
Abstract
SUMMARY: Giant cell tumor (GCT) of the sphenoid bone is a relatively rare entity and metachronous multicentric GCT of the sphenoid is even rarer; we are aware of only 3 previous cases in the literature. We describe here a tumor of the sphenoid bone that was identified 15 years after multiple resections of a GCT of the left inferior pubic ramus. Correlation is made between the histopathologic findings, MR imaging of the brain, CT of the head, and fusion positron-emission tomography (PET)/CT scan performed with fluorine-18 fluoro-2-deoxy-D-glucose (18F-FDG). This report is the first to describe the appearance of a GCT of the sphenoid bone on a fusion PET/CT examination. High metabolic activity in the base of the skull adjacent to the middle cranial fossa was demonstrated in a fashion similar to that of the known pelvic lesion. This case also demonstrates that the increased metabolic activity seen in a GCT of the sphenoid bone may be partially obscured by the adjacent physiologic high metabolic activity of the brain.
Multicentric GCT is a relatively rare entity within the spectrum of giant cell tumors (GCTs), composing less than 1% of all cases of GCT. This variant is usually described in the extremities.1,2 GCT of the sphenoid bone typically presents with symptoms related to palsies of the adjacent cranial nerves, particularly diplopia or sensory symptoms attributable to the facial nerve such as pain or numbness.3,4 Metachronous (occurring at different times) or multicentric (occurring at multiple sites) tumors of the sphenoid bone are even rarer, with only 3 described cases.2,3 Imaging findings consistent with erosion of the sphenoid bone may be seen, along with contrast enhancement.4 There is also potential for extension into the adjacent cavernous sinus or sphenoid sinus; this spread may invade or impinge the internal carotid artery adjacent to the anterior clinoid process. Primary GCTs have similar clinical presentations.5,6 The case reported here is a locally aggressive lesion of the sphenoid bone occurring years after the treatment of a primary pelvic lesion, with correlation between clinical history, histopathology, and imaging findings (including skull base CT scan, MR imaging, and fusion positron-emission tomography [PET]/CT scan). The mean standardized uptake value (SUV, correlating activity within the tissue volume of interest with injected fluorine-18 fluorodeoxyglucose [18F-FDG] dose and patient body weight) was calculated in the sphenoid lesion and correlated with that of the pelvic tumor.
Case Report
Fifteen years before the presentation described here, a 44-year-old woman was treated for GCT of the left ischium and left inferior pubic ramus. Multiple surgical resections of the pathologically proved GCT were performed, including bone-packing procedures, because of tumor recurrence at 15, 14, 13, and 10 years before the current presentation. The tumor was ultimately thought to have been removed, and the patient was relatively asymptomatic for approximately 7 years, until approximately 3 years before the current presentation, when discomfort recurred at the primary pubic site. This recurrence was initially treated conservatively (because the tumor was thought not to be malignant), but the extension of the recurrent tumor into the pelvis (with bladder involvement) warranted more aggressive treatment. Preoperative embolization and local irradiation were initially performed. Surgical exploration and subsequent extensive ischiopubic and adjacent pelvic resection soon followed, and the patient was treated with pelvic irradiation as well. This surgical resection was performed less than 1 year before the presentation described here.
The patient presented approximately 10 months later with headaches and numbness involving the left side of the face and the left upper lip, suggesting abnormalities of the V1 and V2 cranial nerves. A subsequent thorough cranial nerve physical examination by the neurosurgeon was unable to elicit muscular weakness or other cranial nerve abnormalities. Audiology was performed, revealing bilateral mild-to-moderate high-frequency hearing loss. On the basis of these findings, a contrast-enhanced head CT was performed. This examination revealed a large soft-tissue mass in the left anterior skull base, with associated osteolysis involving the greater and lesser wings of the left sphenoid bone as well as extension into the sphenoid sinus to the left of midline. There was also extension of tumor into the left cavernous sinus and Meckel cave (Fig 1A), consistent with the clinical findings of multiple cranial nerve V neuropathies. The tumor also appeared to partially surround the superior and inferior orbital fissures, obliterating the bony lateral walls of these foramina, and to extend caudally into the foramen ovale. These findings were confirmed on the subsequent brain MR imaging (Figs 1B–D).

