
Abstract
SUMMARY: Moyamoya syndrome is the secondary form of intracranial arterial occlusive diseases that produces collateral vessels from the base of brain. We report a case of Moyamoya syndrome developing in association with Graves thyrotoxicosis; as a result of its rapid progression and severe global ischemia, it was ultimately fatal. Because of the rarity of this association, we reviewed the literature in an attempt to establish possible demographic and clinical characteristics that may suggest putative mechanisms of pathogenesis.
We report a case of Graves disease with thyroid storm associated with Moyamoya syndrome, which is particularly noteworthy because of a very rapid progression of the cerebrovascular occlusive disease that was ultimately fatal. The unusual aggressive nature of our case prompted us to review the literature in an attempt to establish possible demographic, clinical, and laboratory patterns that may help to eventually elucidate putative mechanisms of pathogenesis.
Case Report
A 40-year-old woman with a 6-month history of Graves disease underwent iodine-131 ablation of her thyroid gland, which was complicated by the development of acute “thyroid storm” 3 weeks after treatment. At that time, she presented to her local hospital with nausea, vomiting, tremors, and marked neck or throat pain. Her thyroid function tests were consistent with a marked hyperthyroid state (free thyroxine, 18 ng/dL; thyroid-stimulating hormone [TSH], 0.22 μM/mL). Her condition rapidly deteriorated during the next 2 days, when she complained of severe headaches and subsequently became progressively comatose and hypoxic, prompting intubation. A head CT showed multiple areas of cerebral ischemia that could not be attributable to a single vascular territory. Because of the known association of thyrotoxicosis and acute dural sinus thrombosis, the latter diagnosis was suspected, prompting emergent referral to our service for further evaluation and possible dural sinus thrombolysis.
On her arrival at our institution, the patient was comatose with a Glasgow Coma Scale score of 5. Her blood pressure was 210/110 mm Hg, and her heart rate was 97 beats/min and regular. The pupils were both 3 mm and equally reactive to light. Muscle tone was globally increased, and the deep tendon reflexes were symmetrically hyper-reflexic. Coagulation profile showed no significant abnormality (platelet count, 251 × 103/mm3; prothrombin time, 13 seconds; partial thromboplastin time, 23 seconds; international normalized ratio, 1.0). Immunoassay studies for autoantibodies were not performed. Another head CT, performed this time with contrast enhancement, showed multiple bilateral foci of low attenuation associated with loss of gray-white differentiation and sulcal effacement, most compatible with acute cerebral ischemia (Fig 1). The ischemic changes affected mostly the frontal and parietal lobes and seemed to be consistent with multiple arterial vascular territories. Because there was no evidence of thrombus within the major dural sinuses, the tentative diagnosis of acute dural sinus thrombosis was placed into question.

Axial cranial CT scans obtained with intravenous contrast enhancement (A, -B) show multiple areas of abnormal low attenuation, which are most dramatic within both frontal lobes as well as within the bilateral basal ganglia.
Emergent cerebral angiography was subsequently performed and showed unsuspected, severe bilateral basal arterial occlusive disease centered at the intracranial internal carotid arterial (ICA) terminus, with extension distally to involve the proximal middle cerebral artery (MCA) and anterior cerebral artery (ACA) territories (Fig 2). Only minimal antegrade flow of both MCA territories was seen, with significantly delayed transit time and incomplete visualization of distal cortical branches. Prominent collateral vessels were also seen emanating from both posterior cerebral arteries, and minimal basal perforator collateral vessels emerged from the lenticulostriate domain (Fig 3). No typical pufflike Moyamoya vessels were observed. The vertebrobasilar territory was normal, with the exception of some minor leptomeningeal collaterals seen along the corpus callosum, which inadequately reconstituted portions of the distal ACA territory.

The anteroposterior projections of bilateral internal carotid artery (ICA) angiography in early (A, right; -B, left) and late arterial phases (C, right; -D, left) and lateral projections of bilateral ICA angiography (E, right; -F, left) show nearly complete occlusion of the bilateral supraclinoid ICA as well as bilateral proximal segments of the ACAs and MCAs. Only minimal delay antegrade flows of the bilateral MCAs are noted. Collateral flows are seen from the posterior cerebral artery via the posterior choroidal plexus to the pericallosal artery.

