
Article Figures & Data
Figures
- Fig 1.
Patient 1 is a 39-year-old man with baseline blood pressure 122/61 mm Hg who had severe pneumonia with bronchial obstruction. Bronchial lavage grew Staphylococcus aureus and blood culture grew coagulase-negative staphylococci. Neurotoxicity developed 13 days after positive cultures with severe headache followed by a seizure with blood pressure at toxicity 118/70 mm Hg.
A–B, Brain MR imaging (FLAIR sequence) demonstrates moderate signal intensity abnormality from vasogenic edema in the occipital lobes bilaterally (open arrows) typical of the PRES pattern with full extension to the ventricular surface and moderate local cortical mass effect judged grade 3. Follow up imaging was not obtained, but the patient’s symptoms resolved completely.
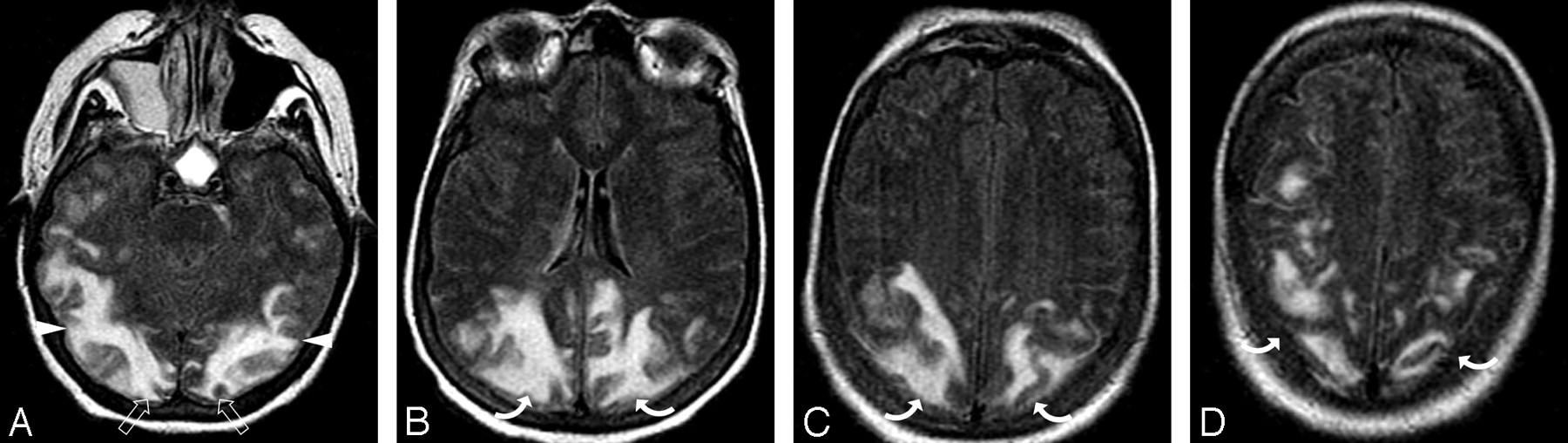
- Fig 2.
Patient 7 is a 68-year-old woman with necrotic pancreatitis, a pancreatic abscess, and baseline blood pressure of 141/67 mm Hg. Abscess grew mixed flora with coagulase-negative staphylococci and Acinetobacter baumannii and blood culture was positive for coagulase-negative staphylococci. Altered mental status with PRES developed 7 days after positive cultures with blood pressure at toxicity of 168/68 mm Hg.
A-B, Brain MR imaging (FLAIR sequence) demonstrates vasogenic edema in the occipital (open arrows) and parietal region (curved arrows) bilaterally typical of PRES with extension into the deep white matter but no extension to the ventricle surface judged grade 2.
C-D, Brain MR imaging (FLAIR sequence) obtained 1 month after initial imaging and toxicity demonstrates near complete resolution of the edema in the occipital (open arrows) and left parietal region (curved arrow) with complete resolution in the right parietal area (arrow).
- Fig 3.
Patient 4 is a 56-year-old woman with a baseline blood pressure of 156/68 who developed a thigh abscess with culture growing mixed flora (Klebsiella pneumonial and enterococci). She developed MOD (coagulopathy, acute respiratory distress syndrome, acute renal failure, liver failure, and shock liver). On day 27 of intensive treatment of her infection and multiorgan failure, the patient developed altered mentation followed by a generalized seizure and blood pressure of 164/75 mm Hg.
