Brain and Lower Extremity
- MicroRNA Expression in the Blood and Brain of Rats Subjected to Transient Focal Ischemia by Middle Cerebral Artery Occlusion