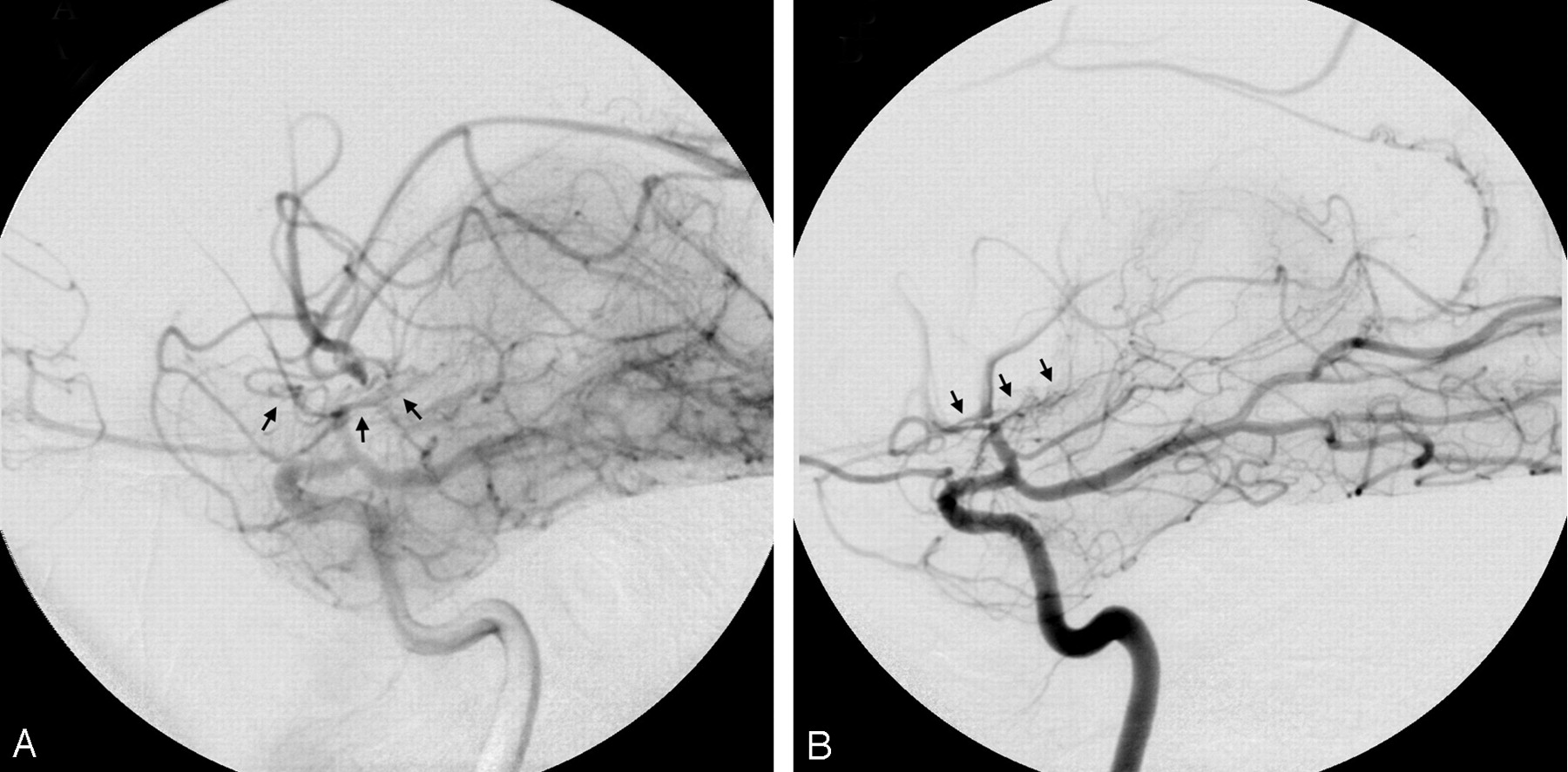
Magnified lateral projections of bilateral ICA angiography (A, right; -B, left) show only minimal collateral flows (arrows) from lenticulostriates over the base of brain, which reconstitute into the postocclusive or highly stenotic portions of the MCAs.
These angiographic findings were most compatible with the diagnosis of secondary Moyamoya phenomena or Moyamoya syndrome. The patient’s condition continued to deteriorate, and soon after undergoing angiography, the findings of her neurologic examination and electroencephalogram demonstrated brain death. She eventually died on the second hospital day after discontinuation of life support. A postmortem examination was unfortunately denied.