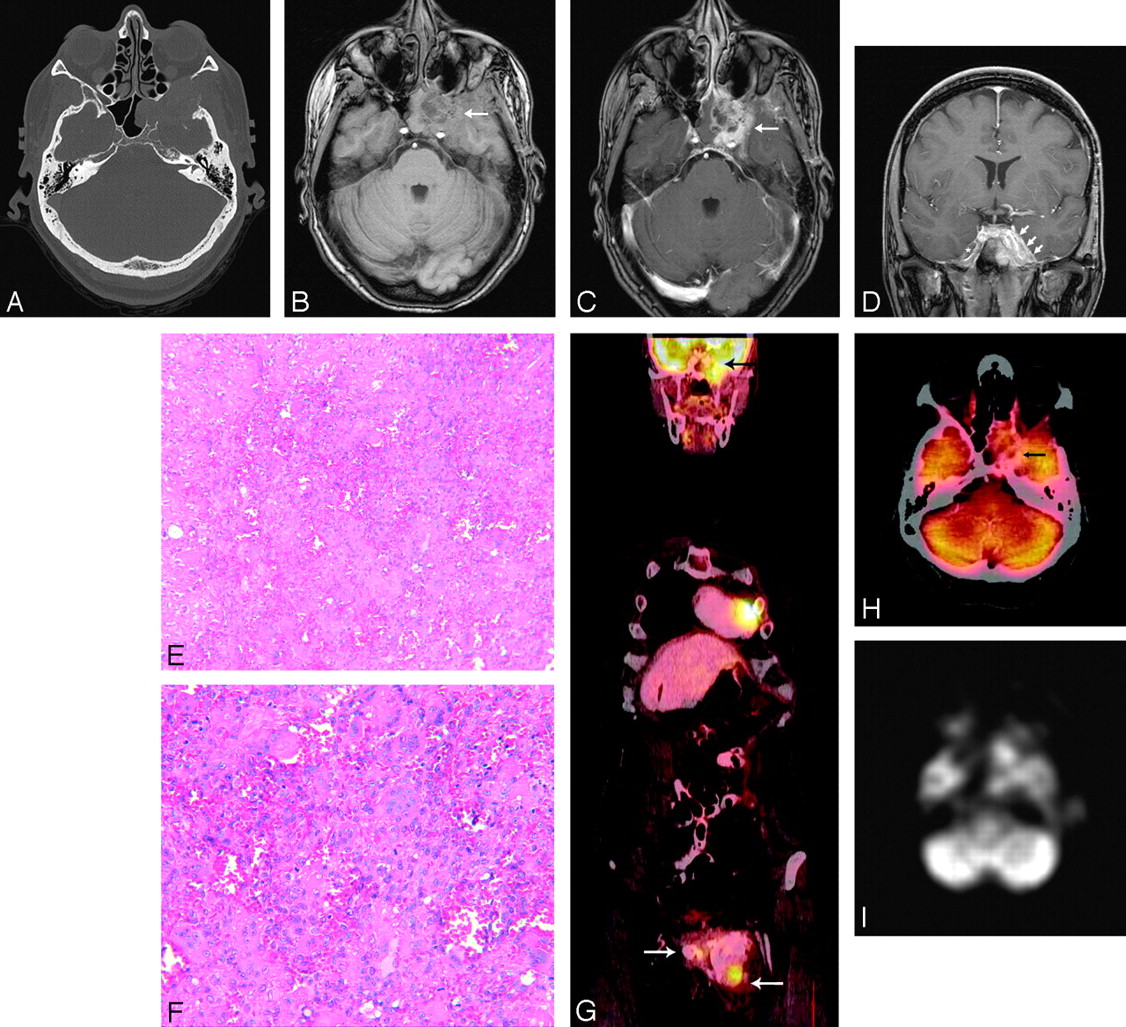
A 44-year-old woman presented with a history of pelvic GCT recurrence, with a mass of the left ischium and left inferior pubic ramus, identified and treated at that site 15 years previously. The patient presented with new left facial numbness, indicating likely trigeminal nerve sensory root deficits. Contrast-enhanced CT of the skull base was performed (A, bone windows) to evaluate a suspected lesion. A lytic and contrast-enhancing mass was seen involving the lesser and greater wings of the sphenoid bone, with possible invasion of the cavernous sinus and Meckel cave. Brain and skull base MR imaging demonstrated a heterogeneously enhancing mass obliterating the sphenoid sinus to the left of midline, with invasion of the left cavernous sinus and Meckel cave on axial pre- and postcontrast T1-weighted images (B and C, arrows), explaining the patient’s symptoms (note the lack of well-visualized nerve roots within an obliterated left Meckel’s cave on coronal T1-weighted postcontrast images [D, arrows], compared with the roots on the more normal opposite side [asterisk]). Microscopic examination (E, hematoxylin-eosin, original magnification ×10) from the sphenoid bone biopsy sample and partially resected tumor shows a highly vascular tumor comprising abundant osteoclast-like giant cells intermixed with mononuclear epitheloid cells. Reactive osteoid was present focally (left), likely at the advancing border of the tumor. Higher power view (F, original magnification ×20) demonstrated that the nuclear features of the epitheloid cells resembled those of the multinucleated cells, with mitotic figures being common throughout the sample. Findings were consistent with GCT (and not metastatic disease) and were similar to those of the pelvic lesion. Coregistered fused PET/CT coronal (G) and axial (H) reformations performed 3 months later (to evaluate the remainder of the body) demonstrated high metabolic uptake within the sphenoid mass (black arrow; SUV, 7.4) and the recurrent left pubic lesion at the primary site (with associated surrounding bone cement; white arrows; SUV, 8.4). Note that it may be difficult to distinguish a discrete sphenoid lesion adjacent to the normal relatively high metabolic activity of the cerebral cortex in the adjacent middle cranial fossa, particularly on the nonfused PET data (I).
