
Article Figures & Data
Figures
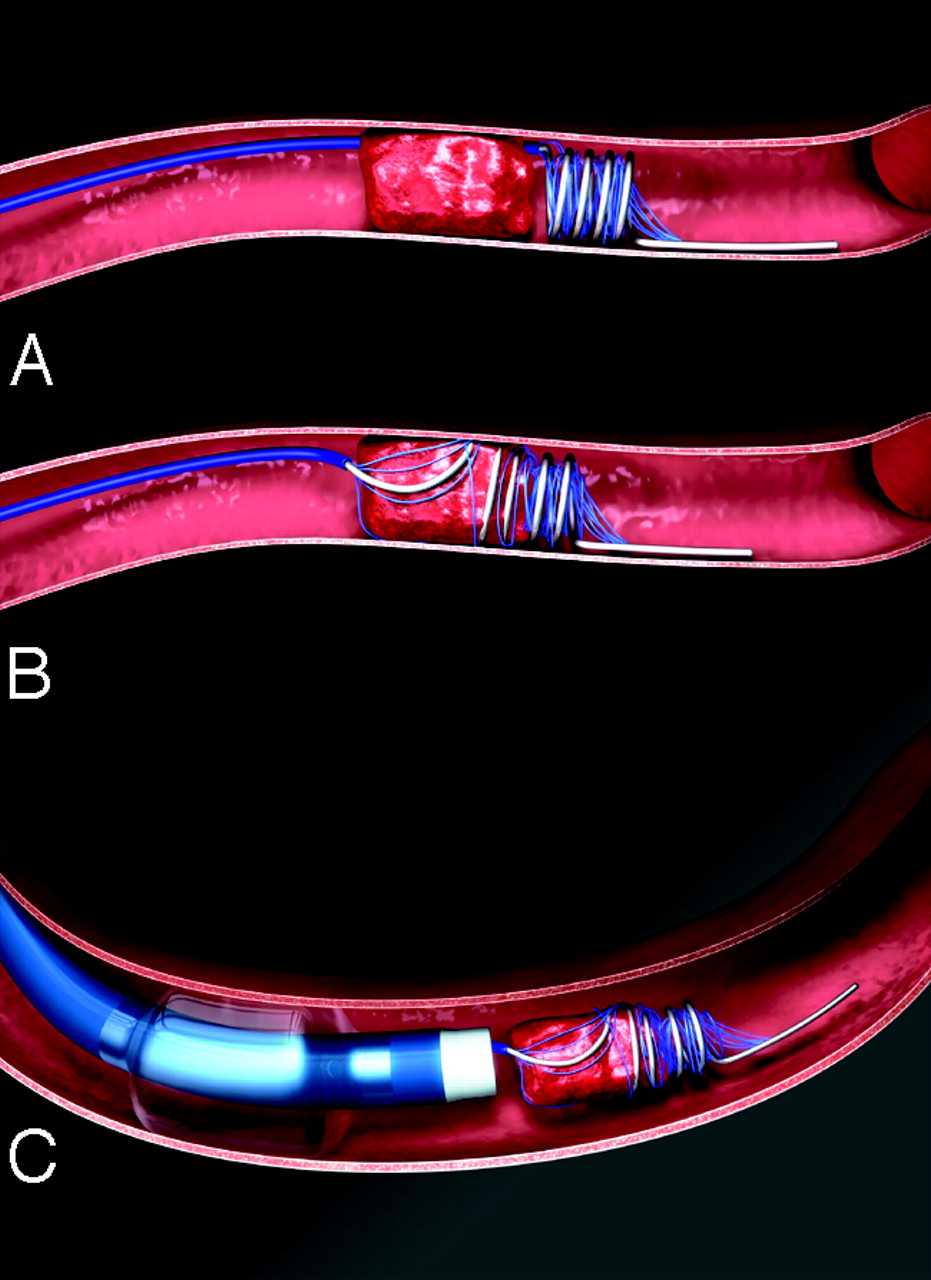
- Fig 1.