Discussion
Moyamoya disease is a cerebrovascular disorder of unknown cause, characterized by slowly progressive steno-occlusive disease that first involves both distal ICAs and eventually progresses to involve both proximal ACAs and MCAs. Abnormal collateral vasculature develops in response to this process, mostly derived from the basal lenticulostriates and thalamoperforators. The same slowly progressive occlusions of the anterior cerebral circulation with enlarged pathologic basal collaterals can be seen in association with other diseases, which have been alternatively defined as Moyamoya phenomenon or syndrome.1 Furthermore, Moyamoya syndrome has a more variable pattern of clinical presentation. Suzuki2 proposed that the secondary form of the disorder, which he described as “quasi-Moyamoya disease,” should be considered in any one of the following patterns that do not fulfill the original definition of primary Moyamoya disease: (1) unilateral involvement, (2) stenosis or occlusion of the proximal MCA with Moyamoya vessels, (3) association with an arteriovenous shunt surgery vascular malformation, and (4) other known associated conditions (eg, neurofibromatosis, sickle cell disease, Down syndrome, etc). Although several diseases may be putatively associated with Moyamoya syndrome (Table 1), a clear pathoetiologic link remains to be elucidated.
Summary of diseases associated with Graves disease and with Moyamoya syndrome
Graves disease is an autoimmune disorder in which TSH receptors are targeted by various autoantibodies, resulting in excessive production and release of thyroid hormones. The resultant hyperthyroid state produces multiorgan physiologic derangements. Rarely, Graves disease has been reported to occur in association with other diseases (Table 1). Moyamoya syndrome is one of the associations, with only 9 previous cases reported in the English literature. It has been presumed that there is some pathoetiologic linkage between these 2 disorders, although no specific mechanism has been elucidated. Certain salient features of these cases are summarized in Table 2.
Summary of reported cases of Moyamoya syndrome in association with Graves disease
The association of Graves disease with Moyamoya was first reported by Kushima et al,3 who documented 2 cases of patients presenting with clinical symptoms of thyrotoxicosis, subsequently followed by stroke. In 1 patient, 2 episodes of cerebral infarction occurred during clinical and laboratory evidence of hyperthyroid function. It is noteworthy that the patient’s neurologic symptoms were alleviated after normalization of thyrotoxicosis by antithyroid drug therapy. The second patient experienced left hemiparesis and motor aphasia after diagnosis of Graves disease. The patient underwent subtotal thyroidectomy for her recurrent thyrotoxicosis.
Another case, reported by Liu et al,4 was noted in a woman who experienced dysarthria and right facial and extremity weakness 5 months after being diagnosed with Graves disease and receiving standard antithyroid medication. Tendler et al5 subsequently described 2 more cases. One patient experienced acute onset of left-sided paresthesias and weakness 2 weeks after radioactive iodine therapy for her Graves thyrotoxicosis. An occlusion of the ICA terminus and a high-grade stenosis of the left supraclinoid ICA with Moyamoya vessels were found on conventional angiography. In the second instance, the patient was first diagnosed with Moyamoya syndrome approximately 10 years before developing symptoms of hyperthyroidism. However, she did not become neurologically symptomatic until she began medical treatment for her Graves thyrotoxicosis. Both patients in the report by Tendler et al received medical treatment and subtotal thyroidectomy.
The case reported by Leno et al6 concerned a patient with Down syndrome who experienced acute onset of left extremity weakness. He was found to be in a severe hyperthyroid state from Graves thyrotoxicosis at that time. A catheter angiogram revealed marked stenosis of his right supraclinoid ICA with Moyamoya collaterals. The patient in the case reported by Kim et al7 was diagnosed with Graves thyrotoxicosis during the later part of her pregnancy (31 weeks). Severe cardiomegaly with global hypokinetic wall movement of the heart and pulmonary edema were also noted. She subsequently developed a seizure, which prompted MR imaging and MR angiography of the brain. These studies showed areas of cerebral infarction secondary to either complete occlusions or severe stenoses of both supraclinoid ICAs, as well as an occlusion of left MCA.
More recently, Nakamura et al8 reported 2 additional cases with clinical presentations similar to those of the patients previously reported. The first patient was found to have cerebral infarction while she was in her thyrotoxicosis state and also had cardiomegaly and heart failure. The second patient was diagnosed with Graves disease 12 years before she experienced her ischemic neurologic symptoms. Both affected patients underwent surgical treatment for revasculization, and the first patient also received medical treatment for thyrotoxicosis.
All the patients in the previously reported cases, except one, are women. The clinical courses were relatively similar with the exception of the second patient in the series of Tendler et al,5 in which the original diagnosis of Moyamoya syndrome preceded the clinical onset of Graves disease by 10 years. However, all cases except one were associated with clinical and laboratory evidence of a significant hyperthyroid state (frequently occurring after initiation of treatment) that coincided with the onset of cerebral ischemic events. The thyroid function of 1 patient (the second patient in the series of Nakamura et al8) who was not in a significant hyperthyroid state was still in the upper limits of normal range. Most of the reported patients eventually recovered from their neurologic symptoms after completion of medical and/or surgical treatment.