Given the patient’s history, we thought that these findings were most likely due to recurrent GCT. Because this would represent metachronous GCT, it also raised the concern for the possibility of additional sites of GCT recurrence, as well as sphenoid chondrosarcoma, chordoma, or even metastasis of another origin. The patient subsequently underwent biopsy of the greater sphenoid portion of the mass, via the infratemporal fossa.
The neuropathologist thought that the histologic findings were typical of GCT, though the anatomic location of this tumor was considered somewhat unusual. Histologic sections (Figs 1E,-F) of the biopsy sample showed abundant mononuclear stromal cells with round-to-ovoid nuclei and prominent nucleoli, intermixed with evenly spaced osteoclast-like multinucleated giant cells. Widespread foci of hemorrhage, a marked fibrocollagenous reaction, and areas of reactive bone formation were also noted. No malignant features or evidence of dedifferentiation were noted to suggest the possibility of metastasis. The histologic findings were considered similar to and consistent with those found in the complex pelvic mass.
A combined MR imaging of the lumbar spine and pelvis (not shown), performed days after the brain MR imaging, demonstrated new lesions within the right iliac bone and inferior pubic ramus, as well as postoperative changes in the left hemipelvis. No definite vertebral lesions were seen.
The sphenoid tumor was subsequently resected. It was not feasible to remove the lesion in its entirety, and residual tumor was present. The patient refused radiation treatment to the sphenoid lesion, so local radiation therapy was not performed. The patient subsequently began a regimen of chemotherapy (doxorubicin and ifosfamide) within 3 months following the sphenoid surgery.