Illustration of the L5 thrombectomy device removing thrombus. The L5 device is a helix of flexible nitinol wire with an arcade of filaments secured to the loops of the helix. This differs from the X5 and X6 Merci Retrievers by having filaments and no taper to the coils. Within 8 hours of acute ischemic stroke, the balloon guide catheter is placed via femoral artery into the proximal internal carotid or vertebral artery. The blue microcatheter is advanced through the balloon guide catheter and placed through the occlusion using a microguidewire. The guidewire is then exchanged for the Retriever, which is advanced distal to the clot and several loops are deployed (A). The device is further deployed so as to fully ensnare the clot (B). Then, the proximal balloon of the guide is inflated to prevent distal embolization, some torquing maneuvers are applied, and the microcatheter and Retriever are withdrawn together to retrieve the clot (C).
- Fig 2.
Multi MERCI patient flow and primary outcomes. Recanalization is from device alone; final recanalization is after Retriever and any adjuvant therapy. Patients with symptomatic intracranial hemorrhage (ICH), and procedural complications may overlap.


Tables
Variable Overall (N = 111) IV tPA (N = 30) No IV tPA (N = 81) P Value Age, y (mean ± SD) 66.2 ± 17.0 65.4 ± 13.5 66.5 ± 18.2 .772† Female, % 56.8% 56.7% 56.8% >.99‡ Baseline NIHSSS* (mean ± SD) 19.0 ± 6.3 19.6 ± 4.3 18.8 ± 6.9 .565† Hours to device treatment, median (range) 4.2 (1.3–17.3) 3.6 (2.1–7.0) 4.4 (1.3–17.3) .072§ Procedure length (h), median (range) 1.6 (0.5–5.8) 1.6 (0.6–3.3) 1.7 (0.5–5.8) .353§ No. of passes (mean ± SD) 2.8 ± 1.6 2.7 ± 1.7 2.8 ± 1.6 .460§ IV tPA, N (%) 30 (27.0) 30 (100) 0 (0) – IA tPA postretriever, N (%) 43 (38.7) 13 (43.3) 30 (37.0) .661‡ Vascular occlusion location, N (%) .296¶ ICA 1 (0.9) 1 (3.3) 0 (0) ICA-T 32 (28.8) 10 (33.3) 22 (27.2) MCA 68 (61.3) 18 (60.0) 50 (62.0) Vertebral alone 0 0 0 Vertebral + basilar, basilar 9 (8.1) 1 (3.3) 8 (9.9) P1 1 (0.9) 0 (0) 1 (1.2) Note:—IV tPA indicates intravenous tissue-type plasminogen activator; NIHSSS, National Institutes of Health Stroke Scale score; IA, intraarterial; ICA, intracranial carotid artery; ICA-T, ICA terminal bifurcation; MCA, middle cerebral artery.
* One posterior circulation (distal basilar artery occlusion) patient was enrolled against protocol with a baseline NIHSS score of 4. No other patients had a baseline NIHSS score below the required protocol score of 8. Procedure length was the time from groin puncture to final angiogram.
† t Test.
‡ Fisher exact test.
§ Wilcoxon rank-sum test.
¶ Likelihood ratio χ2 test.
No. IV tPA dose (mg/kg) IA tPA dose (mg) Total tPA Dose (mg) Total tPA dose (mg/kg) IV tPA only 17 0.68 ± 0.14 52.6 ± 17.3 0.68 ± 0.14 Lower dose 12 0.60 ± 0.04 45.0 ± 8.97 0.60 ± 0.04 Regular dose 5 0.88 ± 0.03 70.9 ± 19.5 0.88 ± 0.03 IA tPA only 27 14.0 ± 9.65 14.0 ± 9.65 0.19 ± 0.14 IA + IV tPA 13 0.67 ± 0.17 7.54 ± 3.91 69.3 ± 12.5 0.76 ± 0.17 Lower dose 7 0.53 ± 0.05 8.87 ± 4.67 64.4 ± 8.74 0.61 ± 0.04 Regular dose 6 0.85 ± 0.06 6.00 ± 2.28 74.9 ± 14.5 0.93 ± 0.08 Note:—IV indicates intravenous; IA, intraarterial; tPA, tissue plasminogen activator.