Our case shows certain critical similarities to the previously mentioned reports. First, as seen in several of the other cases, our patient did not seem to become symptomatic from her Moyamoya syndrome until after the Graves disease was treated. Furthermore, as with all previous reports, our patient from both clinical and laboratory perspectives had a severe hyperthyroid status (in this case, so-called thyroid storm). Finally, as summarized in Table 1, our patient too had multifocal basal occlusive disease around the circle of Willis (bilateral distal ICAs, proximal ACAs, and MCAs) that was well documented by conventional angiography. An important difference between our case and all other reported cases is that the former manifested as an extremely rapid and fulminant clinical course that was ultimately fatal. We believe that this patient certainly shared a similar patholoetiology with the other patients but had a very rapid clinical course. To our knowledge, this is indeed the first fatal case of Moyamoya syndrome associated with Graves thyrotoxicosis. It is unfortunately difficult to hypothesize the reason for this poor outcome, other than the observation that our patient seemed not to have had adequate Moyamoya vessels and leptomeningeal collaterals, as documented on the cerebral angiogram.
On the basis of these limited observations, it would seem that the development of a significant thyrotoxic state, particularly after initiation of therapy, might be a risk factor for at least the symptomatic manifestation of Moyamoya syndrome, though a direct patholoetiologic linkage is also quite possible. Certainly, one plausible mechanism for producing acute ischemic symptoms is the production of significant alterations in cerebrovascular hemodynamic, either directly or indirectly from the excess release of thyroid hormone. This can derive from a variety of putative mechanisms that can alter cerebral perfusion or increase cerebral metabolic demand and has led one group to recommend that abrupt surges of thyroid hormone levels as a consequence of treatment in such association should be avoided,3 particularly when using radioactive iodine ablation, which may be more prone to cause these surges.
In terms of finding a direct patholoetiologic linkage, we could hypothesize that an autoimmune mechanism is responsible. The most plausible possibility is a cross-reactivity of the TSH receptor antibodies with yet-to-be-elucidated antigens derived from cerebral arteries, resulting in an immune-mediated arteritis. Leno et al6 were the first to point out this possible autoimmune mechanism, though no specific laboratory evidence was offered. Tendler et al5 suggested that although more definitive proof is needed, there is considerable evidence that an “aggressive autoimmune mechanism” is involved with this association.
Clearly, other disorders associated with Moyamoya syndrome have well-established autoimmune mechanisms of pathogenesis or are associated with an arteritis that affects the cerebral arteries. Such diseases include systemic lupus erythematosus, antiphospholipid syndrome, ulcerative colitis, tuberculosis, leptospirosis, and postradiation arteritis. Even seemingly “nonvasculitic” diseases may have an autoimmune pathoetiologic linkage, as suggested with Down syndrome, which has long been known to be associated with Moyamoya syndrome. Interestingly, thyroid dysfunction is a manifestation of Down syndrome, which has been, at least in part, hypothesized to be attributable to a relatively high prevalence (39.3%) of potentially broad-reacting autoantibodies.9 Although these observations strengthen a putative pathoetiologic mechanism of autoimmune arteritic cross-reactivity, which ultimately results in the characteristic histopathologic changes of Moyamoya syndrome, definitive proof still requires both the isolation of the specific causative autoantibodies and better elucidation of the specific cellular and molecular mechanisms responsible for the progressive occlusive arteriopathy that is characteristic of the syndrome.
Conclusion
Moyamoya syndrome could occur in association with Graves disease, through presumably a yet-to-be-defined pathoetiologic link. In reviewing the literature, we believe that almost all cases seem to be coincident with a significant hyperthyroid state, most commonly occurring shortly after initiation of therapy. Affected persons typically have multifocal basal occlusive disease of the circle of Willis and may clinically improve after completion of antithyroid therapy. However, as seen in our patient, a fulminant course may occur. Graves disease should be considered in the differential diagnosis for pathoetiologic mechanisms associated with Moyamoya syndrome.
Footnotes
Presented in the section of Excerpta Extraordinaire at the 41st Annual Meeting of the American Society of Neuroradiology, Washington, DC, April–May 2003.
References
- Received April 8, 2005.
- Accepted after revision May 6, 2005.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}
{kind=link}