A-D, Brain MR imaging (FLAIR sequence) obtained the 1-day after neurotoxicity demonstrates severe and extensive vasogenic edema primarily involving the subcortical white matter of the parietal (curved arrows), occipital (open arrows), and temporal lobe regions (arrowheads) bilaterally with ventricular distortion from edema judged grade 5.
- Fig 4.
Patient 8 is a 55-year-old woman with multiple liver metastases from renal cell carcinoma who underwent liver wedge resection and intraoperative chemotherapy infusion. Baseline blood pressure was 115/70 mm Hg. She developed ARDS and Streptococcus pneumoniae sepsis 3 days after resection followed by pneumonia (S aureus) and line sepsis (coagulase-negative staphylococci). Patient developed altered mental status 3 days after pneumonia and bacteremia with blood pressure at toxicity of 150/80 mm Hg.
A-C, Brain CT images obtained at toxicity demonstrate vasogenic extensive edema in the occipital (open arrows), parietal (curved arrows), and frontal regions (arrows) bilaterally with focal edema also noted in the anterior limb internal capsule bilaterally (arrowheads) consistent with PRES with ventricular compression and deformity from the edema judged grade 5.
D, Follow-up brain CT imaging performed 1 month after initial imaging demonstrates complete reversal of the PRES pattern shown here in the parietal (curved arrows) and frontal (arrows) regions bilaterally.
- Fig 5.
Patient 2 was a 73-year-old woman who had undergone gastric surgery. Her baseline blood pressure of 157/77 mm Hg. She developed aspiration and pneumonia. Bronchial washings and blood cultures grew Pseudomonas aeruginosa. Neurotoxicity developed 6 days after positive cultures with altered mental status and blood pressure 128/80 mm Hg.
A-C, Brain MR imaging (FLAIR sequence) obtained at the time of toxicity demonstrates an unusual pattern of vasogenic edema in the parietal region bilaterally much greater on the left (curved arrows) involving both cortex and some extension to the deep white matter judged grade 2.
D, MRA obtained at the same time as imaging demonstrates diminutive severely “pruned” intracranial vessels, in particular MCA branches (arrows).
E, Follow-up brain MR imaging (FLAIR sequence) obtained 1 month after initial imaging demonstrates complete resolution of the vasogenic edema bilaterally shown here only on the left (curved arrow). Incidental subdural hygromas are also present.
F, Follow-up MRA also obtained 1 month after initial imaging demonstrates marked improvement in vessel visualization with partial reversal of the severe “pruning” and spasm in the MCA branches (arrows) bilaterally. The patient’s mental status completely normalized.
- Fig 6.
Patient 19 was a 54-year-old woman who had undergone gastric bypass surgery. She developed a severe pneumonia 2 months after surgery that eventually required intubation along with antibiotic treatment. This occurred while she was being treated at an outside hospital. The patient developed vision changes, confusion, and hypertension (200/100 mm Hg) during treatment with initial CT imaging reported as negative, and she was transferred to our facility for advanced management.
A-C, Brain MR imaging (FLAIR sequence) obtained 1 day after the development of toxicity and transfer demonstrated focal areas of vasogenic edema in the frontal lobes (arrows), parietal region (curved arrows), and occipital poles (open arrows) bilaterally with a mild degree of severity. Frontal lobe signal intensity is linear along the superior frontal sulcus (arrows), disconnected from the parietal abnormality (curved arrows) consistent with PRES and judged grade 1.
D, MRA at the time of initial MR imaging demonstrates extensive vasospasm of first-, second-, and third-order branches in the anterior cerebral artery (arrowheads), middle cerebral artery (arrows), and posterior communicating artery (short arrows) vessels bilaterally. A “node”-like appearance is seen at many branch points of the main parent vessels typical of spasm (black arrows 4G). Similar findings were also present in the posterior circulation.
E-F, Axial FLAIR image obtained on follow-up imaging study 11 days after the initial study demonstrates reversal of the vasogenic edema in all regions.
G, Repeat MRA obtained 11 days after the initial study demonstrates resolution of the extensive vasospasm with a near-normal appearance of all vessels (arrows).