Doses are shown as means ± SD; 3 patients each received 250,000 U of urokinase IA and IV tPA (not shown).
Result Overall (N = 111) IV tPA (N = 30) No IV tPA (N = 81) P Value* Revascularization postretriever, N (%) 60 (54.1) 16 (53.3) 44 (54.3) >.99 Revascularization postadjuvant, N (%) 77 (69.4) 22 (73.3) 55 (67.9) .649 mRS ≤2 at 90 d, N (%)† 37 (34.3) 10 (33.3) 27 (34.6) >.99 Mortality at 90 d, N (%)† 33 (30.6) 8 (26.7) 25 (32.1) .647 Intracranial hemorrhage Symptomatic ICH,‡ N (%) 10 (9.0) 2 (6.7) 8 (9.9) .726 Asymptomatic ICH,§ N (%) 33 (29.7) 12 (40) 21 (25.9) .166 Procedure-related serious adverse events, N (%) 11 (9.9) 0 (0) 11 (13.6) .034 Dissection 3 (2.7) 0 3 (3.7) .562 Perforation¶ 3 (2.7) 0 3 (3.7) .562 Embolization of a previously uninvolved vessel 1 (0.9) 0 1 (1.2) >.99 Groin complications 0 0 0 Symptomatic ICH not associated with perforation‖ 3 (2.7) 0 3 (3.7) .562 Asymptomatic SAH associated with death 1 (0.9) 0 1 (1.2) >.99 Clinically significant procedure complications, N (%) 5 (4.5) 0 (0) 5 (6.2) .321 Note:—IV tPA indicates intravenous tissue plasminogen activator; mRS, modified Rankin score; ICH, intracranial hemorrhage; SAH, subarachnoid hemorrhage.
* Fisher exact test.
† N = 108 (data not available at 90 days in 3 patients in the no IV tPA group).
‡ Includes 3 patients with symptomatic SAH, all within the no IV tPA group. Symptomatic hemorrhage includes 6 hemorrhages adjudicated as evolution of the primary stroke and 4 that were adjudicated as procedure-related as detailed below.
§ Includes 8 patients with asymptomatic SAH; 4 were in the IV tPA group and 4 were in the IV tPA group.
¶ One perforation lead to symptomatic hemorrhage.
‖ Patients in whom the symptomatic ICH was either caused by the procedure or the procedure could not be ruled out as the cause of the hemorrhage.
Result No Major Protocol Violations (N = 73) Major Protocol Violation(s) (N = 38)* P Value† Procedure-related serious adverse events, N (%) 4 (5.5) 7 (18.4) .044 Intracranial hemorrhage Symptomatic ICH†, N (%) 7 (9.6) 3 (7.9) >.99 Symptomatic SAH, N (%) 2 (2.7) 1 (2.6) >.99 Asymptomatic ICH, N (%) 20 (27.4) 13 (34.2) .514 Asymptomatic SAH, N (%) 3 (4.1) 5 (13.1) .120 mRS ≤2 at 90 d, N (%)† 24 (33.3) 13 (36.1) >.99 Mortality at 90 d, N (%)† 20 (27.8) 13 (36.1) .514 Note:—ICH indicates intracranial hemorrhage; SAH, subarachnoid hemorrhage; mRS, modified Rankin score.
* Protocol violations are tabulated per patient.
† Fisher exact test.
‡ N = 72 in no protocol violations group and 36 in the protocol violation group at 90 days.
