
Abstract
SUMMARY: The embolization of missiles to the intracranial circulation is a rare event. We describe here a case of a man shot by a shotgun, presenting with a posterior fossa stroke and occlusion of the superior cerebellar artery by a metallic pellet. To our knowledge, this is the third case of posterior fossa circulation pellet emboli.
Arterial migration of missiles is a very rare complication of penetrating trauma. The embolization of these missiles to the cerebral circulation is even rarer, and most reports are related to anterior circulation events. We describe a case of embolization of a shotgun pellet to the posterior cerebral circulation with a 2-year follow-up and discuss the management options of such an unusual traumatic lesion.
Case Report
A 76-year-old man was sent to our institution 2 weeks after a hunting accident in which he was shot in the left shoulder and neck. Standing to the right and forward of his hunting partner, the patient sustained the injury at a distance of approximately 20 feet. There was no loss of consciousness and initially no symptoms aside from pain. He then felt dizzy without vertigo and his balance was disturbed. He walked with assistance out of the woods to an ambulance. He was assessed in the emergency department of a local hospital. Conventional radiographs of the head and neck were taken, and the multiple pieces of buckshot were determined to be in the soft tissue of the neck. He was treated conservatively and discharged. He was referred by his family physician when the symptoms of imbalance persisted. Neurologic examination showed evident gait disturbance (ataxia), slight left hand weakness, and a more evident dysdiadochokinesia in the left arm and hand. A CT scan was performed and the patient was sent later for neurosurgical evaluation at our institution. A metallic pellet was shown in the interpeduncular cistern and hypoattenuation consistent with ischemic infarcts in the cerebellar hemisphere (Fig 1). An angiogram showed no abnormalities in either the carotid or vertebral arteries in the neck (Fig 2). Occlusion of the left superior cerebellar artery by the metallic object was demonstrated on the vertebral angiogram (Fig 3). With an established infarct, aspirin (325 mg daily) was prescribed, and the patient demonstrated gradual improvement from his cerebellar deficit. By the latest follow-up visit, 2 years after the accident, he has been able to resume most of his normal activities, despite a very mild persistent cerebellar deficit. At his last follow-up visit, he still showed some imbalance, especially if asked to walk in a line.

Conventional radiographs and CT showing the location of the intracranial pellet in the interpeduncular cistern. A small area of hypoattenuation can be seen on the left superior cerebellar peduncle.

Angiogram showing the normal left and right vertebral arteries in the neck.
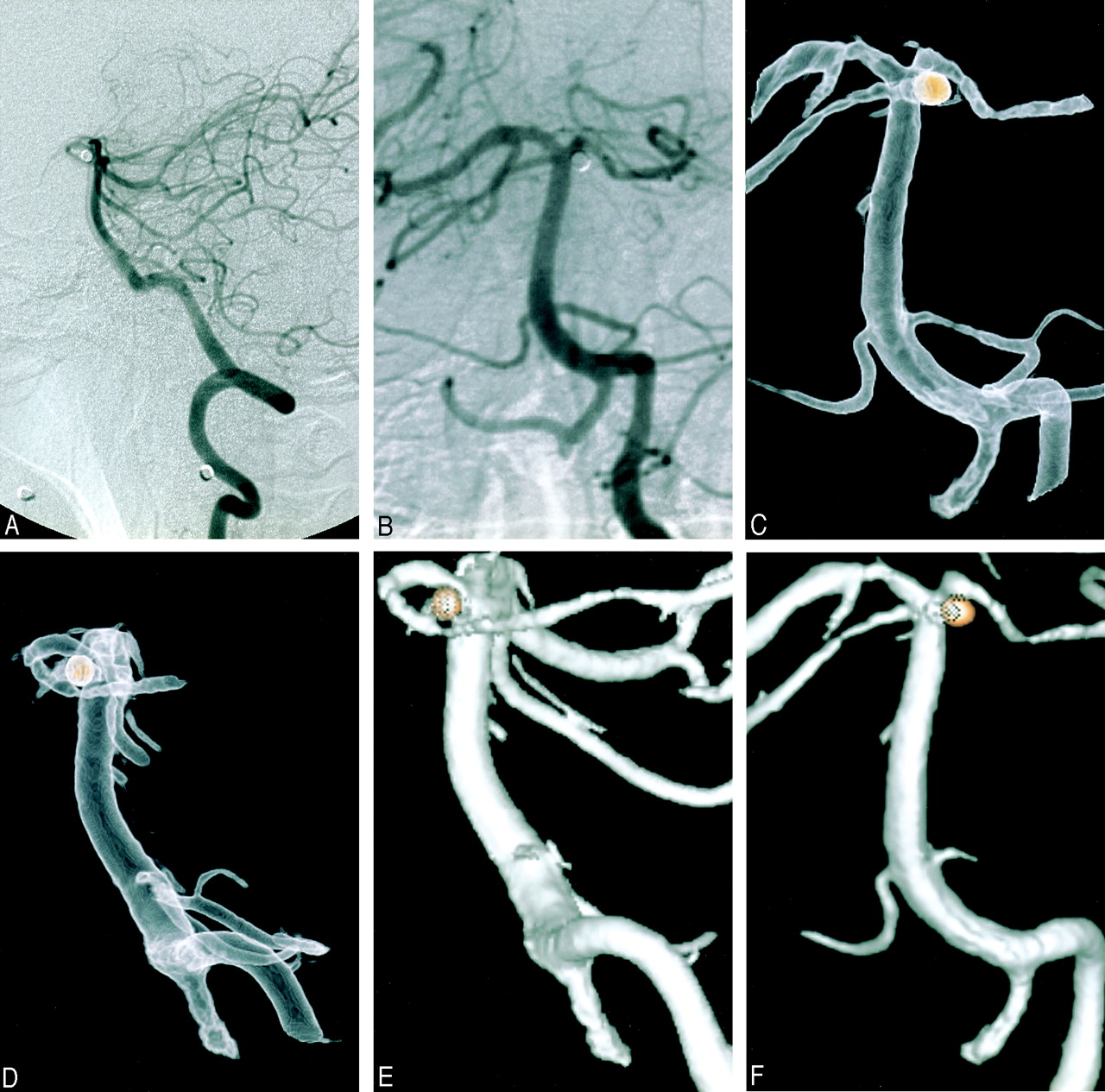
Angiogram, showing exclusion of the left superior cerebellar artery and the metallic pellet in its usual origin location.