Tables
Edema Grade Description Points Grade 1 Cortex edema, limited subcortical white matter edema or both Involved regions nonconfluent Slight local cortex mass effect/distortion due to edema 1 Grade 2 White matter edema slightly greater in thickness than cortex edema White matter edema extends into deep white matter Primarily without wide medial-to-lateral extension Some involved regions occasionally confluent Local cortical mass effect/distortion due to edema 2 Grade 3 White matter edema substantially greater in thickness than cortex edema Some limited and focal extension to ventricular surface Developing wide medial-to-lateral extension Involved regions partially confluent Moderate local cortex mass effect/distortion due to the edema 3 Grade 4 White matter edema substantially thicker than cortex edema Involved regions substantially extend to ventricular surface Diffuse wide medial-to-lateral extension Involved regions almost completely confluent No ventricular distortion due to the edema 4 Grade 5 White matter edema severe and dominates cortex edema Involved regions fully confluent and continuous Diffuse wide medial-to-lateral extension Fully extends to the ventricular surface Ventricular deformity due to the edema 5 Toxicity Category No. of Patients Subgroup No. of Patients Time Point of PRES Relative to ‘Association’ Event 0–1 mos (# pts) 1–4 mos (# pts) 4–12 mos (# pts) > 12 mos (# pts) Not Known (# pts) Cyclosporine/FK-506 toxicity 49 allo-BMT 26 16 5 4 1 SOT 20 5 3 5 7 CsA only 3 3 Postchemotherapy 4 4 3 1 Infection/sepsis/shock 25 Infection/Sepsis 23 21 1 1 Hemorrhagic Shock 2 2 Eclampsia 11 Intrapartum 3 3 Delayed 8 8 Autoimmune 11 11 11 Miscellaneous 6 6 6 Total 106 106 56 10 9 8 23 Note:—# pts indicates number of patients; mos, months; SOT, solid organ transplant; CsA only, cyclosporine treatment in marrow diseases; PRES, posterior reversible encephalopathy syndrome; allo-BMT, allogenic bone marrow transplantation.
Pt # Age Sex Major Clinical Problem and Infection Cultured Organism S/S MOD Delay PRES Neurotoxicity BP Base BP Tox MAP Tox Organ/Tissue Blood Group 1 1 39 M Pneumonia with bronchial obstruction, decubitus ulcer S. aureus Staph coag neg Y 13D Headache Seizure 122/61 118/70 86 2 73 F Gastric surgery, pneumonia, aspiration Pseudomonas P. aeruginosa Y CR 6D Altered MS 157/77 128/80 78 3 59 F Bowel perforation, abscess, sepsis, MOD, antiphospholipid syndrome Pseudomonas Staph coag neg Y CP 13D Altered MS 143/79 150/56 87 Staph coag neg 4 56 F Thigh abscess Klebsiella Y CP 27D Seizure 156/68 164/75 104 Enterococcus F1 LR 5 24 F CML in blast crisis, isolated bacteremia, sepsis, chemotherapy Enterobacter Y PL 20D (15D) Slurred speech 122/82 125/85 98 R Ataxia Seizure 6 20 M ALL, chemotherapy, skin infection Staph coag neg 1. Diphtheroids – CP 7D Seizure 120/70 150/88 106 2. Staph coag neg LR 7 68 F Necrotic pancreatitis, pancreatic abscess Staph coag neg Staph coag neg Y CP 7D Altered MS 141/67 168/68 101 Acinetobacter L 8 55 F Liver metastatis, open hepatic chemotherapy infusion, pneumonia S. aureus 1. S. pneumoniae Y CP 3D Altered MS 115/70 150/82 104 2. Staph coag neg LR 9 66 F Toe infection and abscess, diabetic S. aureus R 9D Seizure 132/52 160/60 93 Staph coag neg Yeast 10 79 F Lap-cholecystectomy; severe