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Cardioembolic Stroke: A Case Study
- Predictors of poor outcome despite recanalization: a multiple regression analysis of the NASA registry
- Scientific Rationale for the Inclusion and Exclusion Criteria for Intravenous Alteplase in Acute Ischemic Stroke: A Statement for Healthcare Professionals From the American Heart Association/American Stroke Association
- Impact of the ASPECT scores and distribution on outcome among patients undergoing thrombectomy for acute ischemic stroke
- Embolectomy for stroke with emergent large vessel occlusion (ELVO): report of the Standards and Guidelines Committee of the Society of NeuroInterventional Surgery
- Clinical, angiographic and radiographic outcome differences among mechanical thrombectomy devices: initial experience of a large-volume center
- Evolution of thrombectomy approaches and devices for acute stroke: a technical review
- Flexible tip guides and intermediate catheters: two center experience and a proposed taxonomy
- Hounsfield unit value and clot length in the acutely occluded vessel and time required to achieve thrombectomy, complications and outcome
- Imaging and Treatment of Patients with Acute Stroke: An Evidence-Based Review
- Addressing challenges in 4 F and 5 F arterial access for neurointerventional procedures in infants and young children
- Optimal Perfusion Computed Tomographic Thresholds for Ischemic Core and Penumbra Are Not Time Dependent in the Clinically Relevant Time Window
- Importance of Cerebral Artery Recanalization in Patients With Stroke With and Without Neurological Improvement After Intravenous Thrombolysis
- Endovascular therapy yields significantly superior outcomes for large vessel occlusions compared with intravenous thrombolysis: is it time to randomize?
- Recommendations on Angiographic Revascularization Grading Standards for Acute Ischemic Stroke: A Consensus Statement
- Alberta Stroke Program Early CT Scale Evaluation of Multimodal Computed Tomography in Predicting Clinical Outcomes of Stroke Patients Treated With Aspiration Thrombectomy
- Mechanical thrombectomy as the primary treatment for acute basilar artery occlusion: experience from 5 years of practice
- Incomplete mechanical recanalization of middle cerebral artery occlusions facilitates endogenous recanalization within 5 h
- Guidelines for the Early Management of Patients With Acute Ischemic Stroke: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association
- Pre-intervention triage incorporating perfusion imaging improves outcomes in patients undergoing endovascular stroke therapy: a comparison with the device trials
- Subarachnoid Hemorrhage in a Multimodal Approach Heavily Weighted Toward Mechanical Thrombectomy With Solitaire Stent in Acute Stroke
- Factors Influencing Clinically Meaningful Recanalization after IV-rtPA in Acute Ischemic Stroke
- National Trends in Utilization and Outcomes of Endovascular Treatment of Acute Ischemic Stroke Patients in the Mechanical Thrombectomy Era
- Use of the Outreach Distal Access Catheter for Microcatheter Stabilization during Intracranial Arteriovenous Malformation Embolization
- Revascularization grading in endovascular acute ischemic stroke therapy
- Merci mechanical thrombectomy retriever for acute ischemic stroke therapy: Literature review
- Angioplasty and stenting for mechanical thrombectomy in acute ischemic stroke
- Endovascular comprehensive stroke center designation parameters
- Use of neuroimaging to guide the treatment of patients beyond the 8-hour time window
- Timing, testing, and standardization of endovascular therapy
- The Penumbra system for mechanical thrombectomy in endovascular acute ischemic stroke therapy
- Periprocedural antithrombotic strategies in acute ischemic stroke interventional therapy
- Interventional Stroke Therapies in the Elderly: Are We Helping?
- Thrombus Branching and Vessel Curvature Are Important Determinants of Middle Cerebral Artery Trunk Recanalization With Merci Thrombectomy Devices
- Quantitative Evaluation of C-Arm CT Cerebral Blood Volume in a Canine Model of Ischemic Stroke
- Clinical and MRI Predictors of No Early Recanalization Within 1 Hour After Tissue-Type Plasminogen Activator Administration
- Mechanical Thrombectomy in Acute Ischemic Stroke: Catch Device
- A Cost-Utility Analysis of Mechanical Thrombectomy as an Adjunct to Intravenous Tissue-Type Plasminogen Activator for Acute Large-Vessel Ischemic Stroke
- Patient Outcomes With Endovascular Embolectomy Therapy for Acute Ischemic Stroke: A Study of the National Inpatient Sample: 2006 to 2008
- Use of the Outreach distal access catheter as an intracranial platform facilitates coil embolization of select intracranial aneurysms: technical note
- CT and MRI Early Vessel Signs Reflect Clot Composition in Acute Stroke
- Partial recanalization of concomitant internal carotid-middle cerebral arterial occlusions promotes distal recanalization of residual thrombus within 24 h
- Acute Stroke Intervention
- Is Mechanical Clot Removal or Disruption a Cost-Effective Treatment for Acute Stroke?