Fusion PET/CT examination performed 3 months after sphenoid resection demonstrated a hypermetabolic lytic lesion involving the left sphenoid bone (Fig 1G; maximum SUV, 7.4). There was also a hypermetabolic mass within the left ischium and left inferior pubic ramus (site of primary lesion; SUV, 8.4) and hypermetabolic foci within the right inferior pubic ramus (SUV, 9.2) and right iliac spine (Fig 1H; SUV, 6.3). A pathologic fracture of the L3 lamina was seen along with associated hypermetabolic activity (SUV, 4.9). In addition, a hypermetabolic focus (SUV, 7.5) was seen in the left lung.
Discussion
Sim et al2 described 2 cases of multicentric GCT of the sphenoid bone and recommended aggressive surgical treatment of these lesions, along with radiation therapy. These authors concluded that multicentric or metachronous GDTs demonstrate aggressive behavior similar to that of the primary GCTs. Yamamoto et al3 also demonstrated a case of locally aggressive multicentric GCT invading the sella and presenting with diplopia. This patient was treated with partial resection and chemotherapy. Long-term follow-up showed partial regression, but tumor remnant persisted within the sphenoid sinus 11 years after initial treatment. In the patient described here, there was recurrence of the primary lesion in the left inferior pubic ramus and left ischial region many years after resection, whereas an aggressive lesion arose in the sphenoid bone 3 years after this recurrence at the primary site. As in the article of Yamomoto et al, the patient described in this report was ultimately treated with a combination of a chemotherapy and partial resection.
Histopathology of sphenoid GCT usually demonstrates multinucleated giant cells with spindle-shaped cells.3,5 Sections from the initial tumor, in this patient, showed the typical histologic features of this relatively uncommon usually benign tumor. The anatomic location of the sphenoid tumor was somewhat unusual, but the histopathologic features were still representative of GCT of bone and were similar to those seen in the previous pelvic specimen. Although there are no specific histopathologic features that predict the clinical behavior of GCTs, there were no worrisome findings (such as dedifferentiation) in this patient to suggest that the sphenoid tumor had originated as a metastasis. The time interval between the occurrence of the original pelvic tumor and the occurrence of the sphenoid tumor, as well as the occurrence of this second tumor in bone rather than in lung, would be unusual for metastasis but might occur with a GCT. The high degree of cellularity, presence of mitotic figures, reactive bone formation, and fibroblastic proliferation would all correlate well with the finding of a metabolically active lesion on the fusion PET/CT scan. The destructive or lytic nature of this neoplasm was somewhat difficult to appreciate on the histologic examination because few, if any, residual normal bone spicules were seen in the specimen, a feature sometimes true of lytic lesions.
To our knowledge, this is the first case report describing the PET/CT appearance of either primary or metachronous GCT of the sphenoid bone and is the first known presentation of correlation between histopathology, MR imaging features, CT appearance, and PET/CT in sphenoid GCT. Strauss et al6 described FDG-PET findings of 18 GCTs located in the extremities, as well as 1 primary lesion of the thoracic spine. In these patients, the mean SUV was 4.8. Similar SUVs have also been described in FDG-PET studies of GCT of the tendon sheath performed as part of a larger study of musculoskeletal tumors, with an SUV of 4.57.7 Identification of tumor recurrence through surveillance following radio- and chemotherapy has been a major use for PET with respect to many tumors besides GCT.8
A small lesion in the sphenoid bone that abuts the middle cranial fossa may be obscured by the high metabolic activity of the normal cerebral tissue on low-resolution or non-coregistered PET scans or may alternatively appear to be adjacent sinus disease. Therefore, suspected lesions of the sphenoid bone or cavernous sinus should undergo evaluation by fusion PET/CT if at all possible; optimally this would be performed for tumor surveillance as well.
GCTs are considered to be benign tumors; however, metachronous lesions or metastases may rarely occur. In this case, the patient had a higher SUV compared with those reported in previous cases describing GCTs. This is of interest because higher SUVs suggest a more aggressive tumor9 and correlate well with the history of the patient’s disease. Further evaluation is needed to determine whether correlation between elevated SUVs and the occurrence of metachronous lesions are a general feature of this rare presentation of GCT.
References
- Received August 17, 2005.
- Accepted after revision November 10, 2005.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.