abdominal hemorrhage Y CP LR 7D Altered MS 138/73 137/74 95 Group 2 11 61 F Postoperative wound infection S. aureus S. aureus 11D Headache 145/65 210/102 138 Vision loss 12 24 F Isolated bacteremia 2 mo post Tx removal S. viridans R 0D Headache Seizure 125/90 170/126 140 13 22 M Original sickle cell crisis w/pneumonia-bacteremia, new sickle cell crisis w/heavy rectal colonization N/A Staph coag neg CR 2M Sickle crisis Seizure 122/80 200/100 133 Enterococcus F2 14 37 M Chronic septic arthritis, shoulder abscess S. aureus N/A CR ? Headache Vision change 175/85 184/111 135 Seizure 15 26 F Crohn disease, bowel perforation, abdominal abscess Enterococcus F1 Staph coag neg Y CP 7D Seizure 115/65 182/100 126 Enterococcus F2 E coli 16 51 F Breast carcinoma, auto-BMT, pneumonia Pseudomonas 1. Micrococcus Y C p L 9D Seizures 121/74 164/100 123 Klebsiella 2. Enterococcus Staph coag neg 3. Staph coag neg 17 55 M Foot infection, diabetic N/A on antibiotics C 0D Headache Vision change 191/88 215/115 148 18 57 F Post gastric stapling, acute UTI Enterococcus F1 Staph coag neg 2D Altered MS Seizure 136/70 203/93 129 19 54 F Pneumonia, severe; intubated N/A outside hosp 9D Vision change Altered MS 112/85 200/100 133 20 81 F Axillary abscess, chemotherapy S. aureus 1. S. aureus Y CL 30D Slurred speech Altered MS 130/52 203/110 141 2. Staph coag neg Seizure 21 37 F Necrotizing pancreatitis, pneumonia N/A outside hosp 7D Headache Seizure 162/92 220/126 157 22 56 F Sickle cell crisis, pneumonia S. viridans R 4D Altered MS Seizure 150/84 170/110 130 23 24 F Alcohol intoxication, shock, bowel perforation N/A on antibiotics Y CP LR 6D Seizure 140/90 203/113 143 24 38 F Peritonitis, PD, renal insufficiency Pseudomonas Pseudomonas 14D Altered MS 145/94 210/110 143 25 19 F Dialysis catheter hemorrhage Y CP R 15D Headache Vision change 149/86 207/106 140 Seizure Note:—S/S indicates clinically hemorrhagic shock or sepsis, severe sepsis, or septic shock before developing PRES; Y, yes; MOD; multiorgan dysfunction developed coincident with PRES; C, coagulation, drop in platelet count; P, pulmonary dysfunction-edema, intubation; L, hepatic dysfunction, rising and elevated bilirubin; R, renal dysfunction, rising and elevated creatinine; Delay, closest time from recognized infection/bacteremia/shock to onset of neurotoxicity and PRES; MS, mental status; BP, blood pressure (mm Hg); base, baseline; tox, at toxicity; MAP, mean arterial pressure; N/A, not available; Tx, transplant; PD, peritoneal dialysis; UTI, urinary tract infection; PRES, posterior reversible encephalopathy syndrome. CML, chronic myelogenous leukemia; ALL, acute lymphoblastic leukemia; auto-BMT, auto-bone marrow transplant; S aureus, Staphylococcus aureus; Staph coag neg, coagulase-negative Staphylococci; E coli, Escherichia coli; S viridans, Streptococci viridans; S pneumoniae, Streptococci pneumoniae. Multiple organisms listed together correspond to mixed flora infections. Numbered blood culture organisms correspond to separate blood culture results with different organisms in the PRES time frame. F1, faecalis; F2, faecium. In patient 5, initial neurotoxicity began 15 days after sepsis/7 days after chemotherapy. Initial imaging negative (16 days), repeat imaging demonstrating PRESS (20 days).