Discussion
Although not common, intravascular migration of missile emboli has been reported in the literature.1,2 In a review of 7500 penetrating traumas from the Vietnam War, Rich et al reported 22 cases of missile emboli, with 19 being arterial embolizations.3 Migration to the cerebral circulation is even rarer: of the 22 cases reported by Rich et al, only 3 occurred and were confined to the carotid circulation.
Stein et al found 15 cases of migration of missiles to the carotid/vertebral circulation, with only 11 involving the intracranial circulation, most lodging in the middle cerebral artery territory.4 Embolization to the posterior circulation has been reported only twice in the literature, to the best of our knowledge.5,6 The occurrence of embolism after penetrating vascular trauma depends on the size of the missile and its velocity. Small size and low velocity are requirements for embolization to occur.1 To allow intravascular embolization, a great part of the pellet energy dissipates in the soft tissues during the penetration in the body, but it keeps enough energy to puncture one of the vessel walls, but not the other, staying in the lumen. It is also a requirement that the vessel should be larger than the pellet. A high-speed missile would just transect the vessel and a larger projectile would either destroy it or compress it, if of low speed. Shotgun wounds are therefore the injuries most commonly related to this phenomenon, because of the small size and low velocity of the missile and the wide area covered by the pellets, which facilitates arterial or venous penetration. The site of entrance of the missile in the vascular tree in cases of embolization to the intracranial circulation is usually the chest and/or the neck, where it can either enter the heart, aortic arch, or the neck vessels. Venous penetration is more common in cases of peripheral migration.4,5 We were not able to determine angiographically the exact site of the vessel penetration, despite good-quality studies. Our hypothesis of arterial embolism is based on the facts that the patient had no skull penetration by any of the pellets, and he presented to our clinic a few weeks after the shooting and the stroke. This time interval may have given the artery enough time to heal, because the angiogram was performed almost 4 weeks after the accident. Of the 2 cases reported in the literature, in one there is no mention of any angiogram,6 and in the other the vertebral artery was angiographically normal.5
The symptoms of the embolism vary from asymptomatic to coma and death. Most patients present with acute symptoms. With the middle cerebral artery the most common site for the missile to be lodged, hemiparesis/hemiplegia and speech disturbances are the more frequently related symptoms.4,6–8 Delayed neurologic symptoms are reported, probably related to carotid dissection, emboli migration, or delayed thrombosis.1–4,8 Delayed cerebral embolism after shotgun wound to the chest has also been reported.4 In the 2 cases related with posterior circulation embolization, one patient died5 and the other was asymptomatic, being diagnosed years after a CT of the head was done for unrelated reasons.6 Our patient had an ischemic stroke related to the emboli but eventually made a good, functional recovery, despite some residual neurologic deficit.
The treatment of intracerebral arterial embolism is controversial. Arterial embolectomies have been performed by some authors,9 but the results have not been encouraging, as most patients already have an established infarct at the time of the treatment.4,8 Metallic pellets are not amenable to endovascular removal, because of the risk of intimal injury from the movement of the pellet on its way back to the internal carotid artery. Consequently, the limited surgical options remain arteriotomy and removal of the emboli.7,9 The option of surgical treatment faces, beyond the technical difficulties of performing a microembolectomy, the major problem of timing of the surgical intervention. In our opinion, there is no role for surgical intervention in established infarcts, and there is no evidence that a patient with asymptomatic intracranial emboli will develop symptoms if not treated with embolectomy. Most symptomatic patients presented either with acute neurologic symptoms or with delayed embolization and symptoms (acute in relationship with the time of the embolization).4–6,8 Although complications from the persistence of the pellet in the intracranial arterial tree are cited in the literature,10 we do not believe that there is sufficient evidence of benefit to support the indication of surgical treatment. The “evidence” in the literature is based on reviews of the available cases and comparison between a small number of patients treated conservatively and an even smaller number of patients treated surgically.7,9,10 In addition, a technically successful embolectomy does not necessarily mean a better prognosis.4 Conservative treatment has been suggested for asymptomatic patients, and patients with established infarcts or improving neurologic deficits. Based on the fact that the time from embolization to reperfusion is a great limiting factor for the success of the surgical treatment and that it has no role if we are dealing with an already infarcted area, we think that this is the best management option. Although the risk of leaving a pellet in the intracranial circulation has been mentioned, we do not believe that there is enough evidence to justify a procedure such as an embolectomy.4,5,7,8
References
- Received February 15, 2005.
- Accepted after revision March 3, 2005.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}
{kind=link}