- Effect of Baseline CT Scan Appearance and Time to Recanalization on Clinical Outcomes in Endovascular Thrombectomy of Acute Ischemic Strokes
- Predictors of Subarachnoid Hemorrhage in Acute Ischemic Stroke With Endovascular Therapy
- Solitaire Flow-Restoration Device for Treatment of Acute Ischemic Stroke: Safety and Recanalization Efficacy Study in a Swine Vessel Occlusion Model
- Predicting Long-Term Outcome after Endovascular Stroke Treatment: The Totaled Health Risks in Vascular Events Score
- Safety of performing CT angiography in stroke patients treated with intravenous thrombolysis
- Endovascular Thrombectomy for Acute Ischemic Stroke in Failed Intravenous Tissue Plasminogen Activator Versus Non-Intravenous Tissue Plasminogen Activator Patients: Revascularization and Outcomes Stratified by the Site of Arterial Occlusions
- In Vivo Evaluation of the Phenox CRC Mechanical Thrombectomy Device in a Swine Model of Acute Vessel Occlusion
- Clinical Outcomes in Middle Cerebral Artery Trunk Occlusions Versus Secondary Division Occlusions After Mechanical Thrombectomy: Pooled Analysis of the Mechanical Embolus Removal in Cerebral Ischemia (MERCI) and Multi MERCI Trials
- Drip, Ship, and Retrieve: Cooperative Recanalization Therapy in Acute Basilar Artery Occlusion
- Equipoise among recanalization strategies
- Occurrence and Predictors of Futile Recanalization following Endovascular Treatment among Patients with Acute Ischemic Stroke: A Multicenter Study
- Good clinical outcome after ischemic stroke with successful revascularization is time-dependent
- Percutaneous Transluminal Angioplasty and Stent Placement in Acute Vessel Occlusion: Evaluation of New Methods for Interventional Stroke Treatment
- Mechanical Approaches Combined With Intra-Arterial Pharmacological Therapy Are Associated With Higher Recanalization Rates Than Either Intervention Alone in Revascularization of Acute Carotid Terminus Occlusion
- Identifying Patients at High Risk for Poor Outcome After Intra-Arterial Therapy for Acute Ischemic Stroke
- Endovascular Approaches to Acute Stroke, Part 2: A Comprehensive Review of Studies and Trials
- Endovascular Approaches to Acute Stroke, Part 1: Drugs, Devices, and Data
- Intra-Arterial Stroke Therapy: An Assessment of Demand and Available Work Force
- Endovascular Therapy for Acute Ischemic Stroke
- Thrombus Burden Is Associated With Clinical Outcome After Intra-Arterial Therapy for Acute Ischemic Stroke
- Interventional Acute Ischemic Stroke Therapy With Intracranial Self-Expanding Stent
- Haemorrhagic transformation in acute ischaemic stroke following thrombolysis therapy: classification, pathogenesis and risk factors
- Staged Escalation Therapy in Acute Basilar Artery Occlusion: Intravenous Thrombolysis and On-Demand Consecutive Endovascular Mechanical Thrombectomy: Preliminary Experience in 16 Patients
- Mechanical Thrombectomy for Acute Ischemic Stroke: Final Results of the Multi MERCI Trial
- Mechanical Thromboembolectomy for Acute Ischemic Stroke: Comparison of the Catch Thromboectomy Device and the Merci Retriever In Vivo
- Current Treatment of Peripheral Arterial Disease: Role of Percutaneous Interventional Therapies
- Intravenous or Intra-Arterial Thrombolysis?: It's Time to Find the Right Approach for the Right Patient
- The Interventional Management of Stroke (IMS) II Study
- Self-Expanding Stents for Recanalization of Acute Cerebrovascular Occlusions
- Mechanical Thrombectomy of Intracranial Internal Carotid Occlusion: Pooled Results of the MERCI and Multi MERCI Part I Trials
- Advances in Interventional Neuroradiology 2006
- Intra-Arterial Thrombolytic Therapy for Acute Basilar Occlusion: Pro
- Intracranial Hemorrhage Associated With Revascularization Therapies