Pt # Imaging Locations of PRES Vasogenic Edema MRA Imaging Modality DWI F/U Imaging Clinical at Discharge Edema Grade MAP C T O P F Misc Group1 1 x x x MR n/o Resolved 3 86 2 Spasm-imp MR Neg Res 2 78 3 x x x x MR Neg Resolving Resolved 5 87 4 x x x x x t Pruning MR n/o Resolved 5 104 5 x x x x CT Res 3 98 6 x CT Expired 2 106 7 Pruning MR Neg Resolving Resolved 2 101 8 x x x x CT Res 5 104 9 x x x x Normal MR Neg Res 2 93 10 x x x MR Neg* Resolving Resolved 4 85 Group 2 11 x x x x t mb Spasm/prun MR Neg Normal 2 138 12 x x x x MR Neg Res 3 140 13 x x x x x bs mb c MR Neg Res 1 133 14 x x x x x bs MR Neg Res 3 135 15 x x x x CT Resolved 1 126 16 x x x CT Expired 2 123 17 x x x t Spasm MR Neg Resolving Resolved 2 148 18 x x x x Spasm MR Neg Resolving Resolved 3 129 19 x x x Spasm-rev MR Neg Res 1 133 20 x x x x bs MR Neg Resolving Resolved 2 141 21 x x MR Neg — Resolved 1 157 22 x x x x Spasm MR Neg Res 4 130 23 x x x x MR Neg Res 1 143 24 x x x x Spasm-rev MR Neg* Res* 3 143 25 x x x x MR n/o Res 2 140 Note:—PRES indicates posterior reversible encephalopathy syndrome; C, cerebellum; T, temporal lobe/inferior temporal-occipital junction; O, occipital lobe; P, parietal region; F, frontal lobes; bs, brain stem including medulla and pons; mb, midbrain; t, thalamus; c, caudate nucleus; rev, spasm reverses; imp, spasm improves; spasm/prun, middle crebral artery spasm with posterior cerebral artery pruning; DWI, diffusion-weighted image characteristics; n/o, DWI not obtained with MR imaging study; Neg, no evidence of restricted diffusion to suggest cytotoxic edema; Neg*, no restricted diffusion in the majority of vasogennic edema with focal region of restricted diffusion and hemorrhage noted; Res, vasogenic edema completely resolved on follow-up imaging studies; Res*, vasogenic edema resolved with minor persistent abnormal signal in region of previously noted restricted diffusion, infarction, or focal hemorrhage; Resolving, resolving vasogenic edema on follow-up imaging studies or resolving clinical symptoms related to PRES; Resolved, clinical symptoms at PRES neurotoxicity resolved; MAP, mean arterial pressure.
- Table 5:
Vasogenic edema grade in Group 1 (Normotensive) and Group 2 (Severely Hypertensive) Patients
Blood Pressure Group Vasogenic Edema Grade (Number of Patients) Group Average Grade 1 Grade 2 Grade 3 Grade 4 Grade 5 Group 1 0 4 2 1 3 3.3 Group 2 5 5 4 1 0 2.07
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Posterior reversible encephalopathy syndrome presenting with thrombotic microangiopathy triggered by malignant hypertension: a case report and literature review
- Serial Imaging of Virus-Associated Necrotizing Disseminated Acute Leukoencephalopathy (VANDAL) in COVID-19
- Posterior reversible encephalopathy syndrome in scrub typhus fever
- Tumour-like presentation of atypical posterior reversible encephalopathy syndrome with prominent brainstem involvement
- A case of posterior reversible encephalopathy syndrome associated with sepsis
- Controversy of posterior reversible encephalopathy syndrome: what have we learnt in the last 20 years?
- CNS Endothelial Cell Activation Emerges as a Driver of CAR T Cell-Associated Neurotoxicity
- Status epilepticus as the initial presentation of antibody-negative Goodpasture's syndrome
- Magnetic Resonance Imaging of Cerebral Malaria Patients Reveals Distinct Pathogenetic Processes in Different Parts of the Brain
- Generalised reversible encephalopathy syndrome: a variant of posterior reversible encephalopathy syndrome (PRES)
- Posterior reversible encephalopathy syndrome resulting from repeat bortezomib usage
- Transient Lesion in the Splenium of the Corpus Callosum in Acute Uncomplicated Falciparum Malaria
- Postoperative Blindness Due to Posterior Reversible Encephalopathy Syndrome Following Spine Surgery: A Case Report and Review of the Literature
- The posterior reversible encephalopathy syndrome in HIV infection
- Posterior Reversible Encephalopathy Syndrome During Ipilimumab Therapy for Malignant Melanoma
- The posterior reversible encephalopathy syndrome: what's certain, what's new?
- Type of Edema in Posterior Reversible Encephalopathy Syndrome Depends on Serum Albumin Levels: An MR Imaging Study in 28 Patients
- Plasma From Preeclamptic Women Increases Blood-Brain Barrier Permeability: Role of Vascular Endothelial Growth Factor Signaling
- Influenza A Encephalopathy, Cerebral Vasculopathy, and Posterior Reversible Encephalopathy Syndrome: Combined Occurrence in a 3-Year-Old Child
- Unusual findings and diagnostic challenges in a child with Lemierre's disease
- Hemorrhage in Posterior Reversible Encephalopathy Syndrome: Imaging and Clinical Features